
Translate this page into:
A comparative analysis of the drug interaction programmes amongst geriatric outpatients
*Corresponding author: Panita Limpawattana, Department of Internal Medicine, Faculty of Medicine, Khon Kaen University, Friendship Highway road, Muang, Khon Kaen, 40002, Thailand. lpanit@kku.ac.th
-
Received: ,
Accepted: ,
How to cite this article: Wannawichate T, Limpawattana P. A comparative analysis of the drug interaction programmes amongst geriatric outpatients. Indian J Physiol Pharmacol. 2025;69:49-54. doi: 10.25259/IJPP_590_2023
Abstract
Objectives:
Drug interaction programmes are considered imperative tools utilised by healthcare professionals to screen potential risks that may occur from drug combinations. However, the outcomes of analysing drug–drug interactions (DDIs) differ across each programme. It is crucial for clinician to be aware of the varying results from each database and their limitations before utilising them. This study aimed to compare drug interaction programmes in geriatric patients at an outpatient clinic of a tertiary care hospital.
Materials and Methods:
A retrospective study was performed at a tertiary care hospital in Thailand. This study collected all prescriptions for patients from the outpatient clinic during November 2021 and 2022. The drug interaction programs using Micromedex, Medscape and Lexicomp were used to detect and assess the severity of DDIs.
Results:
The participants were recruited using electronic medical records in the enrolment of a total of 10,877 individuals. The majority of these patients were male, with an average age of 74.3 (standard deviation 6.8) years. The prevalence of major DDIs using Lexicomp, Micromedex and Medscape was 28.1%, 57.9% and 18.2%, respectively. Only 1700 major DDIs (15.6%) were observed to be consistent across all three programmes. The strength of agreement amongst these drug interaction programmes using Kappa statistics was 0.15, 0.35 and 0.61 (P <0.01) in major, moderate and minor + no interaction groups, respectively.
Conclusion:
The degree of agreement of major DDIs among the three-drug programmes, Lexicomp, Micromedex and Medscape, was minimal. To maintain uniformity in drug information sources, it is essential to apply measures for the standardisation of DDIs documentation.
Keywords
Drug–drug interactions
Drug interaction programme
Elderly
Outpatient

INTRODUCTION
Geriatric populations exhibit a greater propensity for experiencing adverse drug reactions (ADRs) in comparison to other age groups, and diagnosing these adverse effects in older adults is challenging. The unusual symptoms that manifest further compound this complexity, ascertaining whether they are attributable to the ageing process or the medications employed for therapeutic purposes.[1] The prevalence of ADRs in this population fails to evince any significant deviation from the previous times. The average rate of hospital admissions due to ADRs amongst the geriatric populations was recorded at 16.6%, in contrast to a significantly lower rate of 4.1% observed in younger individuals.[2] The occurrence of drug-drug interactions (DDIs) is a major cause of ADRs. Older adults exhibit heightened vulnerability to the occurrence of DDIs due to several variables such as advanced age, multiple comorbidities and polypharmacotherapy.[3]
The prevalence of possible DDIs amongst older adults with multimorbidity in primary care settings ranges from 20% to 100%.[4] A systematic review has indicated that DDIs accounted for 0.57% of hospital admissions in the general population but for the geriatric cohort, this percentage increased to 4.8%.[5] However, it is crucial to prioritise the screening of DDIs, as they are preventable and manageable adverse events.[6]
Drug interaction programs are indispensable tools that healthcare professionals use to screen for potential risks that may arise from drug combinations. The vast amount of DDI information poses a challenge for clinicians to remember all of it. At present, there are several drug interaction programmes available in various forms, such as open access or subscription resources. Upon comparing the results of DDIs screening from different programmes, it has been observed that they may yield different outcomes.[7] Former research has demonstrated a comparatively low level of consensus on the classification of DDIs across different applications.[8,9] It is essential for the clinician to be aware of the varying results from each database and to consider their benefits and limitations when choosing to utilise them.[10] Numerous investigations have been conducted to compare various drug interaction software applications, such as Lexicomp, Micromedex, Medscape, Eporactes, DDInter and Drugs. com.[11-13] The software applications most commonly selected by clinicians in hospital settings are Lexicomp, Micromedex and Medscape. The majority of the studies found that Lexicomp received the highest scores. However, it was found that previous studies were conducted in oral oncolytic [12,14] organ transplants [7,13] and antiretroviral drug interactions.[15] However, a comparative analysis of all three programmes in the elderly population remains limited. Therefore, the aim of this study was to compare drug interaction programmes in the geriatric population at an outpatient clinic of a tertiary care hospital, with the objective of assisting physicians and pharmacists in selecting the most appropriate programme for screening purposes to ensure accuracy and safety in medication prescribing for older patients.
