
Translate this page into:
Effectiveness of Rajyoga meditation on cognitive functions and quality of life in young adults with internet addiction
*Corresponding author: Dr. Preeti Jain, Professor, Department of Physiology, Maulana Azad Medical College and Associated Hospitals, New Delhi, India. drpreetijain@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bansal S, Jain P, Tomar R, Kapoor M. Effectiveness of rajyoga meditation on cognitive functions and quality of life in young adults with internet addiction. Indian J Physiol Pharmacol. 2024;68:288-97. doi: 10.25259/IJPP_188_2024
Abstract
Objectives:
Recently, an increasing trend in the prevalence of internet addiction (IA) has been seen worldwide. IA is found to be associated with impaired cognitive functions, emotional dysregulations and psychological morbidity, warranting the need for appropriate preventive and curative interventional modalities. Nonpharmacological interventions such as meditation may help in positively modifying internet behaviour and combatting its adverse effects on cognitive functions and psycho-social health. The purpose of the study was to assess the influence of Rajyoga meditation (RYM) on cognition and quality of life (QOL) in young adults with IA.
Materials and Methods:
In the present prospective interventional study, a total of 40 young adults with IA were divided equally into two groups: Control and meditation. Subjects in the meditation group practised RYM for 20 min/day, daily for 8 weeks. Control group subjects received no intervention. Assessments were conducted thrice at the following time points: Before intervention (baseline), after 1 week (T1) and 8 (T2) weeks of intervention. Various assessment tools such as Young’s 20-Item IA Test (YIAT), World Health Organization QOL brief (WHOQOL-Bref) and Montreal cognitive assessment (MOCA) questionnaires were utilised. The statistical analysis was performed using the Statistical Package for the Social Sciences version 25.0 (IBM Corp).
Results:
Baseline characteristics were similar in both groups. The results revealed significant (P < 0.001) main effects of time for YIAT and MOCA. This effect was further qualified by a significant interaction between time and group for YIAT (P < 0.001). The results further highlighted significant between groups effects in mean scores of YIAT, MOCA (P < 0.01) and WHOQOL-Bref domains 2, 4 (P < 0.01) and domain 3 (P < 0.05) after 8 weeks of intervention. Within the meditation group, a significant increase in mean scores of both MOCA (P < 0.01) and WHOQOL-Bref (P < 0.05) and a significant decrease in mean YIAT (P < 0.001) scores were observed after 8 weeks of intervention.
Conclusion:
RYM decreased the severity of IA as indexed by YIAT and improved the overall cognitive function and QOL in young adults with IA, as evidenced by MOCA and WHOQOL-Bref, respectively. These findings indicate that RYM was effective in ameliorating the negative effects of IA and can serve as a useful preventive and curative non-pharmacological interventional modality for promoting cognitive and psycho-social well-being in subjects with IA disorder.
Keywords
Internet addiction
World Health Organization quality of life
Cognition
Montreal cognitive assessment
Rajyoga meditation

INTRODUCTION
There has been a global increase in internet usage within the past two decades, with approximately 5.4 billion (67%) of the world’s population using the internet for various recreational and work-related activities.[1] However, this ubiquitous presence of the internet has raised concerns regarding the ill effects of its excessive usage and the emerging problem of internet addiction (IA). IA, often referred to as problematic internet use (PIU), is a rapidly increasing behavioural disorder defined as ‘an uncontrollable psychological dependence on the internet, regardless of the type of activities pursued after logging in’.[2] This heterogeneous problem is marked by an excessive preoccupation with online activities such as internet gaming, social networking, compulsive online shopping, information seeking and even cyber-relationship addiction. This maladaptive pattern of internet overuse leads to negative consequences in various aspects of life, including interpersonal relationships and the overall well-being of an individual.[3] In addition, clinically significant impairments in physical and mental health, co-occurrence of emotional dysregulations, psychological distress and comorbid disorders such as drug or alcohol abuse, anorexia or bulimia and attention deficit hyperactivity disorder have also been reported with PIU.[4] Furthermore, the diagnostic criteria currently available for IA parallel the criteria commonly used for diagnosing substance use disorder, incorporating features such as escalating use over time, loss of control, concealing excessive use from others, failed attempts to cut back, psychological distress, cravings and withdrawal symptoms when/if prevented from using the internet.[5] In 2018, the WHO also recognised IA as an official mental health disorder and behavioural addiction and included it under ‘Disorders Due to Addictive Behaviours’ in the International Classification of Diseases 11th Revision as internet gaming disorder (IGD).[6] As per a recent meta-analysis, the global prevalence of IA in the general population is about 14%.[7]
Cognition pertains to the set of all mental abilities and processes involved in the acquisition, processing, storage and retrieval of information by the brain. It is composed of basic cognitive functions such as alertness, higher cognitive abilities such as attention, executive functioning, perception and memory as well as critical elements such as verbal, language and motor skills.[8] The effects of internet usage on the cognitive functions of an individual are multifaceted. Evidence from the majority of prior studies done on individuals who play online games has shown beneficial effects on the visuospatial skills, working memory and decision-making skills of an internet gamer.[9] In contrast, case-control studies examining the cognitive performance of individuals with PIU have found that enhanced use of the internet is significantly associated with deficits in alertness, attentional inhibition, motor inhibition, decision-making and working memory.[10] Moreover, reductions in executive functioning and inhibitory control contribute to engagement in online behaviours, providing gratification and ultimately leading to the emergence and persistence of PIU.[11]
Quality of life (QOL) is a multidimensional concept composed of domains related to physical, mental, emotional and social functioning; being influenced by personal characteristics and environmental factors.[12] An emerging body of multidisciplinary studies that have examined the effects of overuse of the internet has indicated a causal link between IA and impairment of QOL.[13] An increase in self-isolation, feelings of loneliness, depressive mood, anxiety disorders, suicidal behaviours,[14] poor academic performance, sleep disorders and a sedentary lifestyle have been demonstrated among problematic internet users.[15] However, this is not a universal finding, and the positive impact of internet usage on developing interpersonal relationships with family and friends has also been reported.[16]
Considering that internet usage is fast becoming an indispensable part of modern-day society, calls for solutions to prevent and combat IA, especially in adolescents and young adults, are on the rise. Appropriate IA preventive measures are needed to encourage individuals to have more control over their internet usage and help them to positively modify their internet behaviour by strengthening their capability of self-awareness and self-control.[17]
Mindfulness meditation is a mind-body type of nonpharmacological behavioural therapy that aims to give a sense of calmness, inner peace, and emotional balance[18] and can also improve cognitive performance.[19] This therapy helps individuals improve their self-regulation skills. Prior studies have put forth evidence highlighting the beneficial effects of various mindfulness meditation techniques in non-clinical settings.[18-21] Recently, the usefulness of this technique has also been explored in clinical settings, including addictive behaviours.[22] Rajyoga meditation (RYM) is a very simple form of meditation performed without rituals or mantra recitation and can be practised anywhere at any time. In this technique, an emphasis is placed on naturally using the mind to concentrate on the present moment, shifting focus from negative thoughts and empowering the mind by promoting positive thought patterns and feelings.[23] Hence, RYM, with its emphasis on mental discipline, emotional regulation and stress reduction, may prove to be beneficial in terms of prevention, harm reduction and intervention toward addictive internet behaviour.
