
Translate this page into:
Liposomal amphotericin-B-induced atrial fibrillation with hypomagnesaemia in acute invasive mucormycosis of the right maxillary sinus
*Corresponding author: Deeptipriya Nekkanti, Department of Pharmacy Practice, Bapuji Pharmacy College, Davangere, Karnataka, India. nekkantideepti@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nekkanti D, Yogeesha BS, Manasa R, Darshan M. Liposomal Amphotericin-B-induced atrial fibrillation with hypomagnesaemia in acute invasive mucormycosis of the right maxillary sinus. Indian J Physiol Pharmacol. doi: 10.25259/IJPP_222_2024
Abstract
Liposomal amphotericin B (LAmB) is the preferred drug for treating mucormycosis, a dangerous opportunistic infection caused by fungal pathogens. This case report details the medical history and treatment of a female patient who had type 2 diabetes, pulmonary artery hypertension and congenital heart disease. She was diagnosed with acute invasive mucormycosis in her right maxillary sinuses and underwent right endoscopic debridement. Throughout her treatment, she received 50 mg of injection LAmB. However, her magnesium levels decreased, and on the 10th day of treatment, she developed abnormal heart rhythms, specifically atrial flutter. This condition was successfully managed with an injection of digoxin (0.25 mg). Thus, continuous monitoring of magnesium and potassium levels, as well as electrocardiogram monitoring, is crucial in these cases. Failure to correct low potassium and magnesium levels in patients with congenital heart disease may result in heart rhythm disturbances or artery spasms. In our case, they treated it with syrup potassium chloride, and an injection of magnesium was given as a stat doses. Careful management and close monitoring are required to treat some cardiac-related effects of drugs and to achieve optimal outcomes in complex cases of mucormycosis treated with LAmB in our case continuous monitoring helped us with the achievement of treatment.
Keywords
Liposomal amphotericin B
Mucormycosis
Hypomagnesaemia
Atrial fibrillation
Congenital heart disease

INTRODUCTION
In the 1950s, amphotericin B (AmB) emerged as a vital polyene antifungal agent. However, its original formulation AmB deoxycholate faced considerable drawbacks, primarily dosing limitations and significant toxicity concerns, notably nephrotoxicity and infusion-related problems. Hence, a new drug formulation named liposomal AmB (LAmB) was introduced which has been used for the past 20 years; the oral administration of LAmB is poor so the intravenous route was preferred.[1,2] AmB acts by interacting with ergosterol present in the fungal cell membrane, initiating pore formation, ion leakage and eventual fungal cell death. IV administration of AmB can lead to hypokalaemia, hypomagnesaemia and hyperchloraemic acidosis due to increased permeability of the distal tubular membrane. Consequently, many patients necessitate substantial potassium and/or magnesium supplementation during therapy to mitigate these electrolyte imbalances.[3]
LAmB infusion in a patient with a cardiovascular history will have a risk of cardiotoxicity, cardiac arrest, myocardial infarction, arrhythmia, heart failure and cardiomyopathy with electrolyte abnormalities (hypokalaemia and hypomagnesia). To avoid these, proper timings should be maintained between the dosing (cumulative doses).[4-6]
Mucormycosis is a rare aggressive invasive fungal infection that affects immunocompromised and diabetic patients and causes thrombosis of vessels with consequent black necrosis of nasal and sinus tissues.[7]
Pathophysiology
The pathophysiology of mucormycosis entails the inhalation of spores through the nose, mouth or even through a skin laceration. In individuals with compromised cellular and humoral defence mechanisms, the response generated may be insufficient. This allows the fungus to potentially spread to the paranasal sinuses, orbits, meninges and brain through direct extension. Nonetheless, there are cases where patients with mucormycosis exhibit no discernible risk factors.[8]
Treatment
Surgical intervention alongside systemic antifungal therapy is the recommended approach for mucormycosis, with resection or debridement as needed. High-dose LAmB is strongly advised as the primary treatment, while isavuconazole and posaconazole through intravenous or delayed-release tablets are recommended alternatives with moderate strength. In addition, both triazoles are highly recommended as salvage treatments.[9]
Aim
In this case, treatment with LAmB was initiated which resulted in atrial fibrillation in acute invasive mucormycosis due to electrolyte abnormalities and successfully achieved complete therapy with LAmB by electrolyte monitoring and electrocardiogram (ECG) monitoring.
