
Translate this page into:
Developing and introducing structured cooperative self-directed learning activities for undergraduate medical students

*Corresponding author: Puja Dulloo, Department of Physiology, PIMSR, Parul University, Vadodara, Gujarat, India. drpujapsmc@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dulloo P, Patel M, Vedi N. Developing and introducing structured cooperative self-directed learning activities for undergraduate medical students. Indian J Physiol Pharmacol. 2024;68:252-62. doi: 10.25259/IJPP_128_2023
Abstract
Objectives:
The National Medical Commission of India introduced Competency-based Medical Education in 2019 mandated duration allocation for the self-directed learning (SDL) activity in each course throughout the undergraduate medical programme. A successful implementation requires a structured methodology for the introduction of SDL activities for the undergraduate learner. The objectives of this study were as follows: (1) To develop and implement structured cooperative self-directed learning (Sc-SDL) activity for 1st-year medical students. (2) To explore perceptions of students for the developed process (Sc-SDL).
Materials and Methods:
A prospective cohort study for 1st-year medical students was initiated, exposing them to three Sc-SDL activities having sessions in a blended manner. The formative assessment score was analysed by mean, standard deviation and paired t-tests. A validated learner feedback questionnaire was submitted by the participants, which was analysed by the Friedman rank test and satisfaction index. Analysis for open-ended questions from the participants 3 months after completion of the course was by thematic analysis manually.
Results:
The academic score for topics taught through the Sc-SDL approach ranged from 67.62 ± 21.72 to 83.72 ± 24.34 (Activity-1–3), showing significant differences in scores for Activity-1 with 2, and Activity-1 with 3. The maximum satisfaction index score and Friedman rank, from the learner feedback questionnaire were for item 8 (8.80; 93.6%) and the minimum for item 10 (3.28; 57.83%). Three major themes other than suggestions for improvement were identified from the open-ended questionnaire.
Conclusion:
The Sc-SDL approach showed an increase in academic gain, thus enhancing the cognitive approach of the learner. The activity encouraged undergraduate students to attain attributional and social skills such as team-building, sharing, presentation skills and time and conflict management. However, input from other stakeholders needs to be considered.
Keywords
Learning
Self-directed learning
Cooperative learning
Collaborative learning
Undergraduate medical students

INTRODUCTION
The concept of self-directed learning (SDL) starts from the time a child is born, We need not teach a child how to breastfeed, although they are initially guided and later are self-directed to accomplish the task. There are many examples that we can quote from our ancient history one being the story of Ekalavya from Mahabharat.[1] Researchers mention that 74% of Indian students are joining private tuition/coaching centres drifting them toward the practical aspect of the taught course and having little way to expand the co-curriculum strength.[2] Probably, our school education system with the parallel education system is curbing the SDL efficiency of students. Hence, there is a need to recreate activities to enhance students’ skills of being SDL and, subsequently, lifelong learners.
The amended Regulations on Graduate Medical Education-2019[3] provided a layout for the new model of curriculum, Competency-Based Medical Education (CBME), for undergraduate Indian medical students starting from Batch 2019 to 2020. The curriculum, in its three volumes, enlists the competencies to be attained by undergraduate students to be competent as Indian medical graduates.[4] Concepts such as Foundation Courses, Early Clinical Exposure, Electives, Professional Development including Attitude, Ethics and Communication Module, Learner-doctor method of clinical training (Clinical Clerkship) and SDL were officially introduced in the formal CBME curriculum.[3] For the first time, the term lifelong learner was specified in the formal medical curriculum.[4] Specific time-slot durations are allocated for each module. Mandate specific hour allocation for the SDL activity for each subject in each academic year became the catchword for every faculty of medical institutes across the country.[3]
In 1975, Knowles[5] defined SDL as ‘A process in which individuals take the initiative, with or without the help of others, in diagnosing their learning needs, formulating learning goals, identifying human and material resources for learning, choosing and implementing appropriate learning strategies and evaluating learning outcomes (LOs)’. Over time, different researchers have presented various models for SDL starting from Knowles[5] in 1975, Long’s[6] in 1989; Candy[7] and Brockett and Hiemstra[8] in 1991; Garrison’s[9] in 1997; Oswalt[10] in 2003 and Boyer et al.,[11] in 2014, have explained the approach of SDL in their manner. All the models of SDL, in sequence, added strategies where students would have accountability for their learning.
SDL is viewed as a complex process that ingrains the quality of critical thinking, problem-solving, analytical and resource search skills over and above that of developing the affective attributes of team-building, communication and interpersonal skills.[12-15] Attaining the skill of SDL will monitor students’ conceptual understanding of the content and ability to integrate disciple-based information to synthesise their knowledge and apply it in the real practical world, thus being a lifelong learner.
Towle and Cottrell,[16] in their study, have enlisted SDL activities starting from setting learning goals by learners to monitoring the effectiveness of self-study habits which not only facilitates learning but also helps learners cultivate the critical skills of lifelong learning.[16]
Numerous studies have shown a variety of teaching-learning strategies such as case-based learning, problem-based learning (PBL) and team-based learning that allow students to be self-directed learners.[17-20] The study on case-based learning showed a beneficial outcome for motivating students to be self-directed learners and develop analytical and problem-solving skills.[17] Similarly, the team-based learning approach showed better interaction among learners leading to active engagement and an increase in academic performance.[18] PBL strategy allows students to work in groups on a problem in 2–3 learning sessions which are well spaced out allowing students to undertake SDL and manage information to be able to discuss in the final session.[18,20] The challenges of having limited trained facilitators to conduct the sessions, work overload and the time to prepare relevant contextual cases as per students’ milestones and specific time-slot to be incorporated as per regulatory norms[21] being faced at our level limit its implementation.
Researchers have published plans[22] or faculty guide reviews[23] showing ways or approaches for implementing SDL modules/activities.