MATERIALS AND METHODS
Study setting and design
A retrospective study was undertaken at a tertiary care institution that functions as a University Hospital located in the Northeastern area of Thailand. The study collected all prescriptions for patients from the outpatient clinic from November 2021 to 2022. Patient data were carefully obtained from the healthcare facility’s information system, with the highest level of caution taken to guarantee the anonymity of patients and the confidentiality of the collected data. The study (reference number HE661074) received approval from the Institutional Review Board of the University, with a special exemption for individual consent in relation to this observational analysis.
Populations
Subjects for this study were selected based on the criteria of being 65 years or older and having been prescribed at least 2 medications. The electronic health records under scrutiny were exclusively sourced from the Special Medication Centre. The scope of this study did not include topical preparations, specifically inhalers, creams, ointments, patches and sprays.
Drug interaction programme
The data for the study were obtained by utilising electronic medical records. The identification of possible drug interactions and their respective levels of severity were determined using drug interaction programmes, including Lexicomp, Micromedex and Medscape. These three programmes have extensive usage by pharmacists in hospital settings. Both Lexicomp (by Wolters Kluwer Copyright 2023 UptoDate, Inc. version 7.7.7 [2023.06.29])[16] and Micromedex (by Merative, version 2930)[17] necessitate subscriptions for usage in the context of drug interaction analysis, whereas the Medscape programme (WebMD Network)[18] is freely accessible. The drug interaction software previously mentioned provides explanatory information and can be identified under various names. Lexicomp generates a category with a risk rating and severity [19] [Table 1].[20] For this analysis, the various categories were transformed into degrees of severity, as illustrated in Table 2.[13] We decided to provide a comprehensive account solely of the DDIs that were deemed clinically significant, specifically those with a moderate or major risk, as per the guidelines established in the literature.[21] In cases where a program designed for detecting drug interaction database identified one category for a particular drug pair, the most critical category was opted for.
| Risk rating | Severity | Action |
|---|---|---|
| A | No interactions found | Nothing |
| B | Minor | No action needed |
| C | Moderate | Monitor treatment |
| D | Major, moderate | Change regimen |
| X | Major | Avoid use together |
| Categorised by severity | Lexicomp | Micromedex | Medscape |
|---|---|---|---|
| Contraindication | Major | Contraindicated | Contraindicated |
| Major | Major | Serious-use alternative | |
| Moderate | Moderate | Moderate | Monitor closely |
| Minor | Minor | Minor | Minor |
| None | No interaction found | No results found | No interactions found |
Interrater percent agreement and reliability
Descriptive statistics were used to delineate the attributes of the studied population. The kappa statistic was employed to encapsulate the concordance among the three-drug interaction programmes. A kappa statistic is proportionate to a range of values from 0, indicating agreement attributable to chance, to 1.0, which indicates absolute agreement. To deduce the strength of the agreement, the Landis and Koch scale was utilised. A kappa value of <0.00 signifies inadequate agreement, 0.00–0.20 indicates minimal agreement, 0.21–0.40 denotes moderate agreement, 0.41–0.60 signifies intermediate agreement, 0.61–0.80 suggests considerable agreement, and 0.81–1.00 indicates nearly perfect agreement. Furthermore, the kappa’s P-values were computed and assessed for statistical significance, which was determined to be <0.05.[22]
RESULTS
Prevalence of DDIs using Lexicomp, Micromedex and Medscape
A cumulative cohort of 10,877 individuals was gathered for participation in this research through electronic medical records. The mean age of patients was 74.3 (standard deviation 6.8 years), characterised by a notable prevalence of male subjects (54.3%). Table 3 illustrates the overall prevalence of DDIs in the geriatric population, with a focus on moderate and major DDIs, as well as contraindications, as analysed by Lexicomp, Micromedex and Medscape. In this study, it was observed that drugs that were deemed contraindicated were not included in any of the three-drug interaction programmes. Our findings indicated that while the overall figures were similar, differences in severity were observed. Figure 1 further represents the overlap in the prevalence of major DDIs, as identified by the Micromedex, Medscape and Lexicomp Drug Interaction Programmes. There were only 1700 major DDIs (15.6%) that exhibited consistency across all three drug interaction programmes. The majority of major DDIs were found in Micromedex, followed by Lexicomp and Medscape. The prevalence of major DDIs in Micromedex was not correlated with other programmes, resulting in a total of 3202 DDIs or 29.4%. The major DDIs between Lexicomp versus Micromedex exhibited consistency, with 1156 DDIs or 10.6%. Similarly, Micromedex versus Medscape accounted for 243 DDIs or 2.2%, and Lexicomp versus Medscape was found to be 9 DDIs or 0.1%.
