
Translate this page into:
Pharmacodynamic interaction profile of apigenin with diclofenac in an experimental model of inflammation in rats

*Corresponding author: Heenu Dhar, Department of Pharmacology, Faculty of Medicine & Health Sciences, SGT University, Gurugram, Haryana, India. heenu_fmhs@sgtuniversity.org
-
Received: ,
Accepted: ,
How to cite this article: Mondal A, Dikshit H, Kumar M, Mishra H, Mohan L, Dhar H. Pharmacodynamic interaction profile of apigenin with diclofenac in an experimental model of inflammation in rats. Indian J Physiol Pharmacol. doi: 10.25259/IJPP_404_2024
Abstract
Objectives:
Chronic use of non-steroidal anti-inflammatory drugs(NSAID’s) is often limited by their side effect, necessitating the development of safer therapeutic alternatives. Apigenin, A plant flavonoid, has shown potential in enhancing the efficacy of NSAIDs while potentially reducing their adverse effects. This study aimed to evaluate the synergistic effects of apigenin combined with a subtherapeutic dose of diclofenac on inflammation in a rat model, to determine whether such a combination can improve anti-inflammatory effectiveness and reduce the drug dose required.
Materials and Methods:
A total of 42 Wistar albino rats were randomised into seven groups to receive various treatments including control (normal saline), standard diclofenac (100 mg/kg), three doses of apigenin (10, 20 and 40 mg/kg), a subtherapeutic dose of diclofenac (50 mg/kg) and a combination of apigenin (20 mg/kg) with diclofenac (50 mg/kg). Inflammation was induced using carrageenan, and paw volume was measured at multiple time points to assess oedema. The percentage change from baseline paw volume and percentage protection against paw oedema was calculated for each group.
Results:
The study found that the combination of 20 mg/kg apigenin with 50 mg/kg diclofenac significantly enhanced the anti-inflammatory response, achieving a peak reduction in paw volume of up to 49.66% at 3 h post-administration. This was superior to the responses seen with apigenin or diclofenac alone, where the maximal dose of apigenin (40 mg/kg) only managed a peak reduction of 28.18%, and the standard dose of diclofenac (100 mg/kg) reached a peak inhibition of 66.66% at 6 h. The subtherapeutic dose of diclofenac (50 mg/kg), used alone, showed a lower peak effect of 21.47% at 3 h. These results underscore the enhanced efficacy of the combination therapy, potentially allowing for lower doses of diclofenac while maintaining effective anti-inflammatory action.
Conclusion:
The findings suggest that combining apigenin with diclofenac enhances anti-inflammatory responses, supporting the potential of flavonoid-NSAID combinations as more effective and safer anti-inflammatory therapies. Future studies should explore the long-term effects and mechanisms of action to fully understand the benefits and limitations of such combinations in managing chronic inflammation.
Keywords
Pharmacodynamics
Rat model
Synergistic effects
Anti-inflammatory
Diclofenac
Apigenin

INTRODUCTION
Inflammation is a fundamental biological process that occurs in response to injury or infection, characterised by symptoms such as redness, heat, swelling, pain and loss of function. While it is primarily a protective mechanism aimed at removing harmful stimuli and initiating the healing process, chronic inflammation can contribute to the progression of various diseases.[1] This dual nature makes inflammation a significant focus in medical research, especially concerning its role in chronic conditions. Chronic inflammation is implicated in a wide range of diseases that have substantial impacts on public health. These include but are not limited to, cardiovascular diseases such as atherosclerosis, metabolic disorders such as type 2 diabetes, neurodegenerative diseases such as Alzheimer’s and autoimmune conditions including rheumatoid arthritis and inflammatory bowel disease.[2] The persistent nature of inflammation in these conditions often leads to tissue damage and can significantly deteriorate the quality of life, thus representing a major burden on health systems worldwide.
