
Translate this page into:
A study of changing trends in consumer preferences and perspectives towards health-care services during the pandemic
 , Lucklin Medimpudi2, Lakshmana Rao Ayyagari2, Jeswanth Araveti3, Mahesh Kadiri4
, Lucklin Medimpudi2, Lakshmana Rao Ayyagari2, Jeswanth Araveti3, Mahesh Kadiri4
*Corresponding author: Srikanth Medimpudi, Department of Diabetology, Dr. Srikanth’s Diabetes Specialities Centre, Vijayawada, Andhra Pradesh, India. drmsrikanth@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Medimpudi S, Medimpudi L, Ayyagari LR, Araveti J, Kadiri M. A study of changing trends in consumer preferences and perspectives towards health-care services during the pandemic. Indian J Physiol Pharmacol 2022;66:168-74.
Abstract
Objectives:
The novel coronavirus disease 2019 (COVID-19) pandemic has caused a turmoil in the health-care delivery system and challenged consumers’ sense of well-being. This study examines the evolving consumer expectations and explores the key interventions that health-care providers can employ to increase engagement with consumers and prepare organisations to cope with post-pandemic challenges.
Materials and Methods:
We conducted a cross-sectional survey of 715 randomly selected patients visiting three secondary diabetes care centres across Andhra Pradesh – Vijayawada, Tenali and Tirupati between December 2020 and January 2021. We collected participants demographic data and history of comorbidities.
Results:
During lockdown, 59.3% of the respondents were concerned about health management, 63.9% expressed fear of contracting infections while visiting hospitals. Majority (70%) did not prefer visiting hospitals treating COVID-19 patients, while 18.3% reluctantly consider only if COVID-19 ward was kept isolated. Measures such as wearing personal protective equipment sanitisation and thermal screening and social distancing in outpatient settings/waiting areas were demanded by 89.7%, 84.5% and 60% of respondents, respectively. Concurrently, there is an increasing trend (from 2.8% to 24.9%) in teleconsultation. About 31.7% show an inclination to continue teleconsultations even after COVID-19 era with 51.7% recognising telemedicine as a time-saving option. Among interested patients (54%) with no prior experience of telemedicine, 41.5% reported concerns due to lack of technical equipment and improper training. About 23.1% were skeptical of effective personalised treatment. Sample collections at home (75.3%), home monitors (63.3%), medication delivery (47.3%) and telemedicine (31.7%) are preferred choices.
Conclusion:
On a real-time basis, participants are willing to share their health status-related data with their health-care team. Succumbing to the worldwide COVID-19 experience, both health-care providers and patients need to adopt and devise a ‘new normal’, a paradigm for addressing both health-care providers’ and patients’ requirements.
Keywords
COVID-19 Pandemic
Consumer behaviour
Health care
Safety protocols
Telemedicine

INTRODUCTION
The novel coronavirus disease 2019 (COVID-19) pandemic had brought the turmoil of the health-care delivery system challenging the consumers’ sense of health-care seeking behaviour. Globally, there have been a several million COVID-19 deaths, reported by the World Health Organisation. The global unrest due to unavailability of specific treatment, limited availability of hospital beds[1,2] and other public places[3] the virus being a super spreader continues to prevail despite numerous measures have been taken to contain the infection. The lack of preparedness leading to poor management of chronic conditions including diabetes, hypertension[4-6] due to the inadequate telemedicine facilities and home healthcare services during the lockdown contributed to several mishaps during the first and second wave of COVID infections.
Increasing the awareness of the prevailing pandemic has led to an exponential growth in health literature and strategies to encourage individual responsibilities of their personal health management. Concurrently, growing demands for virtual consultation, implementation of feasible heath technologies to be accessed from home, favourable transformation of privacy policies is evidenced.[7,8]
The release of telemedicine guidelines by the Government of India, coupled with reducing resistance among medical practitioners to virtual consultations, has accelerated the adoption of teleconsultations to a certain extent.[9] The user base for telemedicine has increased during the lockdown.[7] The present and the future will witness a revolutionary change from the traditional approaches in the health-care delivery fuelled by a growing interest in telemedicine. This will further augment the invention and implementation of novel long-term measures including home collection of diagnostic samples and home delivery of regular drugs, regular monitoring of health status and real-time sharing of data with health-care professionals, fitness tracking and timely order refills.