The shortage of faculties in institutes like Indian medical institutes[24] may not allow the absolute focus of the facilitators on each learner. There is a need for the development of a model that would provide an opportunity for students to attain SDL skills despite human resources limitations. Thus, the study was devised by amalgamating the SDL approaches with the five principles of Cooperative Learning (CL) of Johnson and Johnson[25] and termed it Structured Cooperative SDL (Sc-SDL). This model was incorporated for the 1st-year medical students as per the requirement of a competency-driven undergraduate curriculum prepared by the National Medical Commission, India, earlier named the Medical Council of India, where specific hours have been indicated for SDL sessions in each subject.[3]
The study aimed to develop and introduce a Sc-SDL activity as a student-centric approach for 1st-year undergraduate medical students and to identify their perceptions.
MATERIALS AND METHODS
Ethical approval
The study was conducted for 150 1st year undergraduate medical students after acquiring ethical approval.
Study design
A prospective, observational and cohort study for 150 1st-year medical students was done from (June to November 2021) with a sequential mixed-method approach. The study commenced by developing and implementing a Sc-SDL activity in the department of physiology.
Before the initiation of the activity, all seven facilitators, of the department were oriented on the concept, planning and conduct of the strategy. The role of the facilitator, in terms of observing learners throughout the process for each session, scoring them, and providing them with feedback at the end of each session, was explained to the facilitators. Input and suggestions for modifying the strategies were welcomed.
In the next step, students were sensitised regarding each step of the Sc-SDL activity, and their expected roles and responsibilities during the process were highlighted. The key components of Group Dynamics and Group Behaviour Among Adults,[26,27] such as creating a group, collaborative knowledge building, teamwork, conflict management and practical value were explained. Thus, students were aware that, with each Sc-SDL small group, members had to choose a leader, recorder, reporter and timekeeper and other members’ roles had to be clarified within the group.
For the first Sc-SDL module, the students were selected as per roll number, and subsequently, for each Sc-SDL activity, systemic random sampling was done, dividing students into five/six groups each time under a different facilitator from the department. The systemic random selection was done based on student feedback since they expressed a desire to engage in team building and learning with their classmates.
The entire activity was conducted under three sub-sessions with a specific time duration for each session. They were specified as in Figure 1:
Exploring session (60–120 min),
Interactive intersession (7–10 days)
Sharing session (120 min).
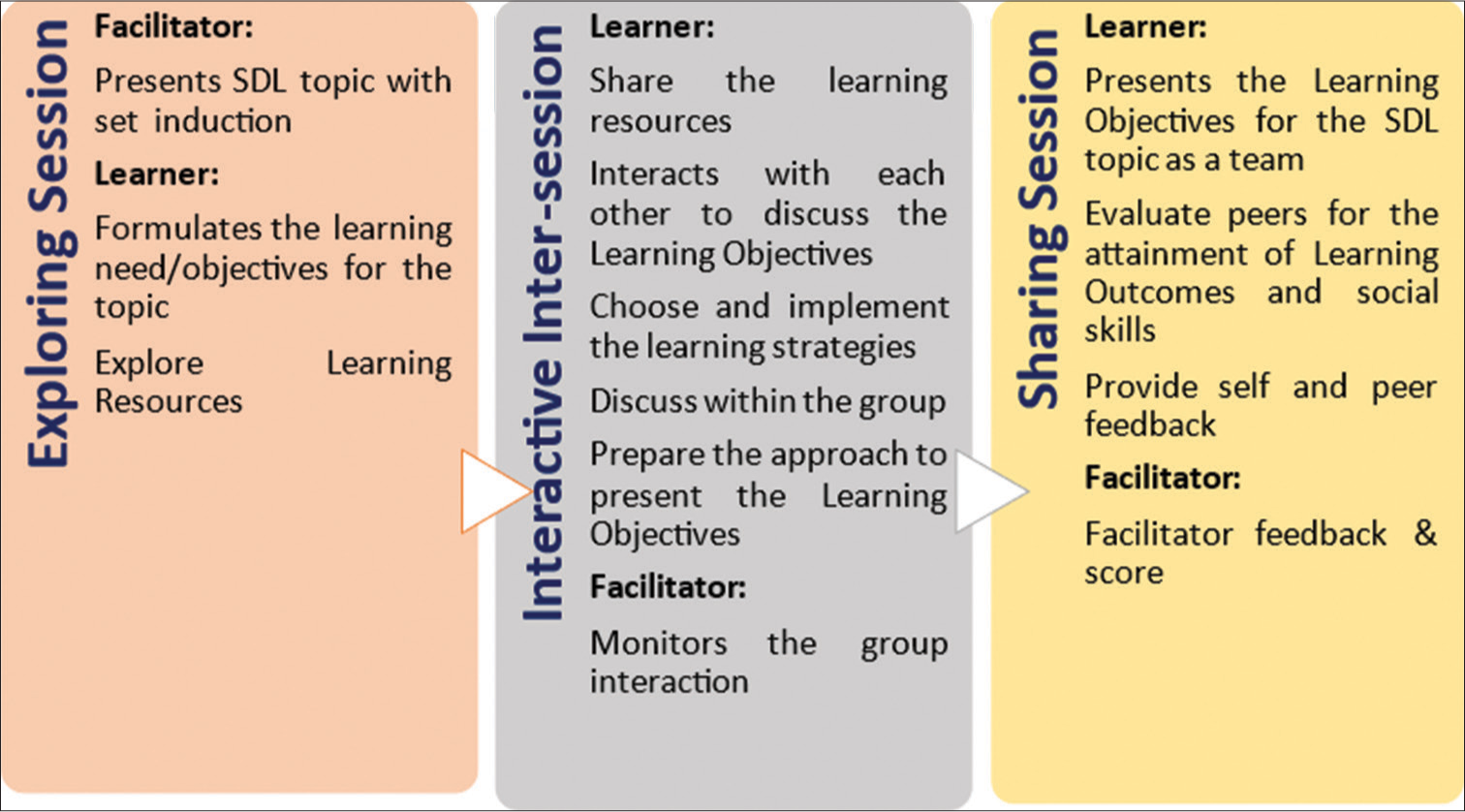
- Strategy for the structured cooperative self-directed learning (SDL) activity
Before session 1, a departmental meeting was organised. The topic was identified for the Sc-SDL strategy for 1st-year medical students by the department of physiology.