CASE REPORT
A 65-year-old female patient came up with complaints of pain in the right cheek with right side nasal block and right frontal headache with a history of type 2 diabetes mellitus, pulmonary artery hypertension and congenital heart disease; there was no family history of type 2 diabetes mellitus and hypertension. On examination, pathology history depicts acute invasive mucormycosis of the right maxillary sinus and a surgical procedure was done for right side endoscopic debridement 20 days back and further referred for management with LAmB. LAmB management was commenced immediately upon the patient’s admission, aligning with their past medical and medication history and corresponding to their current complaints. Before initiating the initial dose of LAmB, cross consultation was done with a cardiologist and was sought that her 2D echo was congenital heart disease, situs solitus, levocardia, severe pulmonary artery hypertension and good biventricular function. The regimen began with a daily dose of 50 mg of LAmB, subsequently adjusted to a maintenance dose of 100 mg per day. There were no cardiac-related complaints before the drug administration and electrolytes (magnesium, potassium, sodium and chloride) were monitored before and after LAmB from day 1 to day 23 alternatively, sodium and chloride levels were normal, [Table 1] given with the magnesium and potassium levels.
| Days (1-23) | Serum magnesium levels | Potassium levels |
|---|---|---|
| Day-1 | 1.8 mg/dL | 4.35 mmoL/L |
| (Before LAmB) | ||
| Day-2 | 1.63 mg/dL | 4.22 mmoL/L |
| Day-4 | 1.41 mg/dL | 4.57 mmoL/L |
| Day-6 | 1.38 mg/dL | 3.99 mmoL/L |
| Day-8 | 1.39 mg/dL | 4.2 mmoL/L |
| Day-10 | 1.3 mg/dL | 3.72 mmoL/L |
| Day-12 | 1.35 mg/dL | 3.68 mmoL/L |
| Day-14 | 1.41 mg/dL | 4.1 mmoL/L |
| Day-16 | 1.11 mg/dL | 3.7 mmoL/L |
| Day-18 | 0.8 mg/dL | 3.5 mmoL/L |
| Day-19 | 1.3 mg/dL | 3.6 mmoL/L |
| Day-21 | 1.4 mg/dL | 3.9 mmoL/L |
| Day-22 | 1.42 mg/dL | 3.4 mmoL/L |
| Day-23 | 1.43 mg/dL | 3.5 mmoL/L |
LAmB: Liposomal amphotericin B
On the 10th day, after reaching a cumulative dose of 900 mg, the patient experienced abnormal heart rhythms, as indicated by arterial flutter observed on the ECG in [Figure 1] due to continuous intravenous administration of LAmB which shows the cardiac effect of the drug due to disturbances in electrolytes. This condition was effectively managed with a 3-day course of injection digoxin (0.25 mg) after that stat injection of magnesium sulphate (2 g) in 100 mL normal saline was given. Following this episode, rechallenging was undertaken on the 12th day with a dose escalation to 1000 mg, resulting in a notable reduction in the patient’s complaints.
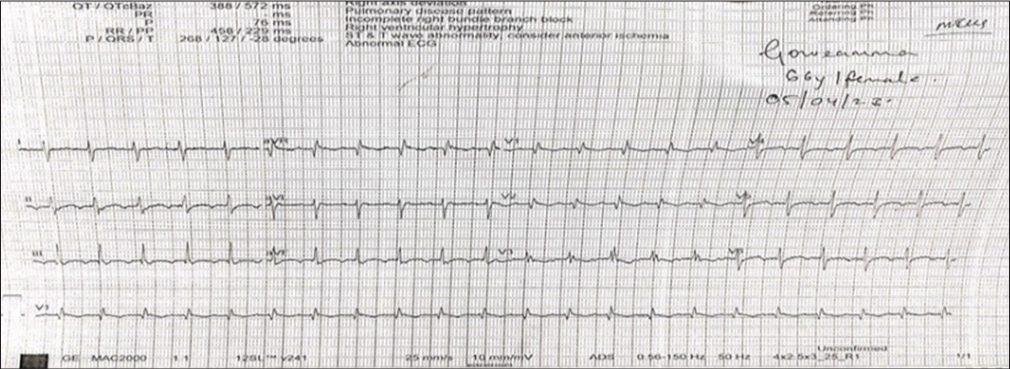
- 10th day electrocardiogram showing atrial flutter with 2:1 AV conduction. AV: Atrioventricular.
On the 18th day, the cumulative dosage that was administered was 1600 mg, the magnesium levels of the patient were decreased to 0.8 mg and the potassium level was 3.5 mmoL/L which can be seen in Table 1 and ECG shows sinus tachycardia in Figure 2; again, the LAmB treatment was on hold for a day because LAmB treatment cannot be stopped. Since mucormycosis is a life-threatening infection, the cumulative dosage of 1700 mg was again started on the 21st day.