| Category | Lexicomp | Micromedex | Medscape |
|---|---|---|---|
| Minor+None, n (%) | 3858 (35.5) | 3495 (32.1) | 3355 (30.8) |
| Moderate, n (%) | 3960 (36.4) | 1081 (10.0) | 5543 (51.0) |
| Major, n (%) | 3059 (28.1) | 6301 (57.9) | 1979 (18.2) |
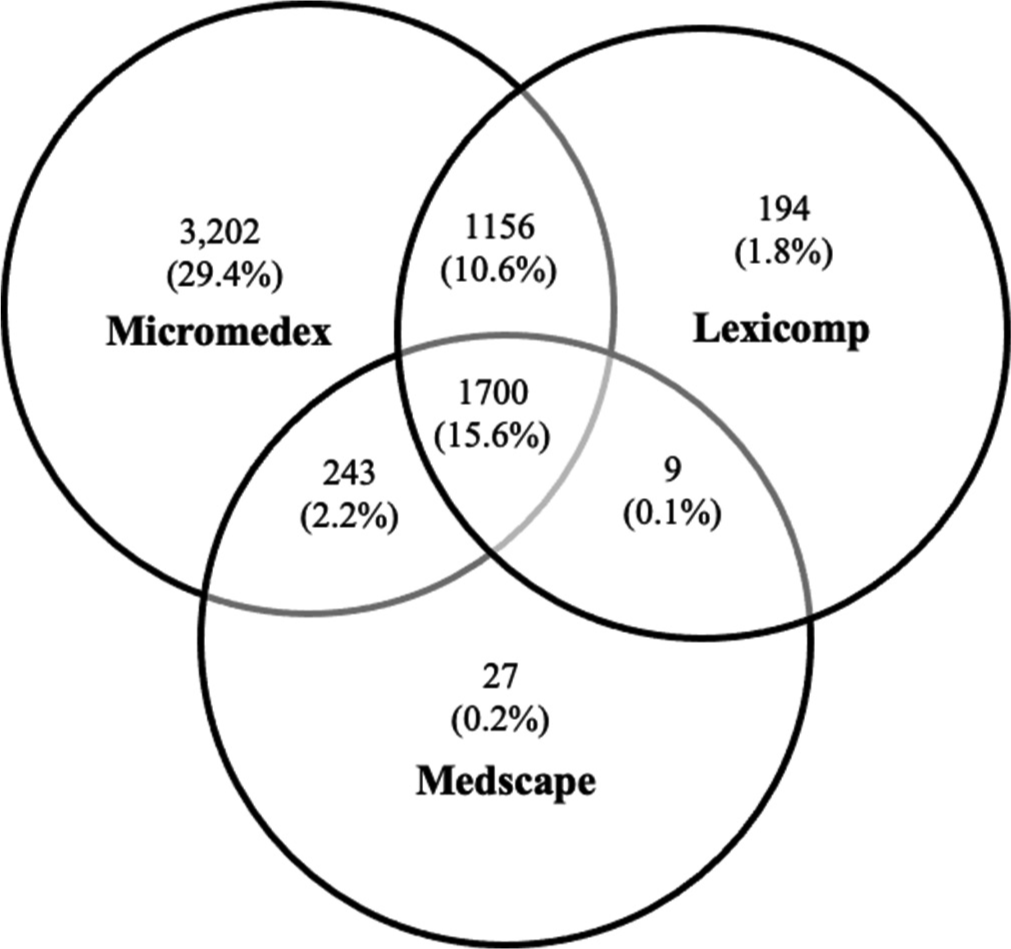
- Prevalence of major drug–drug interaction identified by the Micromedex, Medscape and Lexicomp Drug Interaction Programmes.