Pandemic brought a sudden and significant drop in nonCOVID-19 patients seeking urgent medical attention.[8] On the other hand, people are experiencing health-related anxiety and worry about managing their health during the lockdown and are hesitant to visit health-care institutions for fear of contracting the virus themselves or spreading it to others. Hospitals are taking a range of safety measures to minimise their patients’ fears, such as using plex glass dividers, testing patients in advance, checking body temperature, distributing disinfectant wipes and ensuring the use of face masks. Based on our observations during COVID times, although hospitals have been periodically enhancing safety measures, they still advise patients with mild symptoms to opt for telehealth services to determine whether a hospital visit is required. Patients are either advised online or asked to visit the hospitals with all the necessary precautions in place based on the need. Today, consumers are making decisions on what type of facility to visit based on the extent of stringent precautionary protocols followed by the facility. In light of all this, the sector has had to continuously innovate and introduce new ways of taking care of patients. Health-care organisations must remain committed to understanding consumers during this turbulent time. Understanding consumer behaviour is a priority for health-care providers. The health-care ecosystem can use this research to develop multifaceted strategies and continue to thrive post-COVID-19 by exploring new settings and delivery channels across all spheres of care. We used our study to gauge consumer behaviour and understand the consumer preferences and expectations from health-care providers regarding care settings and safety protocols, adoption and use of virtual health channels, apps and at-home self-diagnostic and monitoring tests.
Further, the study explores the key interventions that health-care providers can employ to increase engagement with consumers and to prepare organisations to cope with post-pandemic challenges.
MATERIALS AND METHODS
A questionnaire-based survey study was conducted among patients visiting three secondary diabetes care centres in Andhra Pradesh – Vijayawada, Tenali and Tirupati during 2 months from December 2020 to January 2021.
All participants provided informed consent to take part in the study. Consecutive diabetes patients across all socioeconomic strata, educational levels and gender were included in the study to investigate consumer perceptions, behaviours and expectations regarding care settings and safety protocols. Children or students aged under 18 years, people with cognitive disorders and health-care practitioners were excluded from the sample. All the participants gave informed consent. In addition, each ‘consumer’s baseline demographic, including age, sex, location (urban/rural), annual household income (≤ Rs. 100,000 or > Rs. 100,000), education (illiterate, School/ high school, college and university) and any comorbidities were recorded using researcher-administered questionnaire. Further, information was obtained on consumer concerns about health-care facilities’ health management and safety expectations, preferences for visiting hospitals during the pandemic, preferences for diagnostic tests and reasons for and against the use of telemedicine. The questionnaire was pre-evaluated in ten non-study patients as a sample study before administering it to the study patients and minimal changes were made before standardisation.
Statistical analysis
The data were collated using Microsoft Excel sheet and SPSS software. All categorical variables are presented as proportions and descriptive variables are presented as mean ± standard deviation (S.D.). Data representation images were done using GraphPad Prism v 9.0.
RESULTS
A total of 715 subjects randomly selected from secondary diabetes care centres in Vijayawada, Tenali and Tirupati in Andhra Pradesh, India, were enrolled. The demographic and clinical characteristics of the study subjects are shown in [Table 1].
| Characteristics of the study subjects n=715 | n(%) |
|---|---|
| Age (years) Mean±SD | 51.8±10.1 |
| Gender, n(%) | |
| Male | 422 (59) |
| Female | 293 (41) |
| Location, n(%) | |
| Rural (n=345) | 345 (48.3) |
| Urban (n=370) | 370 (51.7) |
| Annual Income, n(%) | |
| ≤Rs. 100000 | 253 (35.4) |
| >Rs. 100000 | 462 (64.6) |
| Education, n(%) | |
| Illiterate | 161 (22.5) |
| Elementary School | 108 (15.1) |
| High School | 191 (26.7) |
| College | 140 (19.6) |
| University | 115 (16.1) |
| Number of Chronic Ailments, n (%) | |
| <2 | 241 (33.7) |
| ≥2 | 474 (66.3) |
The mean age was 51.8 ± 10.1 years and the most of the consumers attended the centres for their diabetes care and other chronic ailments [Table 1]. Most patients were hailing from urban areas (51.7%). Less than one-fourth of the participants were illiterates and the rest had at least graduated from high school. About 35.4% had an annual household income of Rs.100,000 or less. On an average, many of the study participants had at least three other coexisting conditions including hypertension or dyslipidaemia or overweight. About 66% (474/715) of the respondents had two or more underlying medical conditions.
