
Translate this page into:
Aspiration pneumonia induced by haloperidol – A case report
*Corresponding author: K. Saranraj, Department of Pharmacology, Rangaraya Medical College, Kakinada, Andhra Pradesh, India. drsaranmbbs@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Saranraj K, Usha Kiran P, Rohindh K. Aspiration pneumonia induced by haloperidol – A case report. Indian J Physiol Pharmacol. 2024;68:340-3. doi: 10.25259/IJPP_163_2024
Abstract
Antipsychotic drugs were the most common cause of drug-induced aspiration pneumonia and dystonia. We present a young male in his 20s with a medical history of psychosis and on treatment with haloperidol 2.5 mg once daily for the past 3 months, who presented with breathing difficulty, cough, dysphagia and dystonia. The patient was admitted to the pulmonology ward, and investigations included chest X-ray and sputum tests, ruling out infective growth. Bronchoscopic removal of aspirated contents was done, oxygen support and intravenous antibiotics to prevent secondary infections were also given to the patient. The patient recovered fully, prompting haloperidol discontinuation and a switch to another antipsychotic. Pharmacovigilance data underscored haloperidol’s association with adverse reactions such as dystonia and pneumonia. The outcome emphasised the importance of vigilant monitoring and awareness of haloperidol-induced side effects among healthcare professionals and patients.
Keywords
Haloperidol
Dystonia
Aspiration pneumonia
Pharmacovigilance

INTRODUCTION
Aspiration pneumonia arises mainly from lung infections due to the inhalation or aspiration of non-air substances such as liquid, saliva or food. Factors such as general anaesthesia, bedridden conditions and certain medications like antipsychotics can contribute. Dystonia, characterised by involuntary muscle contractions, results from disorganised motor activity, often linked to basal ganglia lesions. Antidopaminergic therapies can also trigger dystonia. It manifests as twisting movements and abnormal posture, categorised by age of onset and body distribution. Treatment may involve deep brain stimulation or surgical ablation. Understanding these conditions is crucial for effective management and minimising drug-induced adverse events.[1] Reporting known adverse reactions is essential for pharmacovigilance and patient safety, as it allows for the identification of potential risks associated with medication usage. By documenting and disseminating such adverse reactions, healthcare professionals can enhance their understanding of drug safety profiles, improve patient care and contribute to the development of safer treatment strategies.
CASE REPORT
The young male, in his 20s, presented to the pulmonology outpatient department with breathing difficulty, cough, dysphagia and muscle stiffness in the neck and upper limbs for 2 days. He had a history of psychosis and was taking haloperidol 2.5 mg and alprazolam 0.5 mg at bedtime for the past 3 weeks. Physical examination revealed dystonia of neck and upper limb muscles, dyspnoea and bilateral lung basal crepitations. Chest X-ray showed bilateral lower zone heterogeneous opacities, diagnosing aspiration pneumonia and haloperidol-induced dystonia. Dechallenge was positive, indicating a probable adverse drug reaction (ADR), reported through World Health Organization (WHO) Vigiflow, where haloperidol was commonly associated with dystonia and aspiration pneumonia, with 36,122 and 283 cases reported, respectively, along with 2345 cases of haloperidol-induced dystonia.