Therefore, in the present study, we focused on assessing and comparing the influence of RYM on cognitive status and QOL in young adults with IA. By investigating the effectiveness of this non-pharmacological intervention, we seek to provide valuable insights into the potential beneficial role of meditation in combatting the adverse effects of IA and enhancing cognitive functions and psychosocial health.
MATERIALS AND METHODS
Study design
The present study was a non-randomised, prospective and two-armed parallel-group interventional comparative trial conducted from April 2021 to March 2022 (12 months). There were an equal number of participants (20 each) in the control and meditation groups. Participants in the meditation group practised RYM for 20 min/day, daily for 8 weeks. Control group subjects received no intervention. Assessments were conducted thrice at the following time points: Before intervention (baseline), after 1 week (T1) and 8 (T2) weeks of intervention.
Study settings
The study was approved by the Institutional Ethical Committee (approval number: IEC 2020/No. 158) and took place in the Department of Physiology, Maulana Azad Medical College, New Delhi, in an online format. The duly filled informed consent was taken after explaining the research design to the participants.
Participants
The students and staff of our institute were invited to participate in this study through electronic communication. Two hundred eighty-seven respondents were screened based on age, the ability to read English letters, words and numerals, the internet usage questionnaire and Young’s IA Test (YIAT).[2] Forty participants in the age group of 18– 30 years who scored more than 30 on YIAT were included in the study. These individuals were selected from a pool of 87 young adult internet addicts. Those participants who engaged in any form of meditation practice in the past 3 months or had any previous exposure to cognitive testing were excluded from the study. Three months of meditation program has been shown to improve cognitive functions significantly.[24] Hence, the rationale for such exclusion was to limit the confounding effect of prior meditation training/practice on cognition, which could skew the results and undermine the study’s validity. Nine respondents practised Om chanting, 15 did pranayama and eight performed breathing exercises and were excluded from the study. Those suffering from any acute physical or mental illness or those who were on any medication that could likely affect cognition were also excluded from the study. No incentive was given to the participants to take part in this study.
Meditation intervention
The participants in the meditation group attended online meditation training sessions for 2 consecutive days. Each session was of 20 min duration in which they were introduced to and taught the RYM technique following BrahmaKumaris (BK) school of thought. BK RYM is based on the philosophy of self-actualisation and self-mastery. It is practised within a framework of the following four different limbs, namely, (i) Gyan (Knowledge/Wisdom of self and Supreme soul); (ii) Yog (Meditation including aspects of concentration, mindfulness, compassion and visualisation); (iii) Dharana (Inculcation and practice of virtues in daily lifestyle) and (iv) Seva (Service which includes having good wishes/actions for self and others). Visualisation as a tool was used in Yog, focus attention was applied in Gyan and open monitoring was used in Dharana and Seva.
The RYM session protocol included seven domains (based on the four limbs of BK RYM), which were tailored specifically for IA by a team of well-trained, long-term (>20 years) Rajyoga meditators. The details of the RYM protocol are given in Table 1. Each session of RYM lasted for 20 minutes. Hand-outs/audio videos of the commentary were given to them. They were asked to do RYM in sitting posture with eyes open, be in an alert state and follow the instructions throughout the meditation sessions. Participants were asked to continue regular guided RYM through audio commentary for 20 min per day for the next 8 weeks. For sustenance and compliance, online meditation sessions were held twice a week, every Tuesday and Friday, for 8 weeks. Subjects were asked verbally during online meditation classes and follow-up classes about their compliance. RYM was taught free of cost to the participants by a well-trained practitioner having more than 20 years of professional experience in RYM.
| S. No. | Domain | Duration | Rajyoga meditation limb |
|---|---|---|---|
| 1. | Knowledge and awareness of self | 3 min | Gyan (Focus attention) |
| 2. | Knowledge and awareness of supreme | 3 min | |
| 3. | Knowledge of universal flow of energy | 2 min | |
| 4. | Concentration and observation of self-thoughts | 3 min | Yog (Visualisation) |
| 5. | Visualisation and analysis of self-thoughts | 2 min | |
| 6. | Active creation of positive thoughts | 5 min | Dharana (Open monitoring) |
| 7. | Good wishes for self and others, gratitude | 2 min | Seva (Open monitoring) |
Control group
The participants in this group did not receive any intervention currently or in the past and went about their normal daily routine. In addition, there was no exposure to any meditation practice/nor did they initiate any meditation regimen during the study period.