Embracing the current threat due to the COVID-19 pandemic, about 64% (457/715) of respondents expressed fear of visiting hospitals [Figure 1a]. About one in ten participants (12.9%) were in a state of dilemma with respect to whether to visit hospitals during the pandemic. Despite this inherent scepticism with hospital visits, more than half the respondents 59.3% (424/715) acknowledged that health management was a major concern during the COVID-19 lockdown [Figure 1b]. Around 13.4% of participants were not sure of their concern for health management.
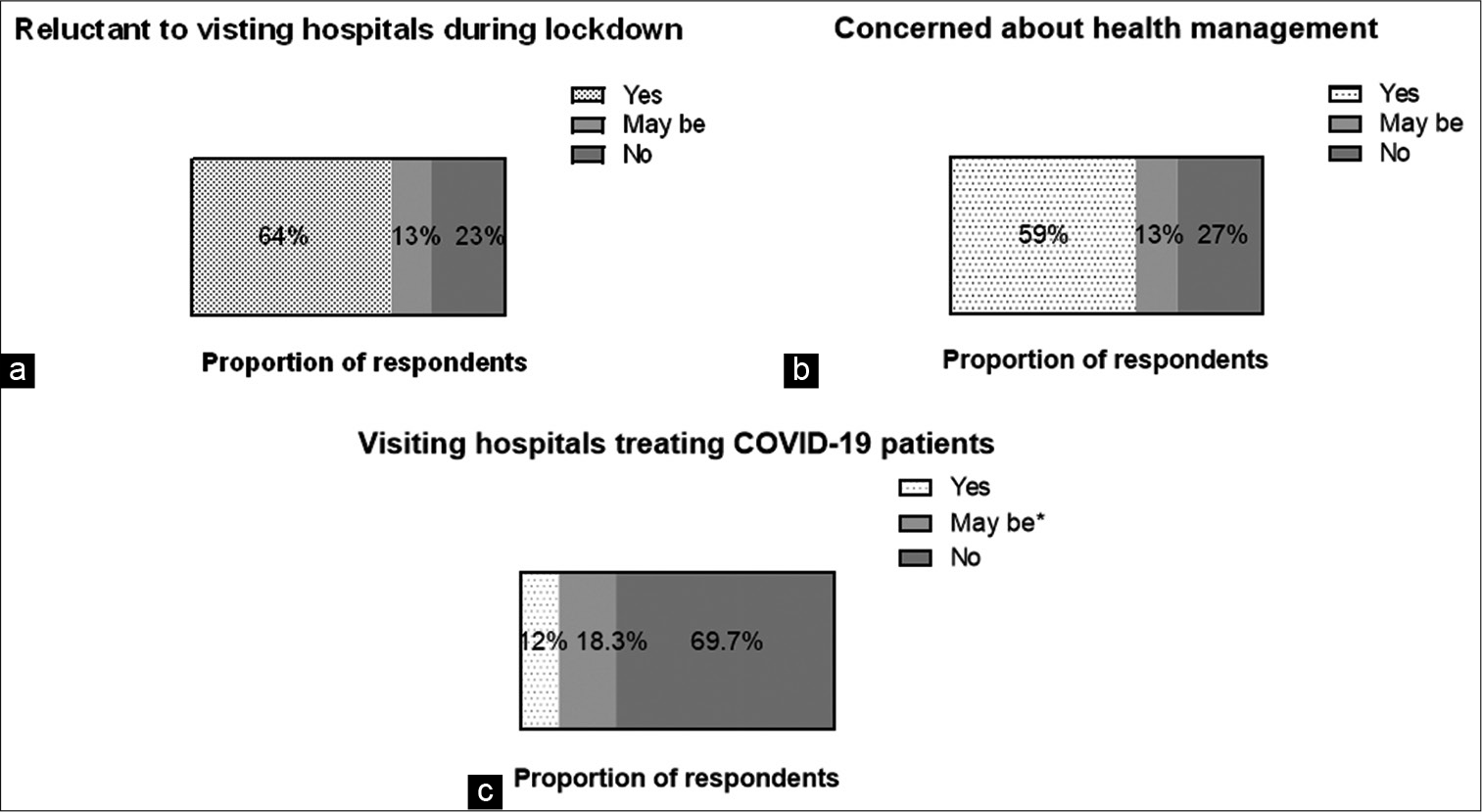
- (a-c) Consumer concerns and preferences of health management during the pandemic.