A set induction in the form of a clinical case scenario was incorporated to introduce the topic in the form of a trigger. The specific expected LOs were identified by the departmental members for the topic; this allowed all the facilitators to be on the same page during the small group activity.
Exploring session
During this session, students were exposed to the Sc-SDL module using a clinical case scenario as a trigger by the coordinator. Then, the students were subdivided into further small groups as per the number of available facilitators (maximum of 30 students/facilitator), formal task-based groups. Each group initiated their discussion on the topic following the rules of group dynamics. The group identified the LO and primary resources that they would be exploring to understand the topic better. The finalised LOs, task distribution as per the group members and list of primary resources were submitted to the facilitator and shared with the group members.
Role of facilitator during exploring session
Initially, facilitators guided learners in following the group dynamics, for CL. The hand-holding of the facilitator for the entry-level medical students was by identifying the topic as a need for learning for the Sc-SDL module. They ensured that the LOs identified by the group would cover those identified by the department. The facilitator confirmed that the discussion was focused on identifying the LOs, primarily, and confirmed that the group was using appropriate and relevant resources for the topic. They clarified to the group that the group could be guided by them in case they felt stuck at any given point of discussion.
Interactive inter-session
The digitally connected group was created by the group leader/member through WhatsApp group, Google Meet and Zoom breakout rooms, in which the facilitator was included, enabling the facilitator to monitor group activities and coordination. However, other modes of technology such as e-classrooms, Google groups, Telegram groups and other platforms were kept open for inter-session activity. The discussion related to the topic was through those connecting digital groups. The group was free to explore appropriate resources from the library in the form of textbooks, articles/reviews of literature/e-journals/Blogs from different search engines, Web-based learning (Clinical discussion forums, Short online courses) or Online reference material (Ted talks, YouTube,…). They were free to explore cases of a similar type in the hospital after seeking permission from the respective departmental head/in-charge. All the students were instructed to write their roll number after adding a resource material, asking a question or responding to the question. This allowed facilitators to keep track of discussions as well as students within the group.
They were instructed to prepare an online PowerPoint link to make every member contribute toward the making of the final presentation and relevant components could be inserted as per the LOs identified during session 1.
Role of facilitator during the session
They guided the learners wherever and whenever they felt wedged. Facilitators maintained records of each session activity and discussion by the group since they were part of the digital connecting group. They monitored the electronic usage of the database and access to reliable resources like the number of hits at resources and library visit entries.
Sharing session
During this session, students within the group present the topic as per the identified LOs in a sequential manner followed by question and answer and discussion among themselves. Each member was allowed to present a part of the presentation. This allows everyone to gain presentation skills and public speaking skills, which further enhanced their ability to express ideas and explain in front of colleagues. The group had the flexibility to choose the way of presentation in the form of a Seminar (PPT, Video and Audio), Collage, Poster presentation, role play, panel discussion, etc. During these Sc-SDL activities, students presented their outcomes as animated PowerPoint seminar presentations. However, during the Sc-SDL session on the topic Myasthenia Gravis (Activity 1), one of the student group presented a patient’s interview along with the PowerPoint presentation.
Role of facilitator during the session
The facilitators listened to the presentation prepared by the students in the group and provided an opportunity for every group member to present a part of the topic. They also ask questions to the presenter and motivate other members. Facilitators provided feedback to the group as a whole and identified the students who did well throughout the three sessions of the Sc-SDL activity, as well as those who needed further guidance. Finally, they will allow students to attempt the online assessment in the form of multiple-choice questions (MCQ) to assess their cognitive gain. The facilitator will also create an opportunity by asking students to provide input for their performance as well as that of their peers through self-assessment visual analogue scale and peer-score sheets. Finally, the group would be asked to reflect on their experiences with the Sc-SDL activity by the facilitators.
Sessions conducted
A total of five student-centric activities were conducted as per the Sc-SDL module for the topics [Table 1]. The competency-based undergraduate medical curriculum’s core and must-know levels comprised the topics from the physiology course that were chosen for the Sc-SDL sessions. Keeping practicality in mind, at least five facilitators participated in the activity at once.
| S. No. | Topic for Sc-SDL | Sc-SDL sessions (duration and mode; online/offline) | ||
|---|---|---|---|---|
| Exploring session | Interactive intersession | Sharing session | ||
| 1. | High altitude sickness | 60 min; Offline | 7 days; Google meet and WhatsApp | 120 min; Offline |
| 2. | Dumping syndrome | 60 min; Offline | 7 days; Google meet and WhatsApp | 120 min; Offline |
| 3. | Myasthenia Gravis | 120 min; Offline | 10 days; Google meet and WhatsApp | 120 min; Zoom breakout room |
| 4. | Nephrotic syndrome | 120 min; Zoom breakout room | 10 days; Google meet and WhatsApp | 120 min; Zoom breakout room |
| 5. | Refractory errors | 120 min; Offline | 7 days; Google meet and WhatsApp | 120 min; Offline |
Sc-SDL: Structured cooperative self-directed learning activity
The first two activities were taken as a pilot test session for the Sc-SDL activity. During those pilot Sc-SDL activities, facilitators identified the issues related to the implementation of the activity at different stages. During the exploring session, facilitators could not have a separate room for the small group discussion. Secondly, students were not able to frame LOs for the topic (despite sensitisation session for the same), during intersession, they just forwarded the presentation for their assigned topic and there was no discussion within the group, and during the sharing session, students had presented their part of the LO without having an understanding about what others had to present as a sequence. The facilitators and authors discussed the issue and came up with the following solutions to overcome those challenges for subsequent activities.