[2] The patient’s symptoms improved post-haloperidol cessation, confirmed by positive dechallenge and ethical constraints prevented rechallenge. Permission for the publication of this case report has been obtained from the Institutional Ethics Committee affiliated with Rangaraya Medical College, associated with the Government General Hospital, Kakinada Andhra Pradesh. The Institutional Ethics Committee registration number is IEC/RMC/2024/1269. Assessment using both the WHO–Uppsala Monitoring Centre[3] and the Naranjo ADR probability scale [4] categorises it as a probable reaction. Specifically, the Naranjo ADR probability scale yielded a score of +7, indicating a probable reaction [Table 1].[5]
| Interrogation | Yes | No | Unknown/not available | Score |
|---|---|---|---|---|
| Are there previously confirmed reports of reaction? | +1 | 0 | 0 | 0 |
| Did the adverse event appear after the drug was used? | +2 | −1 | 0 | +2 |
| Did the adverse reaction improve when the medicine was withdrawn or a specific antagonist was used? | +1 | 0 | 0 | +1 |
| Were there other feasible causes for the reaction? | −1 | +2 | 0 | +2 |
| Did the adverse reaction appear again on administration of a placebo? | −1 | +1 | 0 | +1 |
| Was the medicine determined in the blood or other fluids in toxic concentrations? | +1 | 0 | 0 | 0 |
| Was the reaction worsened by increasing the dose? Or was the reaction lessened by decreasing the dose? | +1 | 0 | 0 | 0 |
| Did the adverse reaction appear again on re-administering the drug? | +2 | −1 | 0 | 0 |
| Did the patient have an identical reaction to the medicine or a related agent in the past? | +1 | 0 | 0 | 0 |
| Was the adverse event confirmed by any other objective evidence? | +1 | 0 | 0 | +1 |
| Total score | +7 | |||
ADR: Adverse drug reaction
Differential diagnosis
During the patient’s assessment, several potential diagnoses were considered, including chronic bronchitis, acute laryngotracheobronchitis, tuberculous pneumonia, infective bacterial pneumonia, COVID-19 pneumonia and drug-induced aspiration pneumonitis. Following a comprehensive evaluation encompassing physical examination, systemic assessment, haematological analyses and radiological and microbiological investigations, all potential diagnoses were meticulously ruled out, leading to the conclusive diagnosis of drug-induced aspiration pneumonitis. The investigative process involved a series of tests:
-
A chest X-ray revealed bilateral lower zone heterogeneous opacities [Figure 1]
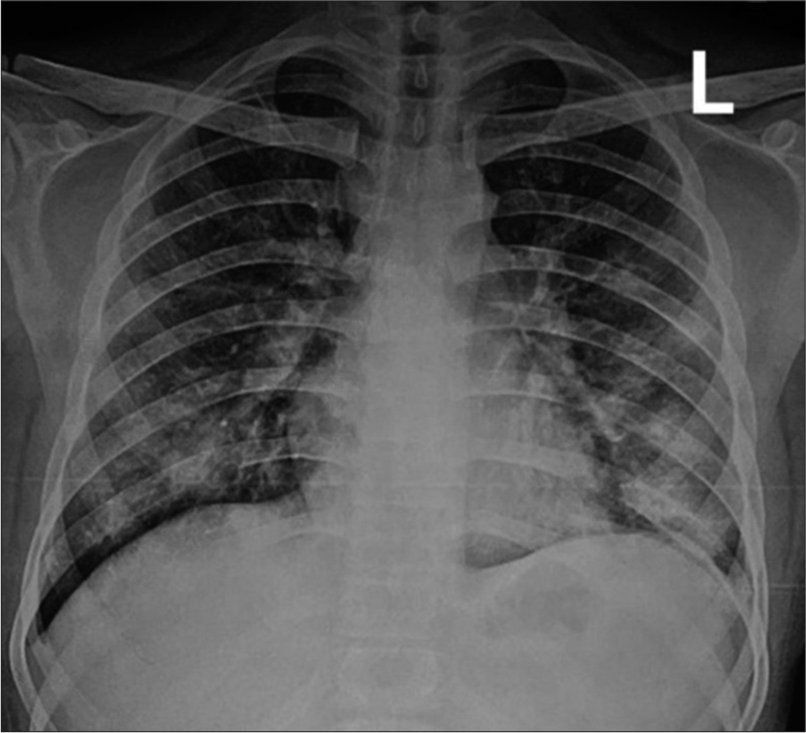 Figure 1:
Figure 1:- Chest X-ray of the patient denotes bilateral lower zone heterogeneous opacities.
COVID-19 reverse transcription polymerase chain reaction testing yielded negative results
Sputum samples for CBNAAT/GENE XPERT testing returned negative results
Sputum culture and sensitivity testing indicated no evidence of infective growth
Bronchoscopic aspiration lavage fluid was subjected to Gram staining, bacterial culture and sensitivity and fungal culture and sensitivity, all of which exhibited negative findings with no observable growth.