The importance of managing inflammation effectively is underscored by its association with such a broad spectrum of health issues. Effective control of inflammation is thus not only crucial for managing specific inflammatory diseases but also for preventing the progression of other chronic diseases where inflammation is a contributing factor. Nonsteroidal anti-inflammatory drugs (NSAIDs) are amongst the most commonly prescribed medications worldwide for the management of pain and inflammation. They function primarily by inhibiting the cyclooxygenase (COX) enzymes, which are crucial in the production of pro-inflammatory prostaglandins. Common examples of NSAIDs include ibuprofen, aspirin and naproxen, which are widely used for a variety of acute and chronic inflammatory conditions.[3] Despite their efficacy, the chronic use of NSAIDs is associated with a range of adverse effects. Gastrointestinal complications are the most common, with symptoms ranging from mild dyspepsia to severe conditions such as gastric ulcers and bleeding. In addition, long-term NSAID use has been linked to increased risks of cardiovascular events and renal impairment, particularly in elderly populations or those with existing health complications.[4] These side effects significantly limit the long-term use of NSAIDs, especially at higher doses required for effective inflammation management. Given the limitations associated with NSAIDs, there is growing interest in the therapeutic potential of natural compounds, particularly those derived from plants. Flavonoids, a diverse group of phytonutrients found in fruits, vegetables and herbs, have garnered attention for their anti-inflammatory, antioxidant and anti-carcinogenic properties. Apigenin, a specific type of flavonoid present in chamomile, parsley and celery, has shown promising anti-inflammatory activity in several preclinical studies. In preceding research studies, apigenin decreased skin inflammation by downregulating the expression of COX-2.[5] The exploration of such natural compounds could lead to safer and more effective therapeutic strategies for managing inflammation. The exploration of natural compounds, particularly flavonoids, offers a promising avenue in the management of inflammation. Flavonoids are a diverse group of plant-based compounds known for their anti-inflammatory, antioxidant and anti-carcinogenic properties. These compounds are prevalent in a wide variety of fruits, vegetables and other plant-based foods and supplements.[6] Their mechanisms of action include inhibition of enzymes involved in the synthesis of inflammatory mediators, scavenging of free radicals and modulation of cell signalling pathways. Amongst the flavonoids, apigenin – found in abundance in chamomile, parsley and celery – has gained significant attention due to its potent anti-inflammatory properties. Research has shown that apigenin can inhibit the production of NF-κB signalling pathway which plays a critical role in the inflammatory process.[7] In addition, apigenin has been noted to suppress the expression of various inflammatory cytokines, such as tumor necrosis factor-alpha and interleukins, which are pivotal in the development and persistence of inflammatory responses.[8] The potential benefits of using plant-derived substances such as apigenin in inflammation management extend beyond their direct anti-inflammatory effects. Unlike traditional NSAIDs, flavonoids such as apigenin are associated with a lower risk of gastrointestinal toxicity and do not significantly affect platelet function, thus potentially offering a safer alternative for the long-term management of chronic inflammatory conditions.[9] Furthermore, the ability of apigenin to modulate multiple pathways involved in inflammation suggests that it could be effective in treating complex, multi-faceted diseases where conventional therapies have limited efficacy.[10]
The integration of flavonoids into therapeutic regimens for inflammation could revolutionise treatment paradigms, emphasising the need for further clinical studies to fully establish the efficacy and safety profiles of these compounds. The promising data on apigenin and other flavonoids underscore the potential of botanical compounds in enhancing health and combating disease, particularly in areas where conventional medications fall short. The interest in combining apigenin with NSAIDs stems from the increasing evidence suggesting that certain plant-derived compounds can enhance the efficacy and reduce the adverse effects of conventional pharmaceuticals. Preliminary studies have indicated that apigenin, a bioactive flavonoid, exhibits properties that can synergistically interact with NSAIDs to potentiate their anti-inflammatory effects while possibly mitigating associated gastrointestinal and cardiovascular risks.