Assessments
The demographic, internet usage and previous meditation experience data were collected using a structured questionnaire. The data for various outcome variables such as IA, psychological health and QOL was collected using self-reported rating scale questionnaires. Assessment of cognitive functions was done using a battery of neurocognitive tests.
Outcome variables
Young’s IA test (YIAT)
It is a 20-item scale that measures the presence and severity of internet dependency among adults. This self-reported questionnaire measures characteristics and behaviour associated with compulsive use of the internet, including compulsivity, escapism and dependency. Each item is rated on a 5-point scale ranging from 0 to 5 (0 = does not apply, 1 = rarely, 2 = occasionally, 3 = frequently, 4 = often and 5 = always). The maximum score is 100 points. Total scores that range from 0 to 30 points are considered to reflect a normal level of internet usage; scores of 31–49 indicate the presence of a mild level of IA; 50–79 reflect the presence of a moderate level, and scores of 80–100 indicate a severe dependence on the internet.[2] The Cronbach’s alpha coefficient of YIAT in our study was 0.78.
World Health Organization QOL (WHOQOL) questionnaire-bref
This questionnaire was used to assess the quality-of-life profile of the participants. It contains a total of 26 questions that quantifies the subjective QOL in four domains (D1–D4), namely, physical (D1–D7 items), psychological (D2–D6 items), social (D3–D3 items) and environmental (D4–D8 items) health. In addition, two items separately examine the overall QOL and general health facet of the individual. Responses to questions are on a 1–5 Likert scale where 1 represents ‘disagree’ or ‘not at all’ and 5 represents ‘completely agree’ or ‘extremely’. The final score lies on a transformed linear scale between 0 and 100, following the scoring guidelines. A higher score indicates a better QOL.[25] The Cronbach’s alpha coefficient of WHOQOL-Bref in our study was 0.79.
Montreal cognitive assessment (MOCA) questionnaire
It is widely used as a screening tool for detecting mild cognitive impairment. This neurocognitive test assesses the following cognitive domains: (i) visuospatial abilities by having the subject copy a three-dimensional cube (1 point) and draw a clock (3 points); (ii) executive function that includes an alternation task adapted from the Trail Making B test (1 point), a verbal fluency (1 point) and a two-item verbal abstraction task (2 points); (iii) attention by forward and backward digits (1 point each), target detection by tapping (1 point) and a serial subtraction task (3 points); (iv) delayed recall by having the subject complete two trials involving learning nouns and their recall after 5 min (5 points); (v) language by having the subject complete a three-item naming task with animals (3 points), repeat two syntactically complex sentences (2 points) and complete the fluency task mentioned above and (vi) the subject’s orientation in time and place is assessed (6 points). The maximum achievable score is 30, and a score of ≥26 is considered normal.[26]
Sample size
This was a parallel, two-arm, prospective and nonrandomised trial wherein measurements of outcome variables were done 3 times. Accordingly, sample size estimation was done through G*Power 3.119 for a repeated-measures analysis of variance (ANOVA) within-between interactions using a priori power analysis. Aiming for a small to medium effect size (f = 0.25) and a power of 0.80 with an alpha level of 0.05, keeping a correlation among repeated measures of 0.5 and a non-sphericity correction ε of 1, each group would require 14 participants. Factoring a dropout rate of up to 40%, it was determined that a total of 20 participants should be recruited initially in each group. A total of 40 participants with IA were enrolled in this study, 20 of whom were assigned to each group.
Statistical analysis
The collected data were entered, cleaned and systematised using Microsoft Excel Sheets (version 2010). The data were analysed using the Statistical Package for the Social Sciences version 25.0 package (IBM Corporation Business Analytics Software Portfolio, Chicago, Illinois, USA). The normality of distribution was assessed using the Shapiro–Wilk test. Reliability analysis of all measures was done by calculating Cronbach’s alpha. Group-wise descriptive statistics of parameters were computed as mean ± Standard deviation.
Qualitative data were expressed in percentages and statistical differences between the proportions were tested by the Chi-square test or Fisher’s exact test. Separate sets of repeated-measures ANOVA were conducted on YIAT, WHOQOLBref and MOCA. Significant main effects were further analysed using the student’s t-tests, and the Bonferroni adjustment for the number of pairwise comparisons was employed. Greenhouse–Geisser epsilon corrections were used whenever Mauchly’s test of sphericity was violated. For all analyses, P < 0.05 was considered as significant.
RESULTS
There was no statistical difference in the mean age of control (21.80 ± 2.87 years) and meditation (22.70 ± 5.84 years) group participants: χ2 = 13.14, P = 0.52. Gender-wise distribution of participants in the control (M: F = 13:7) and meditation (M: F = 11:9) groups were also not significantly different: χ2 = 0.42, P = 0.51. All the participants in both groups were undergraduate medical students of our institute and belonged to the Delhi-NCR region.
Internet usage behaviour
There was no statistical difference in the mean number of hours spent on the internet per day by participants in the control (5.90 ± 3.58) and meditation (6.35 ± 2.76) groups: χ2 = 3.59, P = 0.31. There was also no significant difference in the mean number of years of internet usage in the control (7.50 ± 3.35) and meditation (8.85 ± 3.08) group participants: χ2 =1.69, P = 0.43. All the participants in both groups accessed the internet on either mobile phones and laptops or personal computers. Ninety per cent of the participants used the Internet for various purposes, including education, information acquisition, gaming, messaging and chatting. Only 10% used it for other purposes, such as watching movies or online shopping.