The three most encountered DDIs with major severity were omeprazole versus clopidogrel (6.3%), followed by central nervous system (CNS) depressants versus opioid analgesics (4.2%), and orphenadrine versus CNS depressant (3.2%). Various programmes detected different severity classifications. For example, orphenadrine versus CNS depressant was detected with major severity in Lexicomp but none in Micromedex and was classified as moderate in Medscape and prednisolone versus aspirin was detected with major severity in Micromedex but was deemed moderate in Lexicomp and Medscape [Table 4].
| Interacting pair | n (%) | Interaction effect | Severity | |||
|---|---|---|---|---|---|---|
| Lexicomp | Micromedex | Medscape | ||||
| Omeprazole | Clopidogrel | 682 (6.3) | Reduce serum concentrations of the active metabolite (s) of clopidogrel | Major | Major | Major |
| CNS depressant | Opioid analgesics | 460 (4.2) | Augment the CNS depressant effect of opioid agonist | Major | Major | Moderate |
| Orphenadrine | CNS depressant | 349 (3.2) | Augment the CNS depressant effect of orphenadrine | Major | None | Moderate |
| TCA | NSAIDs | 199 (1.8) | Result risk of bleeding | Moderate | Major | None |
| Methotrexate | NSAIDs | 198 (1.8) | Increase the serum concentration of methotrexate | Major | Major | Major |
| Prednisolone | Aspirin | 136 (1.25) | Salicylates may augment the adverse/ toxic effect of prednisolone. | Moderate | Major | Moderate |
| Omeprazole | Rifampicin | 126 (1.16) | CYP2C19 inducers may reduce the serum concentration of omeprazole | Major | Major | Major |
CNS: Central nervous system, TCA: Trans-cinnamaldehyde, NSAIDs: Non-steroidal anti-inflammatory drugs
Agreement amongst Lexicomp, Micromedex and Medscape in identifying major DDIs
The strength of agreement amongst the 3 drug interaction programmes using kappa statistic was statistically significance (P < 0.01) across all severity of DDIs, where it was slightly, fairly and substantially agreed in major, moderate and minor + none groups, respectively [Table 5].
| Severity | Kappa | P-value | Strength of agreement |
|---|---|---|---|
| Minor+None | 0.61 | <0.01 | substantial |
| Moderate | 0.35 | <0.01 | fair |
| Major | 0.15 | <0.01 | slight |
Drug pairs with contraindication were not found in this study
DISCUSSION
The prevalence of DDIs in older patients varies depending on the study setting, utilised programmes and selected population. This study involved analysing the medication record in older patients using three-drug interaction programmes at an outpatient facility of a tertiary care hospital. The prevalence of major DDIs in older patients using Lexicomp, Micromedex and Medscape in this study was 28.1%, 57.9% and 18.2%, respectively. Our findings were different from one report in China, and it showed that the prevalence of major DDIs in comparable settings based on three databases such as Lexicomp, Micromedex, and DDInter, was 32.2%, 32.9% and 22.6%, respectively.[4] A study in the nephrology outpatient setting of a University hospital in Hong Kong reported that the prevalence of major and severe DDIs using Lexicomp, Micromedex, and Medscape was 19.6%, 37.8% and 35.5%.[13] These findings indicated weak compatibility among the databases, as evidenced by the interrater agreement obtained from the programmes in our study, particularly with regard to major DDIs (which showed only slight agreement). The possible reasons for the disparity amongst drug interaction programmes such as Micromedex, Medscape and Lexicomp might be due to the variations in the number of potential DDIs detected, the severity of these interactions and the overall quality of information provided. These differences could be attributed to database algorithms, update frequency and the underlying sources of drug interaction data.[23-25] Nonetheless, our study demonstrated substantial agreement between the minor DDIs and the no-interaction group. It implies a high negative predictive value of the DDI report while a low sensitivity in detecting major DDIs. Therefore, it is essential for healthcare practitioners to possess a comprehensive understanding of the diverse potential DDIs identified by various drug interaction software programs.