Apigenin has been shown to modulate several key pathways involved in inflammation. It inhibits the activity of COX enzymes, much like NSAIDs, but without the gastrointestinal toxicity typically associated with these drugs. In addition, apigenin affects other significant inflammatory mediators such as nitric oxide synthase, and various cytokines, providing a broad spectrum of anti-inflammatory actions.[11] These properties suggest that when apigenin is combined with NSAIDs such as diclofenac, it may lead to enhanced inhibition of the inflammatory cascade at multiple points, potentially increasing the overall anti-inflammatory response while using lower doses of the NSAID. Despite growing interest in the potential synergistic effects of combining natural compounds such as apigenin with NSAIDs, there remains a significant gap in comprehensive studies that systematically investigate these interactions. The current literature primarily focuses on the individual anti-inflammatory properties of NSAIDs or flavonoids separately. There is a dearth of detailed research that specifically explores the combined effects of these compounds on inflammation, particularly under varied and controlled experimental conditions. Most existing studies have been either preliminary or limited in scope, often not extending beyond acute inflammation models or short-term observations. Given these gaps, there is a clear need for more detailed and systematic research. Studies should aim to explore these interactions across a variety of inflammation models, including both acute and chronic scenarios, to better understand the dynamics and implications of combining apigenin with NSAIDs.
MATERIALS AND METHODS
The study was conducted using a randomised controlled trial design to evaluate the pharmacodynamic interactions between apigenin and diclofenac in a carrageenan-induced inflammation model in Wistar albino rats. A total of 42 rats were divided into seven groups of six animals each, receiving varied treatments based on the experimental requirements.
The groups included a control group that received 2 mL of normal saline orally; a standard group treated with 100 mg/kg of diclofenac; three apigenin-treated groups receiving 20 mg/kg (most effective dose), 10 mg/kg (subtherapeutic dose) and 40 mg/kg (maximal dose), respectively; a subtherapeutic group receiving 50 mg/kg of diclofenac; and a combination group treated with 20 mg/kg of apigenin and 50 mg/kg of diclofenac. To induce inflammation, each rat received a sub-plantar injection of 1% carrageenan in the right hind paw. The volume of the paw was measured using a digital plethysmometer before and after carrageenan administration at predetermined time points: baseline, 0 h, 1 h, 2 h, 3 h, 4 h, 5 h and 6 h. These measurements helped assess the progression and mitigation of oedema under different treatment regimens. Data were systematically recorded, and the percentage changes from baseline paw volume were calculated to quantify the anti-inflammatory effects of each treatment. In addition, percentage protection against paw oedema was computed for comparative efficacy analysis of the different doses and combinations of apigenin and diclofenac. The results were presented succinctly in tables and heat maps. This method of presentation was chosen to avoid redundancy, ensuring that data were not duplicated across tabular and graphic forms, thus maintaining clarity and focus on the efficacy of the treatment regimens.
RESULTS
In the evaluation of pharmacodynamic interactions of apigenin with diclofenac in an experimental model of inflammation, varying responses were observed across different doses and combinations [Table 1].
| Group description+dose | Basal (mL) | 0 h (mL) | 1 h (mL) | 2 h (mL) | 3 h (mL) | 4 h (mL) | 5 h (mL) | 6 h (mL) |
|---|---|---|---|---|---|---|---|---|
| Control (normal saline), 2 mL orally | 0.56±0.10 | 0.80±0.25 | 1.12±0.04 | 1.24±0.32 | 1.49±0.12 | 1.12±0.07 | 1.09±0.01 | 0.90±0.11 |
| Standard (diclofenac), 100 mg/kg orally | 0.53±0.07 | 0.96±0.06 | 0.80±0.08 | 0.73±0.07 | 0.66±0.09 | 0.58±0.07 | 0.43±0.07 | 0.30±0.08 |
| Most effective dose (apigenin), 20 mg/kg orally | 0.55±0.08 | 0.93±0.11 | 0.87±0.08 | 0.813±0.11 | 0.78±0.10 | 0.74±0.10 | 0.71±0.11 | 0.60±0.07 |
| Subtherapeutic dose (apigenin), 10 mg/kg orally | 0.55±0.12 | 1.22±0.36 | 1.14±0.04 | 1.05±0.06 | 1.02±0.19 | 1.01±0.04 | 1.02±0.08 | 0.78±0.23 |
| Maximal dose (apigenin), 40 mg/kg orally | 0.53±0.15 | 1.11±0.07 | 1.03±0.18 | 0.89±0.06 | 1.07±0.09 | 0.97±0.07 | 1.00±0.02 | 0.59±0.20 |