Young’s IA test
Analysis of the YIAT data revealed a significant main effect of time (P < 0.001) and group (P < 0.05). These effects were further qualified by a significant interaction between time and group (P < 0.001) [Table 2]. There was a significant difference between the mean YIAT scores of the participants in the two study groups at both T1 and T2 times (P < 0.05 and 0.01), respectively. Within the same group, participants of both study groups showed a significant decrease in their IAT scores at T1 (P < 0.01 and <0.001 for control and meditation, respectively) as well as at T2 (P < 0.001 for both) in comparison to their baseline scores. There was also a significant difference (P < 0.001) between their mean IAT scores at 1 week and those at 8 weeks within both the study groups [Figure 1].
| Variable | Time | Group | Time X Group | |||
|---|---|---|---|---|---|---|
| F (df) | P | F (df) | P | F (df) | P | |
| YIAT | 158.92 (1.34, 51.06) | <0.001*** | 4.62 (1,38) | <0.05* | 34.49 (1.34, 51.06) | <0.001*** |
| Overall QOL | 33.83 (1.61, 61.06) | <0.001*** | 0.62 (1,38) | >0.05 | 2.03 (1.61, 61.06) | >0.05 |
| General Health | 33.93 (1.49, 56.44) | <0.001*** | 0.63 (1,38) | >0.05 | 9.15 (1.49, 56.44) | <0.01** |
| D1 | 29.52 (1.47, 55.96) | <0.001*** | 0.56 (1,38) | >0.05 | 3.73 (1.47, 55.96) | <0.05* |
| D2 | 21.06 (1.73, 65.78) | <0.001*** | 0.01 (1,38) | >0.05 | 15.06 (1.73, 65.78) | <0.001*** |
| D3 | 14.99 (1.42, 53.98) | <0.001*** | 0.28 (1,38) | >0.05 | 0.98 (1.42, 53.98) | >0.05 |
| D4 | 13.41 (1.37, 51.95) | <0.001*** | 1.39 (1,38) | >0.05 | 9.88 (1.37, 51.95) | <0.01** |
| Total MOCA | 27.33 (2, 76) | <0.001*** | 2.03 (1,38) | >0.05 | 15.72 (2,76) | <0.001*** |
| Visuospatial Abilities | 14.14 (1.14, 43.47) | <0.001*** | 1.15 (1,38) | >0.05 | 3.73 (1.14, 43.47) | >0.05 |
| Executive Function | 5.40 (2, 76) | <0.01** | 0.82 (1,38) | >0.05 | 5.40 (2, 76) | <0.01** |
| Attention | 4.03 (1.13, 42.88) | <0.01** | 0.08 (1,38) | >0.05 | 10.39 (1.13, 42.88) | <0.01** |
| Delayed Recall | 4.12 (1.63, 62.09) | <0.05* | 0.01 (1,38) | >0.05 | 2.22 (1.63, 62.09) | >0.05 |
| Language | 3.43 (1.43, 54.38) | >0.05 | 0.56 (1,38) | >0.05 | 0.79 (1.43, 54.38) | >0.05 |
| Orientation | 1.00 (2, 76) | >0.05 | 1.00 (1,38) | >0.05 | 1.00 (2, 76) | >0.05 |
Significantly different (*P<0.05, **P<0.01, ***P<0.001). ANOVA: Analysis of variance, df: Degrees of freedom, YIAT: Young’s internet addiction test, QOL: Quality of life, D1-D4: Four domains of World Health Organization quality of life questionnaire, MOCA: Montreal cognitive assessment questionnaire, WHOQOL: World Health Organization Quality of Life, df: degrees of freedom
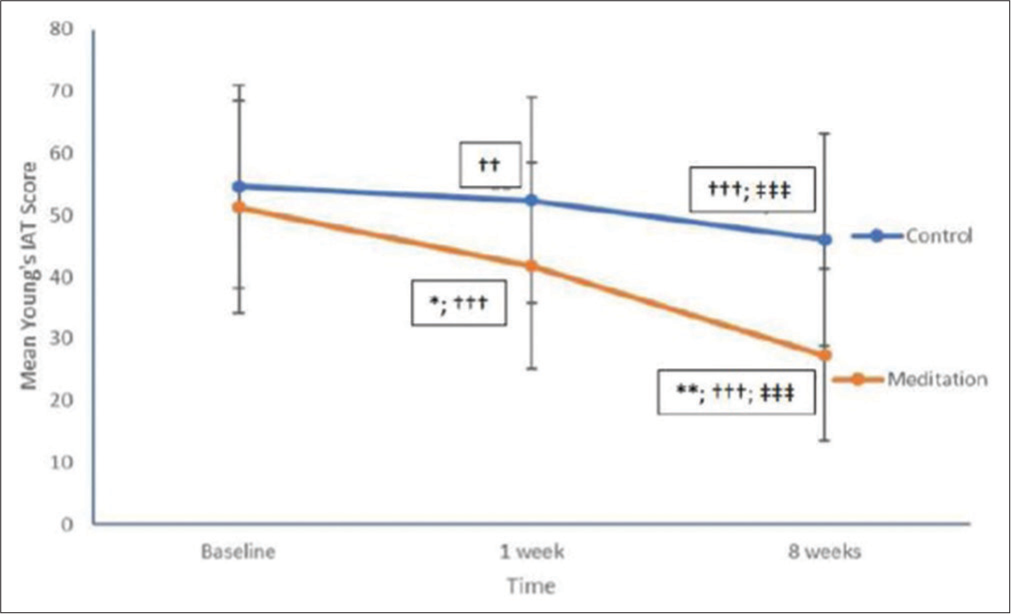
- Young’s 20-Item internet addiction test (IAT) score in participants of both study groups at different time points. n = 20 in each. Data represent Mean ± standard deviation significantly different (*P < 0.05; **P < 0.01) compared to control group Significantly different (††P < 0.01; †††P < 0.001) compared to baseline within group significantly different (‡‡‡P < 0.001) compared to 1 week within group.