This study showed that about 69.7% (498/715) respondents prefer visiting hospitals, not treating COVID-19 patients [Figure 1c]. About 18.3% (131/715) of them were willing to consider visiting hospitals or institutions that treat COVID-19 patients for their routine health check-up visits, only if COVID-19 patients were treated in separate buildings.
Regarding the adherence of stringent safety protocols followed by institutions to evade spread of COVID infections, some factors are more regarded as more important than others [Table 2]. Around 89.7% (641/715) have expected their hospital staff to wear personal protective equipment. In addition, more than 84.5% (604/715) of respondents expect sanitisation and thermal screening at all entry and exit points of the health-care setting. About 60% (427/715) of respondents support social distancing and believe there should be a limit on how many people can be in an outpatient department/waiting area. About 49% (350/715) of respondents expect the hospital facility to provide disposable masks and gloves to all patients and visitors. Separate fever clinics and separate entry, exit and waiting areas for patients with fever/cold/cough were deemed a vital safety measure by 48.2% (345/715) of consumers. Hardly 33.1% (237/715) are in favour of a digital/paperless environment, including online medical records, cashless payments and more.
| Safety protocols | % |
|---|---|
| Hospital staffs use of personal protective equipment | 89.7 |
| Sanitisation and thermal screening at all entry and exit gates | 84.5 |
| Social distancing measures in OPD/waiting areas with an effort to limit the crowding | 60 |
| Patients and visitors offered disposable masks. Gloves provided by the hospital/laboratory | 49 |
| Isolated fever clinics and separate entry, exit and waiting areas for patients with fever/cold/cough | 48.2 |
| Working in a digital and paperless environment | 33.1 |
In our study, 75.1% of consumers (537/715) have never used telemedicine platforms [Figure 2a]. However, throughout the lockdown, the number of users for telemedicine has surged from 2.8% to 24.9% [Figure 2a]. In addition, around 54% (291/537) of respondents, who had never tried telemedicine before, expressed an inclination towards using telemedicine now [Figure 2b]. About 13.7% (98/715) experienced a decline in their telemedicine usage after the lockdown [Figure 2c]. Compared to pre-COVID-19, 70.6% (505/715) of consumers said their telemedicine usage was unchanged in the unlocking phase, while 15.7% (112/715) reported an increase.
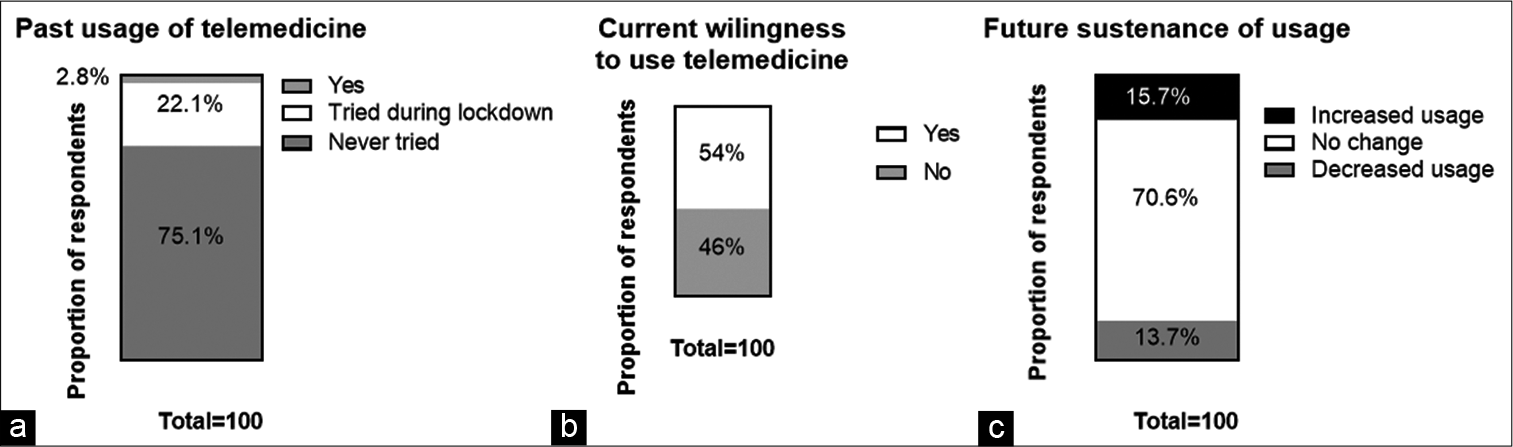
- (a-c) Usage of telemedicine.