The main challenge of identifying a separate demo room for each group was overcome by collaborating with other departments and using their demo rooms for the activity. However, during the COVID state, the conversion of the offline session shifted to the online mode using the Zoom breakout room for the first session, and the third session for presenting the LOs of the topic worked well. Even inter-session discussion groups interacted through WhatsApp and Google Meet.
Initially, facilitators held hands in groups, thus guiding the group on how to frame LO. Later, they managed to do it on their own.
A facilitator score sheet was prepared and validated where the facilitator would grade their group for each session. Hence, the facilitator instructed students to discuss the topic and its LO in their respective online groups rather than submitting their presentation slides during intersession. The group was asked to add a summary of the article/resource link, which they forwarded to the inter-session connecting group. This forced and motivated students to read the text, analyse it’s important points and, finally, present it to the group in the form of a summary with a link. Thus increasing their skills related to search strategies, reading and critical analysis skills.
Every student had to be prepared with the delivery of the presentation since it was made clear that the facilitator would randomly select the presenter for the sharing of each LO rather than the students themselves choosing the slides from the presentation. This made every student accountable and prepared for every component of the presentation.
After completion of all the Sc-SDL activities, students were asked to submit their perceptions through a learner feedback questionnaire. The learner feedback questionnaire was developed by the author team in consultation with professional colleagues within and outside the institute. Short and simple sentences were used to keep the meaning unambiguous. The learner feedback had 13 items, divided into self and peer feedback, that needed to be scored by the learners on a scale of 1–5, where 1 was ‘strongly disagree’ to 5 was ‘strongly agree’. The key areas for learner feedback were to find the perceptions of students on various aspects of conduct and dynamics while working in groups for SDL activities and to gain collaborative and lifelong learning skills. The learner feedback also had three open-ended questions to assess students’ learning from working in groups, contribution to group learning and suggestions to improve team performance and presentation.
Face validity for learner feedback was done with six experts from the medical education institute. A pilot test was done on 2nd-year undergraduate students of the 2019–2020 batch (n = 20), for the readability and understandability of the questions, who were selected voluntarily, and Cronbach’s alpha of 0.87 was calculated.
Purposive sampling was done where students from the same batch were asked to fill out an open-ended questionnaire 3 months after moving to the 2nd-year of the medical program. The sampling was for having at least two students as per gender, high (>65%) or average score (50–65%) attained for 1st-year summative examination. Four experts from the medical institute did the face validity for the open questions. The idea was to gather input from the stakeholders for the conduct of the Sc-SDL activity as per the attainment of the outcome in terms of achieving the characteristics of SDL such as setting clear goals, shaping their learning process in line with goals and plans, monitoring their learning process, self-motivation, value learning, ability to identify apt resources and evaluating the outcomes of their learning.[28]
The data for academic gain were obtained from the pre-university examination to compare the outcomes of students for the topics taught by Sc-SDL and assess the progress in the level of academic score from one to the next Sc-SDL activity.
Statistical analysis
The academic scores outcome was analysed by calculating the mean, standard deviation and paired t-tests using the Statistical Package for the Social Sciences-15 software. The Percentages, mean, standard deviation, Friedman rank test and Satisfaction Index[29] were calculated for the quantitative data obtained for the learner feedback questionnaire, while an inductive semantic approach of thematic analysis was done for open-ended questions and qualitative data.[30,31] The transcript preparation and analysis were done manually by two coauthors, independently, and then, data were compared and compiled for final output.
RESULTS
Descriptive statistics are demonstrated in Table 2 (mean ± standard deviationSD) for the academic scores for the topic taught via the Sc-SDL approach, ranging from 67.62 ± 21.72 (Activity-1: Myasthenia gravis), 78.91 ± 23.53 (Activity-2: Refractory errors), and 83.72 ± 24.34 (Activity-3: Nephrotic Syndrome). Thus, better academic outcomes is achieved by the students once they attain better understanding and adaptability towards Sc-SDL approach of learning.
| S. No. | Sc-SDL topic | Number of learners (n) | Mean±SD of test scores |
|---|---|---|---|
| 1. | Myasthenia gravis | 151 | 67.62±21.72 |
| 2. | Refractory errors | 119 | 78.91±23.53 |
| 3. | Nephrotic syndrome | 137 | 83.72±24.34 |
SD: Standard deviation, Sc-SDL: Structured cooperative self-directed learning activity, C-SDL: Cooperative self-directed learning activity
As shown in Table 3, the statistical significance (P < 0.005) of the academic scores achieved for the topics Activity-1 and 2 and Activity-1 and 3 by the Sc-SDL teaching-learning method. The topics of Nephrotic Syndrome (Activity-3) and Refractory errors (Activity-2) were the last two activities taught by the Sc-SDL approach and thus probably did not show a significant difference as per the paired student t-test.