The Chi-square test revealed that there was no significant difference in the severity of IA between the participants of the two study groups at baseline and 1 week (χ2 = 1.03 and 6.23, P = 0.60 and 0.10, respectively). However, a significant difference was observed in the severity of IA between participants of control and meditation groups at 8 weeks of study (χ2 = 9.41, P = 0.009) [Figure 2].
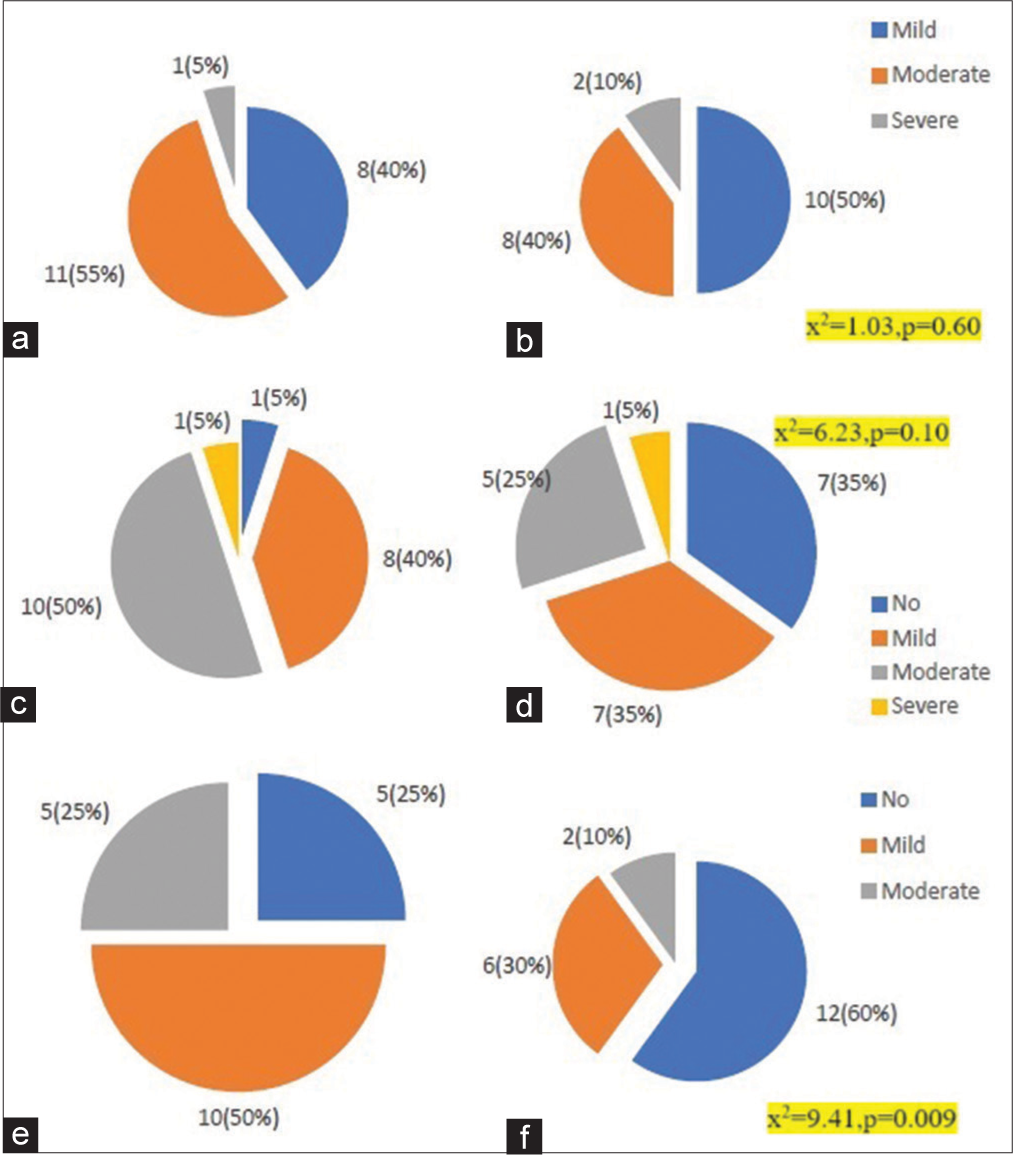
- Internet addiction severity comparison between both groups at different follow-up points. n = 20 in each group. Values are frequency (%). 2a,c,e: Control; 2b,d,f: Meditation; (a and b) Baseline; (c and d) 1 week; (e and f) 8 weeks χ2 Chi-square; P-inter-group difference in severity of internet addiction.
WHOQOL questionnaire- bref
Analysis of the WHOQOL-Bref data revealed that there was a significant main effect of time (P < 0.001) for overall QOL, general health as well as for all its four domains. There was also significant interaction between time and group for D1 (P < 0.05), general health and D4 (P < 0.01) and D2 (P < 0.001) [Table 2].
There was no significant difference (P > 0.05) between the mean D1 scores of the participants in the two study groups at any time point. There was a significant difference (P < 0.05) between the mean general health, D2, D3 and D4 scores of the participants in the two study groups at the T2 time point. Within the same group, participants in the meditation group showed a significant increase in their mean D1, D2 and general health, scores at T1 (<0.05, <0.01 and P < 0.001, respectively) as well as at T2 (P < 0.001) in comparison to their baseline scores. For D3, D4 and overall QOL, a significant increase in their mean scores was observed at T2 (P < 0.001) in comparison to the baseline. There was also a significant difference between their mean domain scores at T1 and T2 (P < 0.001) time points for all four domains as well as overall QOL and general health. No significant difference (P > 0.05) was observed within control group participants at any point in time in WHOQOL-Bref scores [Table 3].