Treatment and follow-up
Aspiration pneumonia was treated with the removal of aspirated contents from the lung by bronchoscopic lavage, medications such as metronidazole 500 mg intravenous injection 3 times a day (TDS), gentamycin injection 80 mg given through intravenous route twice daily (BD) and oxygen therapy given according to the patient’s requirement. Dystonia was treated with high-dose anticholinergics (trihexyphenidyl). Physiotherapy also started to decrease the risk of re-aspiration due to bedridden conditions. On day 6 of hospital admission, the patient recovered completely from aspiration pneumonia, dysphagia and dystonia. The patient was discharged on the 6th day of hospital admission with oral medications. An antipsychotic drug was changed, neurology consultation was sought, and the patient was informed to come for a follow-up after 1 week. During the follow-up, the patient expressed comfort and did not report any haloperidol-related side effects. In addition, symptoms such as dysphagia and neck muscle stiffness markedly decreased upon follow-up. Since the patient’s condition improved notably on discontinuation of haloperidol, additional investigations into alternative causes of aspiration pneumonitis, such as gastroesophageal reflux disease, were not pursued in our study.
DISCUSSION
Drug safety is a primary concern of public health, and it can be continuously monitored by the pharmacovigilance ADR reporting system. We can quantify, qualify and decrease drug-related adverse events with the help of the pharmacovigilance ADR reporting system. For many years, adverse events related to antipsychotic drugs have been investigated using pharmacovigilance programs such as spontaneous reporting systems and electronic medical records. The reliability of the association between drug adverse reactions and drug use is strengthened by confirming the drug’s mechanism of action and drug-receptor interactions, especially in ‘type A’ adverse drug events, which are dose-dependent and based on the pharmacological properties of the drug effects.[1]
The onset of aspiration pneumonia typically occurs within a range of 2–5 days, a timeframe that can vary depending on factors such as the patient’s age, underlying health conditions and additional contributing factors. Due to limitations in the patient’s history, a time-to-event analysis correlating the administration of haloperidol with the onset of aspiration pneumonitis could not be conducted in our study. The likelihood of developing aspiration pneumonia is elevated in patients undergoing combination therapy involving benzodiazepines, barbiturates and antihistamines alongside antipsychotics compared to those receiving antipsychotic monotherapy.[6] In our case report, the patient was prescribed alprazolam, a benzodiazepine, which poses a considerably lower risk of causing aspiration pneumonitis compared to all other benzodiazepines, including diazepam and midazolam.[7] Therefore, in our study, alprazolam was not discontinued due to its lower propensity to induce aspiration. Instead, haloperidol was ceased on hospital admission, and supportive treatment was administered. As a result, the patient’s symptoms improved, leading to discharge. Thus, in our investigation, haloperidol was identified as the primary cause of aspiration pneumonitis.
Haloperidol is commonly used for bipolar disorder, schizophrenia and psychosis.[8] It is a potent typical antipsychotic drug that competitively blocks post-synaptic D2 dopamine receptors and also blocks D1, D4, H1, α1, M1 and 5HT2A receptors.[9,10] Haloperidol is the most important antipsychotic drug that causes more extrapyramidal symptoms, especially dystonia, due to its high affinity for D2 receptors. It causes adverse effects such as dysphagia and aspiration pneumonia, leading to higher mortality.[11,12] Patients prescribed haloperidol have a higher mortality rate than those prescribed other antipsychotic drugs.[9] Moreover, this risk is further escalated among elderly individuals as opposed to younger patients.[13,14]
Haloperidol can cause aspiration pneumonia through several mechanisms, including its high affinity toward D2 dopamine receptor blockade, which leads to many extrapyramidal symptoms such as dystonia, dysphagia, dyskinesia of oropharyngeal muscles, rigidity and spasm of pharyngeal muscles and sedation.[15] These effects suppress the cough reflex and increase the risk of aspiration pneumonia due to the aspiration of saliva, foreign bodies, food particles and gastric contents.[16,17] D2 receptor blockade also causes dry mouth in some patients, leading to impaired oropharyngeal bolus transport and contributing to the occurrence of aspiration pneumonia.[12] Sometimes, antipsychotics paradoxically cause hypersalivation due to disrupted cholinergic function, increasing the risk of aspiration pneumonia in patients taking antipsychotic medications. Haloperidol has also been associated with a decreased level of substance P, which impairs the swallowing reflex and increases the risk of aspiration pneumonia.[15] Its antihistamine effects, such as sedation and sometimes dysphagia, occur due to the H1 receptor-blocking activity of haloperidol, which also increases the risk of aspiration pneumonia. Thromboxane A2 receptor and platelet-activating factor receptor are novel antipsychotic drug target receptors potentially associated with pneumonia, with affinity observed for all antipsychotic drugs except amisulpride.[1]
CONCLUSION
Haloperidol, the most commonly prescribed antipsychotic medication, poses numerous serious complications, including extrapyramidal symptoms, cardiovascular issues and aspiration pneumonia. Clinicians should evaluate patients for their susceptibility to pneumonia and cardiovascular events before prescribing haloperidol. Vigilant monitoring of patients on antipsychotic medications for haloperidol’s adverse effects is crucial. Health-care providers should thoroughly explain the potentially severe side effects of haloperidol treatment to both patients and their relatives. Given the potentially fatal complications such as dystonia and aspiration pneumonia associated with haloperidol, it is imperative to raise awareness among patients and their families regarding the symptoms of haloperidol-induced side effects.