| Subtherapeutic dose (diclofenac), 50 mg/kg orally | 0.52±0.07 | 0.90±0.13 | 1.06±0.11 | 1.12±0.08 | 1.17±0.08 | 1.09±0.06 | 1.01±0.05 | 0.74±0.08 |
| Combination dose (apigenin 20 mg/kg+diclofenac 50 mg/kg), orally | 0.53±0.11 | 0.912±0.05 | 0.86±0.06 | 0.80±0.03 | 0.75±0.03 | 0.68±0.05 | 0.60±0.07 | 0.56±0.08 |
The control group (normal saline, 2 mL orally) showed a progressive increase in paw volume over time, reaching a peak at 3 h post-carrageenan administration. The standard dose of diclofenac (100 mg/kg orally) effectively reduced paw oedema across all time points, achieving a significant reduction by the 6th h. The most effective anti-inflammatory response was observed with a 20 mg/kg oral dose of apigenin, which notably decreased paw volume, peaking at a 3-h interval. Lower doses of apigenin (10 mg/kg orally) and higher doses (40 mg/kg orally) were less effective than the 20 mg/kg dose but showed better outcomes than the control. Notably, a subtherapeutic dose of diclofenac (50 mg/kg orally) alone was less effective compared to its combination with apigenin 20 mg/kg, which significantly improved its efficacy. Percentage Protection against Paw Oedema for Various Treatment Regimens across different time points.
The heatmap [Figure 1] effectively illustrates the percentage protection against paw oedema for various treatment regimens across different time points.

- Percentage protection against paw oedema for various treatment groups across different time points.
Notably, the control group (normal saline, 2 mL orally) served as the baseline, with no protection values provided. The standard dose of diclofenac (100 mg/kg orally) showed a progressive increase in anti-inflammatory efficacy, starting from 5.35% at baseline and reaching up to 66.66% by the 6-h mark, demonstrating a consistent and effective reduction in inflammation. The most effective dose of apigenin (20 mg/kg orally) exhibited significant protection, particularly notable at the 3-h point with a 47.65% reduction in paw oedema. The subtherapeutic dose of apigenin (10 mg/kg orally) displayed a peak protection of 52.5% at 0 h, but showed less consistent results at other times, indicating limited efficacy at this lower dose. The maximal dose of apigenin (40 mg/kg orally) also provided moderate protection, peaking at 38.7% at 0 h, but then showed a general stabilisation of around 28% at later hours. The subtherapeutic dose of standard diclofenac (50 mg/kg orally) revealed lower effectiveness compared to its standard dose, with a maximum protection of 21.47% at 3 h. The combination dose of apigenin 20 mg/kg and diclofenac 50 mg/kg orally highlighted a synergistic effect, achieving enhanced anti-inflammatory activity with a peak protection of 49.66% at 3 h. This suggests that combining apigenin with diclofenac at subtherapeutic levels might allow for dose reduction while maintaining a desirable therapeutic impact. Percentage changes from baseline in paw volume for various treatment groups at different time points. The heatmap effectively illustrates the percentage changes from baseline in paw volume for various treatment groups at different time points after treatment administration.
The control group [Figure 2] administered normal saline, showed significant fluctuations, peaking at +166.07% at 3 h, before gradually declining to +60.71% by the 6-h mark. The standard dose of diclofenac (100 mg/kg orally) exhibited an initial sharp increase to +81.13% at 0 h, followed by a decreasing trend, ultimately dipping below the baseline to −43.40% at 6 h, reflecting a strong anti-inflammatory effect. The most effective dose of apigenin (20 mg/kg orally) displayed a more moderate and consistent efficacy, peaking at +58.18% at 1 h and slowly decreasing to +9.09% by 6 h. Conversely, the subtherapeutic dose of apigenin (10 mg/kg orally) resulted in the highest initial increase of +121.82% at 0 h, maintaining high levels until 5 h and then decreasing to +41.82% at 6 h. The maximal dose of apigenin (40 mg/kg orally) also showed a robust initial response of +109.43% at 0 h, experienced fluctuations and reached another peak of +101.89% at 3 h, before ending at +11.32% by the 6-h mark. The subtherapeutic dose of standard diclofenac (50 mg/kg orally) indicated a steady increase to a maximum of +125.00% at 3 h, followed by a reduction to +42.31% by the end of the period, suggesting substantial inflammation control. Finally, the combination dose of apigenin 20 mg/kg and diclofenac 50 mg/kg showed a moderated yet effective response, beginning at +72.08% at 0 h and gradually reducing to +5.66% by 6 h, denoting effective sustained control over inflammation.