The majority of those who tried telemedicine before or during the lockdown said that they did so to save time [Table 3]. About 51.7% (92/178) cited time savings as their top reason for preferring it. About 32.6% (58/178) tried telemedicine to slow the spread of infection, while 14.6% (26/178) used it to maintain pre-existing relationships with family doctors. There were two respondents that used telemedicine for reimbursement or insurance claims. In addition, inadequate assessment, technical training and equipment and physician resistance were major concerns among respondents. Of the respondents who have never used telemedicine, 41.5% (223/537) cited lack of equipment such as smart phones, laptops and training to use them as a key concern. Most respondents still believe in the traditional benefits of in-person healthcare. Around 23.1% (124/537) expressed those consultations without in-person examination would be ineffective and 21.4% (115/537) point to physician resistance. Data privacy was mentioned as a concern by 14% of respondents (75/537) [Table 3].
| Variables | Proportion of respondents (%) |
|---|---|
| Reasons opting for telemedicine | |
| Time saving | 51.7 |
| Continue with known family doctors | 14.6 |
| Slowing the spread of infections | 32.6 |
| Reimbursement/insurance claims | 1.1 |
| Concerns with adopting for telemedicine | |
| Inadequate assessment | 23.1 |
| Data privacy concerns | 14 |
| Technical training and equipment | 41.5 |
| Physician resistance | 21.4 |
The shift in preference is observed for availing of diagnostic tests at home. An overwhelming majority of those surveyed indicated a preference for home sample collection 75.3% (538/715) over collection in laboratories/ hospitals [Figure 3a]. In addition, about 63.3% (453/715) of respondents indicated a preference for using technology for health monitoring (Glucometer/ABPM/Pulse oximeter) and are willing to share data with their health-care team [Figure 3b].
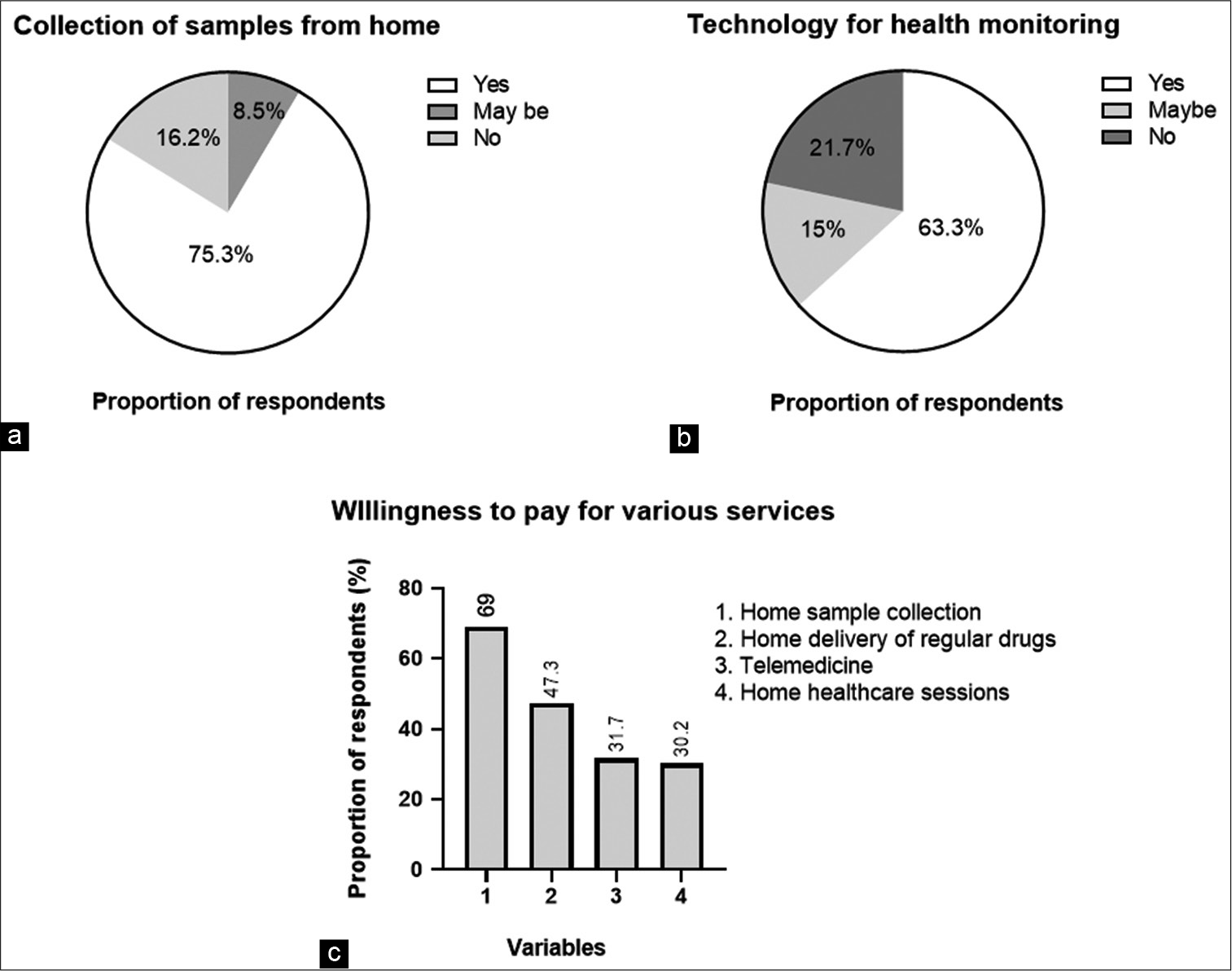
- (a-c) Consumer preferences for diagnostics.