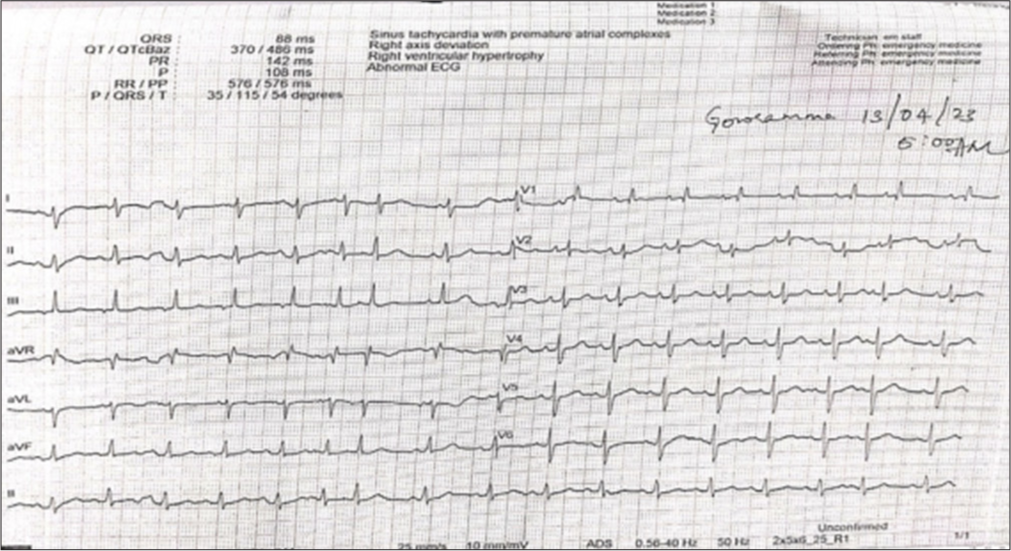
- On 18th day electrocardiogram showing sinus tachycardia with premature atrial complexes.
On the 22nd day, the patient developed chief complaints of (c/o) chills and atrial fibrillation, which occurred during the infusion of 1800 mg LAmB later shifted to an emergency, and LAmB was stopped. Injection amiodarone (100 mg) was given to treat the atrial fibrillation and syrup potassium chloride (15 mL) once daily was given to resolve hypokalaemia along with an injection of magnesium sulphate for hypomagnesaemia. After the patient’s complaints were resolved and stabilised, the patient was discharged against medical advice on day 23 with the instruction to continue taking LAmB at the dose of 1900 mg and to report right away in case of emergency.
In this case, after treatment with atrial fibrillation, the patient’s condition was stable, and continuous monitoring of electrolytes and ECG helped us in dosage adjustments of LAmB. Successful LAmB treatment was achieved, and the patient was treated with mucormycosis with other comorbid conditions.
DISCUSSION
In the study by Chen et al., low magnesium levels that cause various arrhythmias, including torsade de pointes, atrial fibrillation and ventricular tachycardia, were investigated.[10] In our case, on the 18th day of AmB administration, a significant reduction in magnesium levels to 0.8 mg/dL resulted in sinus tachycardia with premature atrial complexes. Magnesium is vital for cardiac electrical stability, and its deficiency can lead to arrhythmias by increasing intracellular calcium and prolonging the QT interval.
In the study by Gremillion, Craven, rapid infusion of AmB resulted in a progressive increase in patient potassium levels, and ECGs conducted over 3 days consistently indicated hyperkalaemia, ultimately leading to ventricular fibrillation.[11] In this case, potassium levels slightly decreased to 3.4 mmoL/L, which was vice-versa; the study by Liu et al. supports the notion that hypokalaemia could lead to cardiovascular deaths associated with atrial fibrillation in older adults, with an incidence rate of 30.98%.[12] In our case, there was a slight decrease in potassium levels, which may have led to the onset of atrial fibrillation due to LAmB administration. This suggests that even minor electrolyte imbalances can result in cardiac issues in patients with past cardiac history. Although evidence linking LAmB to atrial fibrillation is limited, this case demonstrates that electrolyte alterations can provoke heart-related issues in patients with a history of cardiac problems.
In the study, of Autry et al., LAmB-associated cardiac arrest in a patient with pre-existing cardiac-related disease states has been studied, which supports this case that LAmB will cause cardiac-related issues in patients with past heart issues.[7] These observations underscore the varied cardiac effects associated with different antifungal agents and highlight the critical importance of continuous monitoring for electrolyte imbalances and cardiac complications during antifungal therapy in patients with cardiac comorbidities.