| Parameter | Group | Baseline | T1 | T2 |
|---|---|---|---|---|
| Overall QOL | Control | 74.50±7.56 | 77.90±6.14 | 81.85±5.22 |
| Meditation | 73.40±9.54 | 76.05±8.16 | 81.75±5.84†††; ‡‡‡ | |
| General health | Control | 77.90±8.33 | 82.00±7.06 | 81.85±6.85 |
| Meditation | 72.35±6.41 | 78.20±7.51††† | 84.20±4.89*;†††; ‡‡‡ | |
| Domain 1 | Control | 75.30±9.66 | 77.30±9.47 | 80.10±6.69 |
| Meditation | 72.05±10.53 | 73.80±9.41† | 81.15±5.34†††; ‡‡‡ | |
| Domain 2 | Control | 76.60±7.34 | 77.80±6.90 | 79.90±4.89 |
| Meditation | 70.80±9.44 | 77.50±8.34†† | 83.15±6.12*; †††; ‡‡‡ | |
| Domain 3 | Control | 75.20±7.55 | 78.30±6.61 | 79.65±5.26 |
| Meditation | 76.25±10.71 | 77.55±7.88 | 83.70±4.41*; †††; ‡‡‡ | |
| Domain 4 | Control | 77.25±7.83 | 79.95±6.16 | 80.75±5.33 |
| Meditation | 77.00±8.23 | 79.90±5.48 | 84.45±4.02*; †††; ‡‡‡ |
Values are mean±SD. Significantly different (*P<0.05) compared to control group, Significantly different (†P<0.05, ††P<0.01, †††P<0.001) compared to baseline within group. Significantly different (‡‡‡P<0.001) compared to T1 within group. QOL: Quality of life, WHOQOL: World Health Organization Quality of Life
MOCA questionnaire
Analysis of the MOCA data revealed that there was a significant main effect of time and interaction between time and group for total score (P < 0.001) as well as for cognitive domains of executive function and attention (P < 0.01). For visuospatial abilities and delayed recall, significant main effect of time (P < 0.001 and <0.05, respectively) was seen. However, there was no significant main effect of time or group for language or orientation (P > 0.05) [Table 2].
There was a significant difference between the mean visuospatial, attention (P < 0.05 for both), executive function (P < 0.01) and total MOCA (P < 0.001) scores of the participants in the two study groups at the T2 time point.
Within the same group, participants in the meditation group showed a significant increase in their mean total MOCA scores at T1 (<0.05) as well as at T2 (P < 0.001) in comparison to their baseline scores. There was also a significant difference between their mean total scores at T1 and T2 (P < 0.001) time points. Participants in the meditation group also showed a significant increase in their visuospatial and attention (P < 0.01) as well as executive function and delayed recall (P < 0.05) scores at T2 in comparison to their baseline and T1 scores. In the control group participants, no significant difference (P > 0.05) was seen in any mean scores at any time points [Table 4].
| Parameter | Group | Baseline | T1 | T2 |
|---|---|---|---|---|
| Visuospatial | Control | 3.28±0.75 | 3.28±0.75 | 3.39±0.78 |
| Meditation | 3.40±0.68 | 3.45±0.69 | 3.85±0.37*;††; ‡‡ | |
| Executive function | Control | 3.67±0.49 | 3.67±0.49 | 3.67±0.49 |
| Meditation | 3.70±0.57 | 3.75±0.44 | 4.00±0.00**;†; ‡ | |
| Attention | Control | 5.55±0.60 | 5.55±0.60 | 5.45±0.69 |
| Meditation | 5.40±0.68 | 5.45±0.68 | 5.85±0.37*;††; ‡‡ | |
| Language | Control | 4.60±0.50 | 4.70±0.47 | 4.75±0.42 |
| Meditation | 4.75±0.44 | 4.80±0.41 | 4.80±0.41 | |
| Delayed recall | Control | 4.20±0.83 | 4.20±0.76 | 4.15±0.74 |
| Meditation | 4.25±0.96 | 4.50±0.68 | 4.55±0.82†; ‡ | |
| Orientation | Control | 6.0±0.0 | 6.0±0.0 | 5.95±0.22 |
| Meditation | 6.0±0.0 | 6.0±0.0 | 6.0±0.0 | |
| Total score | Control | 27.50±1.50 | 27.55±1.28 | 27.70±1.38 |
| Meditation | 27.50±1.47 | 27.90±1.33† | 29.05±0.99***;†††; ‡‡ |
Values are Mean±SD. Significantly different (*P<0.05; **P<0.01; ***P<0.001) compared to control group. Significantly different (†P<0.05; †††P<0.001) compared to baseline within group. Significantly different (‡P<0.05; ‡‡P<0.01) compared to T1 within group. MOCA: Montreal cognitive assessment questionnaire, SD: Standard deviation
DISCUSSION
The key findings of the present study include a significant decrease in the severity of IA along with significant improvements in the cognitive performance and QOL of young adult internet addicts following 8 weeks of RYM, thereby indicating its usefulness as an effective interventional strategy in counteracting the adverse effects of IA.