Between 30.2% and 69% of respondents indicated a willingness to pay for services that could be accessed at home with a medical subscription [Figure 3c]. About 69% of consumers are willing to subscribe for at-home blood tests to track overall health. About 47.3% (338/715) of consumers are willing to subscribe for home delivery of regular drugs. About 31.7% of respondents (227/715) are willing to subscribe for telemedicine, while 30.2% of respondents (216/715) are willing to receive home health-care sessions from a doctor or nurse to understand their health needs.
DISCUSSION
Our questionnaire-based study indicates the increasing preference for telemedicine, at-home self-diagnostic and monitoring tests and captures the contemporary notion and expectations of patients during a pandemic outbreak. Our observations align with other recent studies.[10,11]
Globally, the COVID pandemic and the enforced lockdown have caused anxiety across the entire human race. The SMART India questionnaire-based study captured the negative impact of COVID-19 on the health-care delivery.[12] During this time, there has been a dilemma among the patients with comorbid disorders who needs routine monitoring of their health to visit hospitals and clinics. As expected, in our survey, the majority (63.9%) of the respondents had concerns about visiting a hospital during the lockdown [Figure 1a]. A US-based study reported that one-third of adult respondents had delayed or avoided routine medical care during the pandemic because of concerns about COVID-19.[13] Other such recent reports highlight that hospital admissions, overall emergency department (E.D.) visits and the number of E.D. visits for even heart attack, stroke and hyperglycaemic crisis have declined since the pandemic has started.[14-16] This is also reflected by most of the participants (88%) avoiding hospitals that treat COVID-19 patients. The majority (69.7%) of the respondents did not prefer COVID-19 treating hospitals and 18.3% were willing to consider hospitals that kept treatment of COVID-19 infected individuals in well isolated wards. Only 12% of respondents did not have an issue with getting their regular check-ups at a health-care facility that treats people with COVID-19 [Figure 1b and c].