The treatment plan included surgical debridement and LAmB to obtain maximum therapeutic success. The treatment approach considered the existing comorbidities and relied on supportive care for the stability of the patient. Challenges, including adverse drug reactions and patient condition fluctuation, were managed effectively. By applying the Naranjo scale in Table 2, scoring was given that the causality assessment of cardiac-related ADRs was probable (Score 6); Hartwig’s severity assessment scale was given in Table 3; this indicates Level 4 and in the World Health Organization causality categories, it is classified as Certain, as a laboratory abnormality showed alterations in magnesium and potassium levels. Finally, the re-challenging and de-challenging of LAmB were satisfactory. This incident emphasises the therapy adjustment, to reduce the risk of adverse effect.
| Naranjo adverse drug reaction probability scale | Score | |||
|---|---|---|---|---|
| Question | Yes | No | Do not know | |
| 1. Are there previous conclusive reports on this reaction? | +1 | 0 | 0 | 1 |
| 2. Did the adverse event appear after the suspected drug was administered? | +2 | -1 | 0 | 2 |
| 3. Did the adverse reaction improve when the drug was discontinued or a specific antagonist was administered? | +1 | 0 | 0 | 1 |
| 4. Did the adverse event reappear when the drug was re-administered? | +2 | -1 | 0 | 2 |
| 5. Are there alternative causes (other than the drug) that could on their own have caused the reaction? | -1 | +2 | 0 | 0 |
| 6. Did the reaction reappear when a placebo was given? | -1 | +1 | 0 | 0 |
| 7. Was the drug detected in blood (or other fluids) in concentrations known to be toxic? | +1 | 0 | 0 | 0 |
| 8. Was the reaction more severe when the dose was increased or less severe when the dose was decreased? | +1 | 0 | 0 | 0 |
| 9. Did the patient have a similar reaction to the same or similar drugs in any previous exposure? | +1 | 0 | 0 | 0 |
| 10. Was the adverse event confirmed by any objective evidence? | +1 | 0 | 0 | 0 |
| Total score | 06 | |||
| Level | Severity | Hartwig’s severity assessment scale |
|---|---|---|
| Level-4 | Moderate | The ADR required that treatment with the suspected drug be held, discontinued or otherwise changed. AND/OR an antidote or other treatment was required and an increase in LOS at least for 1 day |
ADR: Adverse drug reaction, LOS: Level of severity
CONCLUSION
This case report highlights the occurrence of atrial fibrillation as ADR of LAmB in patients with comorbid conditions such as congenital heart diseases, pulmonary artery hypertension and diabetes mellitus and causes challenges in achieving successful treatment. Since LAmB treatment is associated with foreseen ADRs, preventing complications such as arrhythmia by monitoring serum electrolytes, magnesium and ECG frequently helps in preventing cardiac-related complications in patients with cardiac comorbidities. The patient’s condition improved with appropriate management, highlighting the importance of individualised treatment strategies and vigilant follow-up care in optimising outcomes in such complex cases of mucormycosis.
Acknowledgement
We would like to express our sincere gratitude to Dr. Yogeesha B.S professor and HOD of the ENT department of SS Institute of Medical Sciences and Research Centre and our principal, HOD (Head of the department) and all the professors of the department of pharmacy practice of Bapuji Pharmacy College, who helped us in writing this case report.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Pharmacology of amphotericin B In: Smith J, ed. Advances in Antifungal Therapy (2nd Edition). New york: Springer; 2023. p. :1-24.
- [Google Scholar]
- Acute amphotericin B overdose. Ann Pharmacother. 2006;40:2254-9.
- [CrossRef] [PubMed] [Google Scholar]
- Liposomal amphotericin B (AmBisome®): A review of the pharmacokinetics, pharmacodynamics, clinical experience and future directions. Drugs. 2016;76:485-500.
- [CrossRef] [PubMed] [Google Scholar]
- Acute refractory hyperkalaemia and fatal cardiac arrest related to administration of liposomal amphotericin B. Neth J Med. 2008;66:433-7.
- [Google Scholar]
- Fluconazole-induced recurrent ventricular fibrillation leading to multiple cardiac arrests. Anaesth Intensive Care. 2009;37:477-80.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic management of rhinocerebral mucormycosis with topical and intravenous amphotericin B. J Laryngol Otol. 2011;125:807-10.
- [CrossRef] [PubMed] [Google Scholar]
- Liposomal amphotericin B-Associated cardiac arrest. Infect Dis Clin Pract. 2008;26:327-30.
- [CrossRef] [Google Scholar]
- Mucormycosis in a diabetic patient: A case report with an insight into its pathophysiology. Contemp Clin Dent. 2017;8:662-6.
- [CrossRef] [PubMed] [Google Scholar]
- Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019;19:e405-21.
- [Google Scholar]
- Circulating electrolytes and the prevalence of atrial fibrillation and supraventricular ectopy: The Atherosclerosis risk in communities (ARIC) study. Nutr Metab Cardiovasc Dis. 2020;30:1121-9.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factor of ventricular fibrillation during rapid amphotericin B infusion. Antimicrob Agent Chemother. 1985;27:868-71.
- [CrossRef] [PubMed] [Google Scholar]
- Prognosis of older adult patients suffering from atrial fibrillation and hypokalemia. Clin Interv Aging. 2023;18:1363-71.
- [CrossRef] [PubMed] [Google Scholar]