Following 8 weeks of RYM intervention, 60% of the participants achieved normal levels of internet usage, whereas the remaining exhibited either mild or moderate levels of IA, as illustrated by the YIAT scores. The unidirectional significant decreases seen in mean YIAT scores following both 1 and 8 weeks of RYM are in concurrence with earlier works that have shown similar decreases in PIU following different interventional modalities and protocols.[17] Surprisingly, a significant reduction in YIAT scores was also observed in control group participants at both 1 and 8 weeks of the study in comparison to their baseline readings. The recruitment and baseline assessments of the participants in the present study were done during the COVID-19 pandemic in April– June 2021. This period was marked by heightened stress and anxiety, both of which also play a crucial role in the causation of compulsive addictive behaviours, including IA.[4,5] Lifting of lockdown restrictions and resumption of offline classes/activities could have led to decreased scores of YIAT in controls. The same explanation may arguably be applied to the RYM group as well. However, significantly greater decrements were observed in mean YIAT scores in the RYM group as compared to the controls at both T1 and T2 time points. In addition, the significant interaction effect between time and group seen in the present study further highlights that the changes in IA scores over time differed between the meditation and control groups. This indicates that meditation group participants in the present study did experience additional benefits from the RYM practice itself that are not present in the control group. The additional beneficial effects of RYM on IA could be explained by the notion that when participants cultivate greater mindfulness and self-control, they tend to engage with the internet more purposefully, moving away from their compulsive internet use patterns.[17] This positive shift, in turn, enabled RYM group participants to cope more judiciously with their uncontrollable cravings and psycho-pathological dependence to engage in excessive online activities, resulting in lesser YIAT scores as compared to the controls.[27]
Paralleling the YIAT changes, significant improvement in the overall QOL of participants practising RYM within the duration of the intervention was also observed. Here, it is noteworthy that significant improvements in overall general health and physical and psychological health domains were evident even after 1 week of RYM. Our results conform with various other previous studies wherein improvements in mental health, QOL and subjective satisfaction with life were reported in behavioural addiction disorders, including IA, following meditation intervention.[17,18] In addition to within-subject changes, significant inter-group differences in the WHOQOL-Bref domains following 8 weeks of intervention were also seen in the current study.
Recently, some researchers have reported higher grey matter volume in the right superior frontal gyrus, left inferior orbitofrontal cortex, right insula and bilateral precuneus in RYM practitioners as compared to nonmeditators.[28] Notably, these brain regions are associated with positive thought processes, self-awareness and behaviour. People who spend much time online tend to have lower perceived QOL due to poor physical health, sleep deprivation, impaired work capacity, lack of concentration and reduced intimacy with family members.[12,13] RYM, as a form of behavioural intervention, empowers the minds of the practitioners by encouraging the positive flow of thoughts, enhancing self-esteem and imparting greater satisfaction and happiness to them.[23] Such favourable alterations induced by regular 8 weeks of RYM practice manifested as significant overall improvements seen across various domains of WHOQOL-Bref in these participants.
Our MOCA data illustrated the beneficial effect of RYM on visuospatial abilities, executive function, attention and delayed recall mechanisms. These observations in our study corroborate with earlier works examining the influence of meditation on cognitive status employing different populations and different experimental paradigms.[19-22] For instance, in a study conducted on adolescents aged 12– 18 years, significantly better performance on digit span and trail-making tests A and B were seen in the experimental group following 10 days of mindfulness meditation compared to the control group indicating improvements in working memory, shifting attention and executive functioning in them.[20] In another study conducted in young adults, a brief mindfulness exercise of 20 min showed a higher response accuracy and a smaller P3 amplitude at the post-test relative to the pre-test across Flanker conditions, whereas no such changes were observed in the control group, indicating more efficient cognitive processing in interventional group.[19] In addition, findings of a recent meta-analysis which synthesised data across diverse populations put forth mixed evidence of mindfulness meditation on different cognitive domains; namely, they reported significant improvements in executive function but non-significant effects on attention, working memory and long-term memory. The researchers attributed heterogeneity in attention and executive function used across different studies for their observed results.[21]
Preliminary neuroimaging studies have suggested that meditation induces structural and functional alterations in certain brain regions that play a major role in a variety of cognitive processes. Specifically, alterations are produced in regions such as the prefrontal cortex, entorhinal cortex, striatum, limbic regions and anterior and posterior cingulate cortex.[29] Strikingly, these areas have been implicated in attentional control, emotional regulation, response inhibition, memory and self-monitoring of thoughts.[19,29] Recently, in a randomised control trial, the influence of either an 8-session meditation program that focused on attention and acceptance or an 8-time program for body relaxation was compared in young adults with IGD. Meditation intervention was found to be more effective in decreasing addiction severity and gaming cravings compared with body relaxation. Moreover, meditation was associated with decreased brain activation in the bilateral lentiform nuclei, insula and medial frontal gyrus, indicating that it is an effective treatment for IGD, probably exerting its effects by altering frontopallidal pathways.[22]
Here, it is worth mentioning that in our study, the cognitive performance of meditation group participants following 8 weeks of RYM was also significantly better than controls. It is plausible that regular practice of RYM for 8 weeks enabled the participants to focus and orient their attention to the present experience and induced neuroplastic changes in the above-mentioned cognitive centres of the brain. This, in turn, enhanced their ability to select perceptual task-relevant information and to inhibit stimuli that were not relevant to fulfilling the task goal. This led to an increase in alertness, broadened attentional vigilance, better cognitive flexibility and improved working memory of RYM group participants in our study. However, we could not ascertain any significant difference in the language and orientation of the participants either within or between subjects at any point in time. These observations were on expected lines as all the participants were comparable in terms of age and gender distribution, educational level as well as their ability to read English letters, words and numerals.
Taken together, these current findings provide new insights into the effects of RYM on IA severity, neurocognitive functions and QOL in young adult internet addicts. However, it would be imprudent to attempt any generalisation of the findings to other populations without further statistical validation. Nevertheless, the inclusion of a control group, coupled with repeated recordings at 3-time points, enabled us to directly compare the influence of RYM on different outcome variables as well as track both the initial alterations (1 week) and sustained effects (8 weeks) of RYM in them with reasonable temporal resolution.
Limitation and future direction
The main limitation of our study was that our sample size was moderately small and inflated our chances of revealing positive findings, even when a correction for multiple tests was used. Second, although we did collect data regarding the activities for which they used the internet, future studies may also include the time spent on each activity better for understanding IA. Third, the participants practised RYM at home; hence, there is a plausibility of non-compliance on their end. However, to minimise this and to ensure adherence to meditation, we held online sessions twice a week for 8 weeks. In the future, more studies with a larger sample and supervised meditation sessions should be undertaken to elucidate the specificity of such findings further. Future studies may include one more healthy control (non-IA) group to compare the results for a better understanding of the study and its association with IA.