| Independent student test | Mean±SD | df | Sig. (2-tailed) |
|---|---|---|---|
| SDL-Nephrotic syndrome - SDL-Refractory errors | 3.45±28.66 | 118 | 0.192 |
| SDL-Nephrotic syndrome - SDL-Myasthenia gravis | 17.01±34.71 | 136 | 0.000 |
| SDL-Refractory errors - SDL-Myasthenia gravis | 11.93±31.95 | 118 | 0.000 |
Statistical significance is observed for topics taught by Cooperative SDL and with other traditional techniques. Sc-SDL: Structured cooperative self-directed learning activity, SD: Standard deviation, df: Degree of freedom, Sig: Significance
Descriptive statistics are demonstrated in Table 4 for the learner feedback for the Sc-SDL approach showing ‘agree’ and ‘strongly agree’ for most items of the feedback questionnaire except for the item ‘I would have learned better independently,’ that showed lesser percentage of agreement. The Cronbach’s alpha for the 13 items of the questionnaire was 0.85. The table shows the Friedman Mean Rank Test and satisfaction index of each item. The result showed the highest value (the Friedman Mean Rank Test and satisfaction index) for item 8 ‘Working together we could fulfil the knowledge gap’ (8.80; 93.60) and the lowest value for item 10 ‘I would have learned better independently’ (3.28; 57.83). Twelve out of 13 items have shown satisfaction indexes of >75.[29,32]
| S. No. | Items for learner feedback | Mean±SD | Friedman test Mean rank | Satisfaction index |
|---|---|---|---|---|
| 1. | The leader was chosen unanimously by the group | 4.05±1.28 | 7.39 | 82.08 |
| 2. | Every person had the opportunity to express their views for framing learning Objectives |
4.49±0.85 | 8.63 | 91.43 |
| 3. | Appropriate time was spent on the SDL activity discussion by the group members |
4.32±0.88 | 7.83 | 87.79 |
| 4. | The workload for the SDL activity was evenly distributed | 4.17±0.97 | 7.36 | 87.14 |
| 5. | Most of the colleagues made a significant/notable contribution | 3.70±1.07 | 5.44 | 77.54 |
| 6. | Most of the colleagues made a timely contribution | 3.90±0.86 | 5.92 | 81.47 |
| 7. | Leaders and other members were able to manage the conflict within the group | 4.49±0.65 | 8.47 | 91.43 |
| 8. | Working together we could fulfil the knowledge gap | 4.56±0.69 | 8.80 | 93.60 |
| 9. | Input from other members contributed to my learning | 4.10±1.06 | 7.27 | 84.38 |
| 10. | I would have learned better independently | 2.94±0.99 | 3.28 | 57.83 |
| 11. | The team helped me to learn different ways to do literature or resource searches via the internet |
4.01±0.80 | 6.30 | 84.12 |
| 12. | The team motivated me to think about the topic | 3.95±0.92 | 6.11 | 82.32 |
| 13. | SDL activity helped me to acquire lifelong learning skill | 4.43±0.67 | 8.21 | 90.53 |
The Chi-square test for Learner feedback Friedman Test score was 220.448 with df 12; Monte Carlo Significance at 95% Confidence Interval was 0.0001. SDL: Self-directed learning activity, SD: Standard deviation
As shown in Figure 2, the themes and sub-themes as per the responses acquired from the open-ended questions from the learner feedback questionnaire for the Sc-SDL student-centric approach.
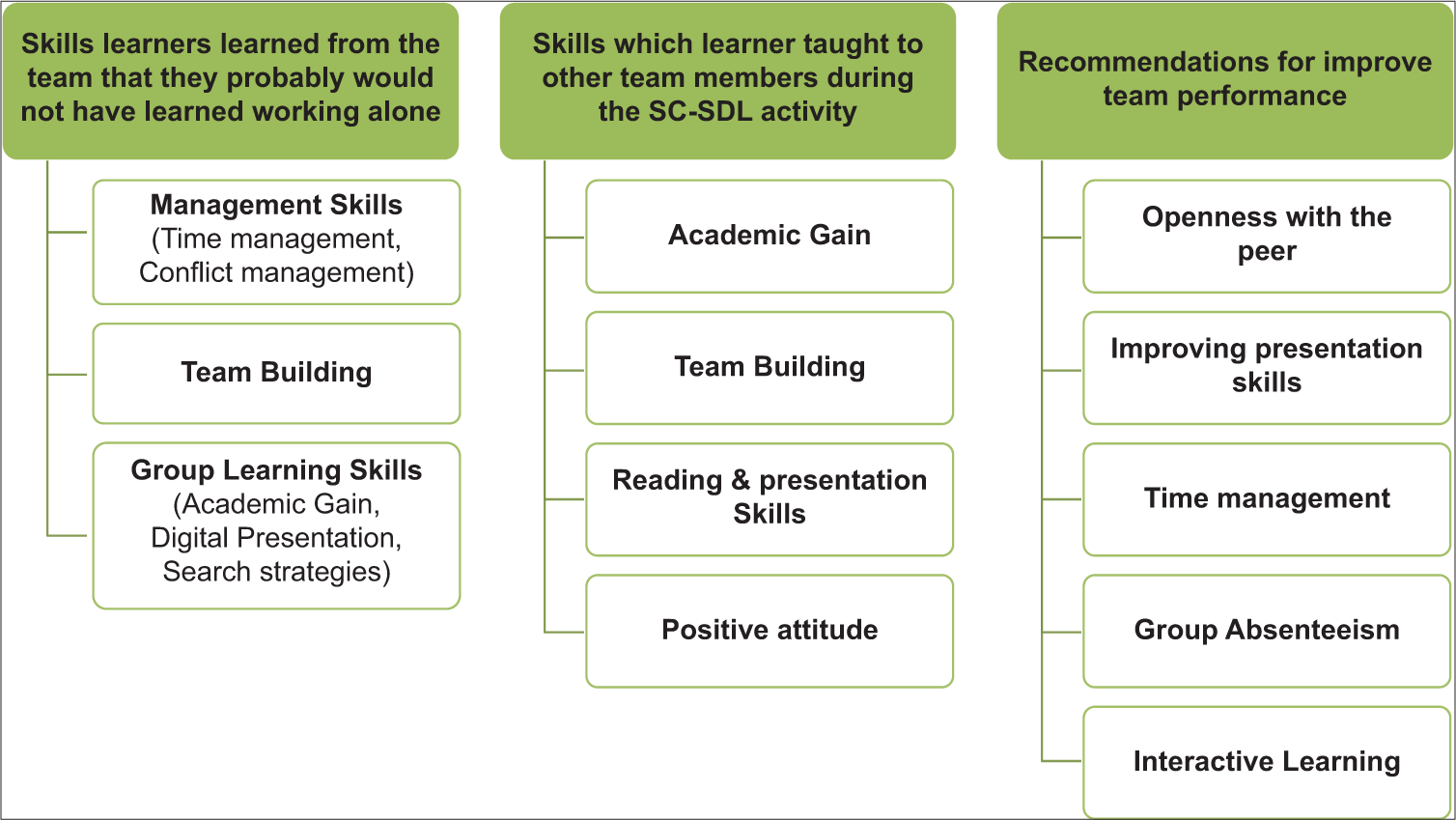
- Response to open-ended questions in the learner feedback questionnaire. SC-SDL: Structured cooperative self-directed learning activity.