In addition, several respondents insist the need for several safety protocols, including personal protective equipment and thermal screening at the health-care facility [Table 2]. About half of the respondents wish for isolated fever clinics and separate access points for individuals presenting with signs and symptoms of COVID-19 infections. Therefore, the hospitals have to devote considerable resources to implement reassuring measures to conform COVID-19 safety and communicate the same to build trust with the consumers.
Although adherence to community mitigation efforts such as stay-at-home orders, temporary closures of health facilities or additional factors is necessary, it leads to another global health concern. If this avoidance of routine care sustains, it is major setback for the management of chronic conditions, receipt of routine vaccinations or early detection of new conditions.
Hospitals are and will have to equip themselves for developing capabilities for alternate channels of administering care, such as telemedicine or home healthcare.[17,18]
Such declining trend in the hospitalised patients or patients visiting ED is not an indication of reduced incidences of prevailing comorbidities. Health management during lockdown remains a concern for 59.3% of respondents.
There is an increasing trend (approximately 10-fold from 2.8% to 24.9%) in the utilisation of virtual health channels during the lockdown [Figure 2a]. An Israel-based survey by Grossman et al. reported that daily use of videoconferencing increased from 1% before COVID-19 to 12% during the lockdown.[19] Even before the pandemic, consumer adoption of virtual visits has been increasing since 2018, majorly favoured as a time-saving option. Virtual consultations are expected to flourish even in a post-pandemic world, as noted by 51.7% of consumers who use telemedicine. On an average, 31.7% are inclined to continue virtual visits even after COVID-19 era [Figure 3c]. About, one-third tried telemedicine to slow the spread of infection. In line with Deloitte survey (73%),[20] more than half of the respondents with no prior experience with telemedicine expressed interest to use it in the near future, [Table 3]. Inadequate assessment, insufficient technical training and equipment were among the top concerns in adopting telemedicine [Table 3]. One of the biggest obstacles to the use of telehealth has been providers’ reluctance to embrace this technology in caring for patients. A study of telephone triage reported patient safety risks and the lack of clear visual clues that help physicians identify patients with acute conditions.[21] With many introduced to virtual health visits for the first time during the pandemic, consumers are increasingly willing to receive virtual care for various services. Therefore, hospitals must prioritise developing telemedicine platforms and digitally upskilling their staffs. It is important that providers ensure that services are appropriately priced according to the patient’s willingness to pay and delivered in the same manner as in-person visits.
As an alternate strategy, various hospitals launched their own home health-care services or partnered with established home health-care providers to continue patient care beyond the hospital walls during COVID-19.[18] Respondents indicated a clear preference to receive care at home – including consultation, diagnostic testing and delivery of medications. Diagnostics players should consider enhancing capabilities developed during COVID-19 for home collection and/or explore possible partnership opportunities to enhance last-mile connections and expand home collection networks in their geographies. The adoption of apps and at-home self-diagnostic tests is accelerating. Most respondents are willing to share data with their health-care team. Mobile devices, at-home tests and other emerging technologies are being developed as part of holistic wellness and prevention strategies, ranging from the diagnosis of acute infections to the management of chronic diseases and identifying future risks of illness.
In addition, with an increase in the elderly population in tier-2 and tier-3 cities, demand for home health-care services is likely to increase. In keeping up with this emerging trend, providers are now toying with the idea of offering subscription-based customised packages to manage care (including for chronic patients who need regular care management).
Home blood testing, regular medication delivery and telemedicine are among the top three services consumers want to subscribe. However, less than a third of the respondents believe that a doctor or nurse needs to physically examine them to understand their health needs and are willing to subscribe to home health-care sessions [Figure 3c].
With the COVID-19 pandemic on the horizon, we are witnessing the rapid evolution of demands in the utility of healthcare by health-care consumers.[10] Each individual’s health journey and experiences with the pandemic has been unique. Health-care organisations must recommit themselves to understanding changing consumer behaviours and deploying new tools and services to benefit consumers through data interoperability, train clinicians in virtual health technologies and earn consumer trust through empathy and reliability.
CONCLUSION
The COVID-19 experience has changed our perceptions and behaviours and the health-care system needs to shape a ‘new normal’ that works for both patients and providers.
This research will deliver a valuable guidance for industry leaders consumer perceptions and behaviours — now and in the future.