CONCLUSION
Our results indicate that 8 weeks of a RYM-based program was impactful in improving the cognitive performance and overall QOL of young adult internet addicts. The findings further illustrated the beneficial effect of RYM in decreasing the severity of IA in these participants, thereby indicating that it is effective in ameliorating the negative effects of IA and can serve as a useful preventive and curative nonpharmacological interventional modality for promoting cognitive and psycho-social well-being in internet addicts.
Acknowledgment
The authors would like to express their sincere thanks to their participants. Without their participation and cooperation, this study would not have been possible.
Ethical approval
The research/study approved by the Institutional Review Board at Maulana Azad Medical College, number F.1/IEC/MAMC/(82/10/2020/No.158, dated 14th January 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Measuring digital development: Facts and Figures. 2023. Available from: https://www.itu.int/en/itu-d/statistics/reports/facts-figures-2023.pdf [Last accessed on 2024 May 05]
- [Google Scholar]
- Internet addiction: The emergence of a new clinical disorder. Cyber Psychol Behave. 1998;1:237-44.
- [CrossRef] [Google Scholar]
- A study on Internet addiction and its relation to psychopathology and self-esteem among college students. Indian Psychiatry J. 2018;27:61-6.
- [CrossRef] [PubMed] [Google Scholar]
- Problematic internet use among adults: A cross-cultural study in 15 countries. J Clin Med. 2023;12:1027.
- [CrossRef] [PubMed] [Google Scholar]
- Internet addiction test: Croatian preliminary study. BMC Psychiatr. 2019;19:388.
- [CrossRef] [PubMed] [Google Scholar]
- ICD-11 for mortality and morbidity statistics. 2024. Mental, Behavioral or Neurodevelopmental Disorders. Available from: https://icd.who.int/browse/2024-01/mms/en#1448597234 [Last accessed on 2024 May 05]
- [Google Scholar]
- Global prevalence of digital addiction in general population: A systematic review and meta-analysis. Clin Psychol Rev. 2022;92:102-28.
- [CrossRef] [PubMed] [Google Scholar]
- Orienting of attention: Then and now. Q J Exp Psychol (Hove). 2016;69:1864-75.
- [CrossRef] [PubMed] [Google Scholar]
- The impact of competitive FPS video games on human's decision-making skills. Procedia Comput Sci. 2023;216:539-46.
- [CrossRef] [Google Scholar]
- Cognitive deficits in problematic internet use: Meta-analysis of 40 studies. Br J Psychiatry. 2019;215:639-46.
- [CrossRef] [PubMed] [Google Scholar]
- Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: An interaction of person-affect-cognition-execution (I-PACE) model. Neurosci Biobehav Rev. 2016;71:252-66.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of social networking sites on the quality of life of college students: A cross-sectional study from a city in North India. Sci World J. 2020;2020:8576023.
- [CrossRef] [PubMed] [Google Scholar]
- Internet addiction effect on quality of life: A systematic review and meta-analysis. ScientificWorldJournal. 2021;2021:2556679.
- [CrossRef] [PubMed] [Google Scholar]
- The mediating role of Internet addiction in depression, social anxiety, and psychosocial well-being among adolescents in six Asian countries: A structural equation modelling approach. Public Health. 2015;129:1224-36.
- [CrossRef] [PubMed] [Google Scholar]
- Association of internet addiction and mental disorders in medical students: A systematic review. Prim Care Companion CNS Disord. 2023;25:22r03384.
- [CrossRef] [PubMed] [Google Scholar]
- Does the internet bring people closer together or further apart? The impact of internet usage on interpersonal communications. Behav Sci (Basel). 2022;12:425.
- [CrossRef] [PubMed] [Google Scholar]
- Internet addiction management: A comprehensive review of clinical interventions and modalities. Cureus. 2024;16:e55466.
- [CrossRef] [Google Scholar]
- Effectiveness of mindfulness-based stress reduction on mental health and psychological quality of life among university students: A GRADE-assessed systematic review. Evid Based Complement Alternat Med. 2024;20:e8872685.
- [CrossRef] [PubMed] [Google Scholar]
- Neurophysiological evidence of the transient beneficial effects of a brief mindfulness exercise on cognitive processing in young adults: An ERP study. Mindfulness. 2023;14:1102-12.
- [CrossRef] [Google Scholar]
- Cognitive benefits of mindfulness meditation among adolescents. Int J Humanit Soc Sci Invent. 2021;10:1-5.
- [Google Scholar]
- Does mindfulness-based intervention improve cognitive function?: A meta-analysis of controlled studies. Clin Psychol Rev. 2021;84:101972.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy and neural mechanisms of mindfulness meditation among adults with internet gaming disorder: A randomized clinical trial. JAMA Netw Open. 2024;7:e2416684.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of Rajayoga meditation on positive thinking: An index for self-satisfaction and happiness in life. J Clin Diagn Res. 2013;7:2265-7.
- [Google Scholar]
- The neuroscience of mindfulness meditation. Nat Rev Neurosci. 2015;16:213-25.
- [CrossRef] [PubMed] [Google Scholar]
- Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998;28:551-8.
- [CrossRef] [PubMed] [Google Scholar]
- The Montreal cognitive assessment, MOCA: A brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695-9.
- [CrossRef] [PubMed] [Google Scholar]
- Mindfulness programs for problematic usage of the internet: A systematic review and meta-analysis. J Behav Addict. 2024;13:327-53.
- [CrossRef] [PubMed] [Google Scholar]
- Rajyoga meditation experience induces enhanced positive thoughts and alters gray matter Volume of brain regions: A cross-sectional study. Mindfulness. 2021;12:1659-71.
- [CrossRef] [Google Scholar]
- Mindfulness, attentional networks, and executive functioning: A review of interventions and long-term meditation practice. J Cogn Enhanc. 2022;6:1-18.
- [CrossRef] [Google Scholar]