As shown in Table 5, the input from the students for the Sc-SDL activity after the completion of the course through thematic analysis showing three major themes need identification, searching skills and outcome attainment. However, students provided suggestions for improving their learning by the Sc-SDL approach. They provided input for each session of the approach.
| Theme | Sub-theme | Description |
|---|---|---|
| Need identification | Identifying topic/s | “...understand the importance of a particular topic in clinical as well as from exam point of view.” (A2F) |
| “…SDL taught me was that the topics selected for SDL were extremely useful in our daily lives.” (A1M) | ||
| “..usually identify topic based on my interest and its importance.” (H1M) | ||
| “…able to point out a specific topic which is important and high yield.” (H1F) | ||
| “..foundation built in 1styear. proven helpful in subjects like pathology and microbiology” (H2F) | ||
| Framing objectives | “I am able to identify the topic learning objectives” (A1F) | |
| “..previous SDL experience. we are competent enough to choose learning objectives” (A2F) | ||
| “...now we can make objectives easily of any topic” (A1M) | ||
| “..after having many SDL sessions, I can enlist learning objectives by myself after exploring them” (H1F) |
||
| “..enlisting objectives before reading any topic…….it proved helpful by SDLs.” (H2F) | ||
| Searching skills | “...I cannot identify the resources… mentor/facilitator to guide which resources are to be referred.” (A1F) | |
| “…well oriented with reliable sources and authentic resources.” (A2F) | ||
| “…I am referring to higher books such as Harrison- which I might not have done.” (H1M) | ||
| “…approach to include research articles in the presentation in case there is less content in books.”(H2M) | ||
| “..to explore the more about the ongoing cases.”(H3M) | ||
| Outcome attainment | “…I can present the topic to the peers.” (A1F) | |
| “...extensive research makes me more confident to teach to friends.” (A1M) | ||
| “...improved my presentation preparation skill and oral presentation… gaining confidence” (H1M) | ||
| “...SDL sessions made me confident enough to present, speak up in front of a crowd which I was hesitant previously.” (H1F) | ||
| “...communicating with a randomised group of participants helped me to communicate better with others.” (H1F) | ||
| “...helped me in revision of the topics for exam.” (H2F) | ||
| Suggestions | “”...facilitator should monitor and interrogate students so that there is equal efforts and participation of all student.” (A1F) | |
| “...instead of presentation from the group, open question answering should be a better alternative.” (A2F) | ||
| “...group size should be 5–6.” (A2F) | ||
| “...intergroup discussion should be there rather than presentation.” (A2F) | ||
| “...ppt presentation is time-consuming” (A1M) | ||
| “...explain the topic in front of the class without the aide of ppt…” (A1M) | ||
| “...topic for SDL should be based on students’ opinion.” (H1M) | ||
| “...balance between core and semi-core areas in the SDL topic.” (H1M) | ||
| “”...MCQ should be avoided.exam should not be on the same day.” (H1M) | ||
| “Peer scoring should not be kept for assessment.” (H1M) | ||
| “...identify the dormant students of SDL group and counsel them by their facilitator.” (H2M) | ||
| “...group should be made randomly so that students come across different mindsets.” (H2M) | ||
| “...everyone is not on the same plane of understanding.” (H3M) | ||
| “…peer scoring as assessment is not good.students are scoring themselves by telling the other students, I will do the same to you” (H3M)”.practice presentation should be done in presence of facilitator.” (H1F) | ||
| “...MCQ assessment done online can be in paperback form as one/two line questions answer…” (H1F) | ||
| “...after presentation, we can do a meeting with our facilitator where facilitator guides us about our overall performance…improve upon it in next SDL.”(H2F) | ||
| “...peer feedback is a good part that is initiated.” (H2F) | ||
AM: Male participant with a score of 50–65% on the final exam; AF: Female participant with a score of 50–65% on the final exam; HM: Male participant with a score above 65% on the final exam; HF: Female participant with a score above 65% on the final exam. SDL: Self-directed learning activity, Sc-SDL: Structured cooperative self-directed learning activity, MCQ: Multiple-choice questions
DISCUSSION
The study demonstrated improvement in cognitive and affective attributional gains by participating through ScSDL. The maximum score achieved for the topic learned through the Sc-SDL activity was 100. Even, a statistically significant difference was observed when comparing the academic score of each Sc-SDL activity of students. However, statistical significance was observed between some of the topics learned by the Sc-SDL except refractive error and nephrotic syndrome. Being the initial stage of learning by the structured approach of SDL probably might be the reason for having a significant difference in the academic scores for the topic of myasthenia gravies and other topics learned by Sc-SDL. The study by Peine et al.,[33] showed similar results. However, Smythe and Hughes’s[34] study showed a similar outcome of SDL assessment compared to conventional teaching, initially, but later, the scores decreased. The probable reason highlighted was the difference in content and time investment, other than proper support and communication with the students for the SDL approach. Similarly, Kooloo et al.’s[35] study for the gross anatomy laboratory sessions showed better outcomes with strictly guided station instructions rather than loosely guided SDL when observed for 8 months duration. The study by LeFlore et al.,[36] favoured instructor-modelled learning compared to SDL during the clinically stimulated experience.
The present approach of Sc-SDL provided a better cognitive outcome as students took charge of their learning and adapted to SDL. Thus, it fits well into quadrant I (low pedagogical control and high psychological control) of Long’s[6] model, which infers that the student is demonstrating self-directedness and facilitators are taking less control of the learning situation.