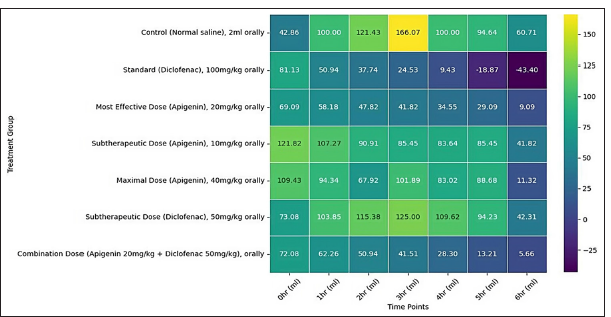
- Percentage changes in paw volume from baseline over time amongst various treatment groups.
DISCUSSION
The current study revealed significant insights into the pharmacodynamic interactions between apigenin and diclofenac, particularly in the context of inflammation management. The study findings demonstrated that the combination of apigenin at 20 mg/kg with diclofenac at 50 mg/kg produced a notably enhanced anti-inflammatory effect in a rat model of inflammation. This combination led to a peak reduction in paw volume of 49.66% at 3 h post-administration, an effect that was superior to what was observed when either compound was administered alone. For comparison, apigenin alone at its most effective dose (20 mg/kg) and diclofenac alone at a standard dose (100 mg/kg) resulted in lower peak reductions under similar conditions. The enhanced efficacy of the combination therapy indicates a synergistic interaction between apigenin and diclofenac, suggesting that apigenin may potentiate the anti-inflammatory effects of diclofenac. This synergy could allow for the use of lower doses of diclofenac when used in conjunction with apigenin, potentially reducing the adverse effects commonly associated with higher doses of NSAIDs. These findings are particularly relevant given the ongoing concerns regarding the safety profiles of long-term NSAID therapy, which include gastrointestinal, renal and cardiovascular risks. The findings from the study are in line with existing research on the anti-inflammatory properties of NSAIDs and flavonoids, particularly apigenin, but they also extend the knowledge by demonstrating the benefits of their combination. NSAIDs are well documented for their efficacy in reducing inflammation through the inhibition of COX enzymes, but their associated risks, especially when used long-term at high doses,[12] have prompted researchers to explore safer alternatives or adjunctive therapies. In this context, flavonoids such as apigenin have been increasingly studied for their potential to mitigate these risks while synergistically enhancing anti-inflammatory effects. Apigenin, specifically, has been shown in numerous studies to possess potent anti-inflammatory, antioxidant and anticancer properties. It acts on various biochemical pathways beyond those affected by NSAIDs, such as the inhibition of protein kinases, modulation of cytokine production and suppression of oxidative stress, which contributes to its therapeutic potential.[13] Our findings confirm these properties and suggest that when apigenin is combined with diclofenac, the therapeutic efficacy is not only maintained but enhanced, potentially allowing for lower doses of diclofenac to be used effectively. Significantly, the study contributes to the body of knowledge by providing experimental evidence of the synergistic effects between apigenin and diclofenac, which has been less explored. Previous studies have hinted at the potential of natural compounds to enhance the effects of NSAIDs, but empirical data demonstrating this effect, particularly in vivo, have been sparse. The enhanced reduction in inflammation observed with their combination in this study supports the hypothesis that natural compounds can effectively complement NSAIDs, leading to improved treatment outcomes. Moreover, this research also highlights the importance of dosage and timing in achieving the optimal therapeutic effect, aspects that have not been extensively explored in previous studies focusing on either apigenin or NSAIDs alone. By systematically exploring these parameters, this study offers new insights into the practical application of combining these compounds for inflammation management. While the findings of this study are promising, several limitations must be acknowledged. Primarily, the use of an acute model of inflammation limits the ability to directly extrapolate the results to chronic inflammatory conditions that involve complex, long-term immune responses. In addition, the study’s reliance on animal models raises concerns about the generalisability of the results to humans, as differences in metabolism, immune response and physiology can affect the effectiveness and safety of the treatments. To address these limitations and advance the understanding of apigenin and NSAID interactions, future research should focus on several key areas. Long-term studies incorporating chronic inflammation models could provide deeper insights into the sustained effects and potential side effects of these combinations. Clinical trials are crucial to determine the efficacy and safety of apigenin and diclofenac in human populations and to establish appropriate dosing regimens. Furthermore, investigating other natural compounds with anti-inflammatory properties could broaden the scope of potential therapeutic combinations and optimise NSAID usage.