Patient’s/patient guardian’s perspective
My son has been taking psychiatric medications such as tablet haloperidol and tablet alprazolam once daily at bedtime for the past 3 weeks. Over the past 7 days, he gradually developed stiffness in the neck and upper limb muscles, along with coughing, difficulty swallowing and breathing issues for the past 2 days. Concerned, I took him to the pulmonology outpatient department and consulted with the doctor. After examination, the doctors admitted him to the hospital ward and administered intravenous medications and oxygen therapy. They informed me that these symptoms were likely due to the tablet haloperidol and decided to change his psychiatric medication. He was discharged from the hospital on the 6th day of admission with oral medications.
Ethical approval
The research/study was approved by the Institutional Review Board at Rangaraya Medical College and Government General Hospital, Andhra Pradesh, number IEC/RMC/2024/1269, dated 16th April 2024.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Biological substantiation of antipsychotic-associated pneumonia: Systematic literature review and computational analyses. PLoS One. 2017;12:e0187034.
- [CrossRef] [PubMed] [Google Scholar]
- Vigiaccess data. Available from: https://www.vigiaccess.org [Last accessed on 2024 Apr 09]
- [Google Scholar]
- Available from: https://www.who.int/publications/m/item/who-causality-assessment [Last accessed on 2024 Apr 09]
- A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239-45.
- [CrossRef] [PubMed] [Google Scholar]
- Classifying causality of an audverse drug reaction: Naranjo algorithm. Int J Pharmacy Chem. 2021;7:125-7.
- [CrossRef] [Google Scholar]
- Pneumonia risk associated with the use of individual benzodiazepines and benzodiazepine related drugs among the elderly with Parkinson's Disease. Int J Environ Res Public Health. 2021;18:9410.
- [CrossRef] [PubMed] [Google Scholar]
- Haloperidol induced dystonia: A case report. J Chalmeda Anand Rao Inst Med Sci. 2017;13:31.
- [Google Scholar]
- Haloperidol-induced isolated lingual dystonia. BMJ Case Rep. 2021;14:e242272.
- [CrossRef] [PubMed] [Google Scholar]
- Exploring a safety signal of antipsychotic-associated pneumonia: A pharmacovigilancepharmacodynamic study. Schizophr Bull. 2021;47:672-81.
- [CrossRef] [PubMed] [Google Scholar]
- Mortality risk associated with haloperidol use compared with other antipsychotics: An 11-year population-based propensity-score-matched cohort study. CNS Drugs. 2020;34:197-206.
- [CrossRef] [PubMed] [Google Scholar]
- Risk of pneumonia is associated with antipsychotic drug use among older patients with Parkinson's disease: A case-control study. Int J Med Sci. 2021;18:3565.
- [CrossRef] [PubMed] [Google Scholar]
- Antipsychotics and the risk of aspiration pneumonia in individuals hospitalized for nonpsychiatric conditions: A cohort study. J Am Geriatr Soc. 2017;65:2580-6.
- [CrossRef] [PubMed] [Google Scholar]
- Extrapyramidal syndrome presenting as dysphagia: A case report. Am J Hosp Palliat Med. 2008;25:398-400.
- [CrossRef] [PubMed] [Google Scholar]
- Antipsychotic drug use and pneumonia: Systematic review and meta-analysis. J Psychopharmacol. 2018;32:1167-81.
- [CrossRef] [PubMed] [Google Scholar]
- Antipsychotic drug use and risk of pneumonia in elderly people. J Am Geriatr Soc. 2008;56:661-6.
- [CrossRef] [PubMed] [Google Scholar]
- Neuroleptic-induced dysphagia: Case report and literature review. Dysphagia. 2007;22:63-7.
- [CrossRef] [PubMed] [Google Scholar]