Brockett and Hiemstra,[8] mentioned in their book that there is a high chance of student success when they have a high level of self-directed readiness score and are being hand-held by the facilitator. This may be because the learner’s experiences are in line with the expectations of the learning situation.[8] The present method of conducting the SDL activity incorporates all the components of the Garrison[9] model of SDL, that is motivation, self-management (Control), SDL and self-monitoring (responsibility). In the present study, a clinical case scenario was used for set induction. However, video recording of stakeholders, newspaper write-ups, movie clips, flipped classrooms, reciprocal teaching, technology-enhanced methods, PBL, group projects[12] and many more can be used depending on the flexibility of the department.
Out of six competencies for SDL mentioned by Patterson et al.,[37] four were identified in the present Sc-SDL activity and the level of each competency was considered as per the academic milestone of the medical student. The four competencies addressed in our present Sc-SDL activity were (i) teamwork: working in a group and preparing a presentation for the sharing session of the Sc-SDL activity; (ii) reflection: where the students narrated their experiences throughout the activity and writing, (iii) critical thinking: where the student’s responded to the MCQ test prepared by the coordinator of the activity for the topic as per the expected LO and (iv) self and peer evaluation: where student graded themselves and peer through a structured assessment score sheet.
In the present study, the Learner Feedback Questionnaire had items for peer and self-feedback, which showed the highest score (4.56 ± 0.81; 8.80) as per the Friedman Rank test for item 8 ‘working together we could fulfil the knowledge gap’ while the lowest score (2.94 ± 0.99; 3.28) for item 10 ‘I would have learned better independently’ which implies that the group as a team together improved their learning for the topic. The result of the items related to SDL showed that this activity helped students to acquire lifelong learning skills (4.43 ± 0.67; 8.21), and the activity allowed every student to frame learning objectives (4.49 ± 0.85; 8.63), thus allowing them to identify topics that they should explore for further studies. The activity also provides an opportunity for students to manage conflicts (4.49 ± 0.65; 8.47).
Hill et al.,[38] study demonstrated the successful implementation of a case-based SDL for 1st-year medical courses, showing a valuable learning experience for the students. Bhandari et al.,[39] showed students and faculty satisfaction with the SDL approach showing learners to be independent and aware of their learning goals and evaluating LOs. The study by Patra et al.,[40] also showed positiveness toward SDL by the students, specifying that the approach led to easy access to resources for learning. Although the study suggested sensitising students about the SDL process and its importance rather than using it as a teaching-learning approach for knowledge acquisition.[40]
The present study, with input from students after passing 1st-year of the medical program, shows improvement in identifying their learning needs, framing the objectives for the topic, searching skills and communication and presentation skills. Thus, other than an increase in the cognitive domain, there is subsequent improvement in their affective attributes, too. The study by Findlater et al.,[13] also supported the SDL approach to improving student engagement, leading to deeper learning and better understanding and knowledge of anatomy. A systematic review for SDL showed a moderate enhancement in knowledge gain while the effective gain for skills and attitude domains.[41]
The present study kept in mind the amount of content in the topic learners would need to cover as per their milestone and the length of time to gain knowledge for the topic through the Sc-SDL approach of teaching-learning which was one of the limitations of Smythe and Hughes.[34] The group performed all the tasks until they attained a metacognitive approach to the topic and significant academic gains other than enhancement of social skills for team building, management skills, digital usage skills and resource search skills.
Student’s suggestions
In the present study, the participants emphasised improvement points in this newer approach of Sc-SDL. Starting from the allocation of fewer students in each group would provide an opportunity for each student to work equally within the team and motivate them for better group interactivity. Few students suggested to have a mock presentation so that they are confident in terms of presentation skills and they can address the errors, if any, beforehand. Instead of an online multiple-choice examination (MCQ), it should be on paper, and there should be short answer questions as well. All the facilitators should be tracking slow performers/dormant learners and guiding them more. Peer assessment scoring should be removed or students should be well-trained before they do so.
Limitation
The approach of Sc-SDL has been conducted in one department of an institute, so there is a scope for expanding this research work. Also, interviewing different stakeholders to know their perspectives on this student-centric approach will provide clarity about the approach.
CONCLUSION
The Sc-SDL approach is an acceptable way of encouraging undergraduate students to attain attributional and social skills, which subsequently promotes them toward the path of being lifelong learners rather than having a cognitive gain. The approach allows learners to adapt to the recent trends of digital technology and makes them ready for futuristic web-based knowledge attainment.
Acknowledgement
The authors would like to thank all the participants of the study MBBS batch 2020–2021 for contributing to this newer approach of student-centric approach and providing their valuable feedback for the same. Special thanks to all the faculty members of the departments for following the sequence of the Sc-SDL module and contributing to its betterment. Hearty thanks to Dr. S. Ghosh for peer-reviewing the manuscript and providing her input for the script.
Ethical approval
The research/study approved by the Institutional Review Board at Bhaikaka University, number IEC/BU/2021/Ex. 42, dated 10 November, 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Ekalavya In: Jaya: An illustrated retelling of the Mahabharata. United Kingdom: Penguin Books; 2010. p. :64-5. Available from: https://kupdf.net/download/devduttpattanaik-jaya-pdf_590a0eb6dc0d60057a959e8f_pdf [Last assessed on 2021 Sep 20]
- [Google Scholar]
- Economic feasibility of parallel education policies in India. Agro Econo An Int J. 2020;7:57-61.
- [CrossRef] [Google Scholar]
- 1997 MCI-34(41)/2019-Med./161726 2019. Available from: https://www.nmc.org.in/activitiwebclient/open/getdocument?path=/documents/public/portal/gazette/gme-06.11.2019.pdf [Last assessed on 2020 Mar 10]
- [Google Scholar]
- Competency-based undergraduate curriculum for the Indian medical graduate. . 2019;1-3 Available from: https://www.nmc.org.in/information-desk/forcolleges/ug-curriculum [Last assessed on 2020 Mar 10]
- [Google Scholar]
- Self-directed learning: A guide for learners and teachers United States of America: Association Press; 1975.