CONCLUSION
This study significantly contributes to the field of inflammation management by demonstrating the enhanced anti-inflammatory effects of combining apigenin with diclofenac. The potential of this combination therapy to improve treatment outcomes and reduce NSAID-related side effects offers a promising avenue for developing safer, more effective therapeutic strategies. These findings lay the groundwork for future research and clinical applications that could transform the management of inflammatory diseases.
Additional information
Disclosures
Human subjects: All authors have confirmed that this study did not involve human participants or tissue.
Ethical approval
The study was approved by the Institutional Review Board at Indira Gandhi Institute of Medical Sciences, number 1919/GO/Re/S/16/CPCSEA, dated December 14, 2018 and by Institutional Animal Ethics Committee (IAEC), IGIMS PATNA Issued protocol number 1919/GO/Re/S/16/CPCSEA for animal subjects.
Declaration of patient consent
Patient’s consent is not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship:
Nil.
References
- Inflammation and atherosclerosis. Circulation. 2002;105:1135-43.
- [CrossRef] [PubMed] [Google Scholar]
- The mechanism of action of anti-inflammatory drugs. Int J Tissue React. 1998;20:3-15.
- [CrossRef] [PubMed] [Google Scholar]
- Non-steroidal anti-inflammatory drugs: Clinical implications, renal impairment risks, and AKI. Adv Ther. 2023;40:2082-96.
- [CrossRef] [PubMed] [Google Scholar]
- Apigenin: A therapeutic agent for treatment of skin inflammatory diseases and cancer. Int J Mol Sci. 2023;24:1498.
- [CrossRef] [PubMed] [Google Scholar]
- Flavonoids as potential anti-inflammatory molecules: A review. Molecules. 2022;27:2901.
- [CrossRef] [PubMed] [Google Scholar]
- Anti-inflammatory effects of apigenin in lipopolysaccharide-induced inflammatory in acute lung injury by suppressing COX-2 and NF-kB pathway. Inflammation. 2014;37:2085-90.
- [CrossRef] [PubMed] [Google Scholar]
- Apigenin blocks lipopolysaccharide induced lethality in vivo and the expression of proinflammatory cytokines by inactivating NF-? B through the suppression of p65 phosphorylation. J Immunol. 2007;179:7121-7.
- [CrossRef] [PubMed] [Google Scholar]
- The therapeutic potential of apigenin. Int J Mol Sci. 2019;20:1305.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of anti-granulation effect of apigenin-a plant flavonoid in wister albino rat. Int J Pharm Sci Rev Res. 2022;73:184-8.
- [CrossRef] [Google Scholar]
- Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and hip osteoarthritis: Network meta-analysis. BMJ. 2021;375:2321.
- [CrossRef] [PubMed] [Google Scholar]
- Plant-derived anti-inflammatory compounds: Hopes and disappointments regarding the translation of preclinical knowledge into clinical progress. Mediators Inflamm. 2014;2014:146832.
- [CrossRef] [PubMed] [Google Scholar]