With the innovative players in the space are already recognising these trends and are exploring tech-enabled solutions, health management will become much more integrated in the future, several services will either transform to a virtual setting or consumers’ homes, with technology platforms pulling them together — much like a jigsaw puzzle.
Acknowledgment
The authors acknowledge all the study participants for their cooperation in this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Nosocomial COVID-19 infection: Examining the risk of mortality. The COPE-nosocomial study (COVID in older people) J Hosp Infect. 2020;106:376-84.
- [CrossRef] [PubMed] [Google Scholar]
- SARS-CoV-2 transmission in patients with cancer at a tertiary care hospital in Wuhan, China. JAMA Oncol. 2020;6:1108.
- [CrossRef] [PubMed] [Google Scholar]
- Indirect virus transmission in cluster of COVID-19 cases, Wenzhou, China, 2020. Emerg Infect Dis. 2020;26:1343-5.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors for COVID-19-related mortality in people with Type 1 and Type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020;8:823-33.
- [CrossRef] [Google Scholar]
- Glycemic characteristics and clinical outcomes of COVID-19 patients hospitalized in the United States. J Diabetes Sci Technol. 2020;14:813-21.
- [CrossRef] [PubMed] [Google Scholar]
- association of blood glucose control and outcomes in patients with COVID-19 and pre-existing Type 2 diabetes. Cell Metab. 2020;31:1068-77.e3.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19 transforms health care through telemedicine: Evidence from the field. J Am Med Inform Assoc. 2020;27:1132-5.
- [CrossRef] [PubMed] [Google Scholar]
- Trends in emergency department visits and hospital admissions in health care systems in 5 states in the first months of the COVID-19 pandemic in the US. JAMA Intern Med. 2020;180:1328-33.
- [CrossRef] [PubMed] [Google Scholar]
- Appendix 5 of the Indian Medical Council (Professional Conduct Etiquette and Ethics Regulation) 2002. Available from: https://www.mohfw.gov.in/pdf/telemedicine.pdf [Last accessed on 2021 Sep 22]
- [Google Scholar]
- COVID-19's impact on home health services, caregivers and patients: Lessons from the French experience. Lancet Reg Health Eur. 2021;8:100197.
- [CrossRef] [PubMed] [Google Scholar]
- Telemedicine, the current COVID-19 pandemic and the future: A narrative review and perspectives moving forward in the USA. Fam Med Community Health. 2020;8:e000530.
- [CrossRef] [PubMed] [Google Scholar]
- Impact on health and provision of healthcare services during the COVID-19 lockdown in India: A multicentre cross-sectional study. BMJ Open. 2021;11:e043590.
- [CrossRef] [PubMed] [Google Scholar]
- Delay or avoidance of medical care because of COVID-19-related concerns United States, June 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1250-7.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in hospital admissions for urgent conditions during COVID-19 pandemic. Am J Manag Care. 2020;26:327-8.
- [CrossRef] [PubMed] [Google Scholar]
- Potential indirect effects of the COVID-19 pandemic on use of emergency departments for acute life-threatening conditions United States, January-May 2020. MMWR Morb Mortal Wkly Rep. 2020;69:795-800.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of the COVID-19 pandemic on emergency department visits United States, January 1, 2019-May 30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:699-704.
- [CrossRef] [PubMed] [Google Scholar]
- Opportunities and challenges for contactless healthcare services in the post-COVID-19 Era. Technol Forecast Soc Change. 2021;167:120712.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of hospital-at-home models: A systematic review of reviews. BMJ Open. 2021;11:e043285.
- [CrossRef] [PubMed] [Google Scholar]
- The future of telemedicine visits after COVID-19: Perceptions of primary care pediatricians. Isr J Health Policy Res. 2020;9:53.
- [CrossRef] [PubMed] [Google Scholar]
- Changing Consumer Preferences towards Health Care Services: The Impact of COVID-19. 2020. Available from: https://www2.deloitte.com/content/dam/deloitte/in/documents/life-sciences-health-care/in-lshc-deloitte_healthcareconsumersurvey-new-noexp.pdf [Last accessed on 2021 Sep 22]
- [Google Scholar]
- Effect of visual cues, vital signs, and protocols on triage: A prospective randomized crossover trial. Ann Emerg Med. 1998;32:655-64.
- [CrossRef] [Google Scholar]