- [Google Scholar]
- Self-directed learning: Merging theory and practice In: Long HB, ed. Self-directed learning merging theory and practice. Norman, OK: Research Center for Continuing Professional and Higher Education of the University of Oklahoma; 1989. p. :1-12.
- [Google Scholar]
- Self-direction for lifelong learning: A comprehensive guide to theory and practice San Francisco, CA: Jossey-Bass; 1991.
- [Google Scholar]
- Self-direction in adult learning: Perspectives on theory, research, and practice New York: Routledge; 1991.
- [Google Scholar]
- Self-directed learning: Toward a comprehensive model. Adult Educ Q. 1997;48:18-33.
- [CrossRef] [Google Scholar]
- Instructional-design theory for fostering self-directed learning; Ph.D. thesis. 2003. Indiana University. Available from: https://www.proquest.com/docview/305333004 [Last assessed on 2022 Mar 12]
- [Google Scholar]
- Self-directed learning: A tool for lifelong learning. J Mark Educ. 2014;36:20-32.
- [CrossRef] [Google Scholar]
- The concept of self-directed learning: Implications for practice in the undergraduate curriculum. Indian Pediatr. 2022;59:331-8.
- [CrossRef] [PubMed] [Google Scholar]
- Development of a supported self-directed learning approach for anatomy education. Anat Sci Educ. 2012;5:114-21.
- [CrossRef] [PubMed] [Google Scholar]
- Integrating cooperative learning into the combined blended learning design model: Implications for students' intrinsic motivation. Int J Mob Blended Learn. 2019;11:58-73.
- [CrossRef] [Google Scholar]
- Significance of self-directed learning. Available from: https://www.researchgate.net/publication/335096519_significance_of_self-directed_learning [Last accessed on 2023 Mar 07]
- [Google Scholar]
- Case-based learning in endocrine physiology: An approach toward self-directed learning and the development of soft skills in medical students. Adv Physiol Educ. 2013;37:356-60.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of team-based learning on student self-directed learning Ann Arbor: ProQuest LLC; 2015.
- [Google Scholar]
- Foundations of problem-based learning Maidenhead: Society for Research into Higher Education and Open University Press; 2004.
- [Google Scholar]
- Student learning strategies, mental models and learning outcomes in problem-based and traditional curricula in medicine. Med Teach. 2006;28:717-22.
- [CrossRef] [PubMed] [Google Scholar]
- Managing Problem-based learning: Challenges and solutions for educational practice. Asian Soc Sci. 2015;11:259-70.
- [CrossRef] [Google Scholar]
- Triple Cs of self-directed learning: Concept, conduct, and curriculum placement. CHRISMED J Health Res. 2020;7:235-9.
- [CrossRef] [Google Scholar]
- Self-directed learning theory to practice: A footstep towards the path of being a life-long learne. J Adv Med Educ Prof. 2022;10:135-44.
- [Google Scholar]
- Problems of medical education in India. Int J Community Med Public Health. 2016;3:1905-9.
- [CrossRef] [Google Scholar]
- An educational psychology success story: Social Interdependence theory and cooperative learning. Educ Res Rev. 2009;38:365-79.
- [CrossRef] [Google Scholar]
- Teaching group dynamics--do we know what we are doing? An approach to evaluation. Med Teach. 2008;30:55-61.
- [CrossRef] [PubMed] [Google Scholar]
- How group dynamics research can inform the theory and practice of postsecondary small group learning. Educ Psychol Rev. 2007;19:31-47.
- [CrossRef] [Google Scholar]
- An investigation of self-directed learning skills of undergraduate students. Front Psychol. 2018;9:2324.
- [CrossRef] [PubMed] [Google Scholar]
- Educational handbook for health personnel. 1998. Switzerland: World Health Organization; Available from: https://apps.who.int/iris/bitstream/handle/10665/42118/924170635X_eng.pdf?sequence=1&isallowed=y [Last accessed on 2021 Oct 22]
- [Google Scholar]
- Thematic analysis of qualitative data: AMEE Guide No. 131. Med Teach. 2020;42:846-54.
- [CrossRef] [PubMed] [Google Scholar]
- Engaging medical undergraduates in question making: A novel way to reinforcing learning in physiology. Adv Physiol Educ. 2016;40:398-401.
- [CrossRef] [PubMed] [Google Scholar]
- Self-directed learning can outperform direct instruction in the course of a modern German medical curriculum-results of a mixed methods trial. BMC Med Educ. 2016;16:158.
- [CrossRef] [Google Scholar]
- Self-directed learning in gross human anatomy: Assessment outcomes and student perceptions. Anat Sci Educ. 2008;1:145-53.
- [CrossRef] [PubMed] [Google Scholar]
- Loosely-guided, self-directed learning versus strictly-guided, station-based learning in gross anatomy laboratory sessions. Anat Sci Educ. 2012;5:340-6.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of self-directed learning versus instructor-modeled learning during a simulated clinical experience. Simul Healthc. 2007;2:170-7.
- [CrossRef] [PubMed] [Google Scholar]
- A new perspective on competencies for self-directed learning. J Nurs Educ. 2002;41:25-31.
- [CrossRef] [PubMed] [Google Scholar]
- Implementation and evaluation of a self-directed learning activity for first-year medical students. Med Educ Online. 2020;25:1717780.
- [CrossRef] [PubMed] [Google Scholar]
- Approbation of self-directed learning by first-year medical students: A mixed-method study. MedRxiv 2021
- [CrossRef] [Google Scholar]
- Module to facilitate self-directed learning among medical undergraduates: Development and implementation. J Educ Health Promot. 2020;9:231.
- [CrossRef] [PubMed] [Google Scholar]
- The effectiveness of self-directed learning in health professions education: A systematic review. Med Educ. 2010;44:1057-68.
- [CrossRef] [PubMed] [Google Scholar]