Drug interaction programmes utilise scientific and contemporary literature to compile information into categories that are accessible to healthcare professionals. However, the results from this study revealed the discrepancies of major DDIs across the three databases, and in actual clinical practice, the individual patient has different background characteristics that might not have been covered in the previous studies. In addition, the diverse factors of each patient cannot be fully integrated into these programmes. Therefore, the use of more than one database in detecting DDIs, particularly for major DDIs, is suggested to ensure a thorough assessment and identification of potential drug interactions. Furthermore, the establishment of clinical protocols concerning the occurrence of clinically substantial DDIs and their probable unfavourable consequences, along with the provision of management approaches to aid clinicians in the prompt identification of potential DDIs, necessitates a thorough evaluation of relevant literature and consultations with proficient clinical pharmacists and experienced physicians. The successful execution of such initiatives can avert the oversight of these interactions and promote the appropriate administration of pharmacotherapy for geriatric patients.[4,26,27]
The frequent major DDIs of the three-drug interaction programmes in this research were omeprazole versus clopidogrel, followed by CNS depressants versus opioid analgesics and orphenadrine versus CNS depressant. These findings should alert physicians and clinical pharmacists, especially while prescribing these medications. Studies have been carried out in Thailand that have produced similar results.[28] Despite pharmacodynamic studies indicating that omeprazole possesses the ability to alleviate the antiplatelet effect of clopidogrel. Nevertheless, the evidence from observational studies does not demonstrate an increase in cardiovascular risk among patients undergoing treatment with this combination. [29,30] Patients treated with the combination of clopidogrel and omeprazole displayed a reduction in the likelihood of experiencing gastrointestinal events and a similar likelihood of experiencing cardiovascular events. However, the judgement to administer proton-pump inhibitors to patients receiving clopidogrel should be made on an individualised basis, taking into account the patient’s bleeding and cardiovascular risk factors.[31] In the United States, studies have indicated that the combination of CNS depressants and opioid analgesics, or the co-administration of two CNS depressants (including muscle relaxants), was the most commonly found DDI in the elderly population.[32] It is advisable to refrain from employing simultaneous administration of agents that depress the CNS unless there are no feasible alternative therapies. In the event that concomitant use is necessary, the healthcare professional should administer the minimal feasible amount and period of each medication, all the while guaranteeing that the intended therapeutic outcome is achieved.[33]
The utilisation of a dependable and extensively validated database derived from preceding research was a key strength of this investigation.[4,34] In addition, it was the first study to compare the prevalence of DDIs in a geriatric outpatient setting within a tertiary care hospital in Thailand. However, some limitations of this study were identified. First, because of its retrospective nature, the data acquired from electronic medical records may be deficient or may underrepresent certain aspects, particularly the data concerning the actual clinical complication of major DDI. In addition, data concerning the usage of over-the-counter medications or herbals were not gathered. Second, this study was performed within a single institution, which might limit the generalisability in other settings. Third, the database has undertaken multiple revises concerning potential DDIs. Therefore, if any changes have been enacted with respect to particular pharmaceuticals across each category, the outcomes of this study may likely differ from its prior versions.
CONCLUSION
The level of agreement amongst the major DDI programmes, namely Lexicomp, Micromedex and Medscape, was slight. To promote consistency in drug information references, it is imperative that standardisation measures are put in place for DDI documentation. It is essential for healthcare providers to acknowledge this variability and understand that these resources only contribute partially to the overall quality of prescribing. To facilitate the timely detection of potential DDIs, it is recommended that a clinical practice guideline should be developed to address clinically significant DDIs and provide management strategies for clinicians.
Ethical approval
The research/study was approved by the Institutional Review Board at Khon Kaen University, Thailand, number HE661074, dated 18th February 2023.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that they have used artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript.
Financial support and sponsorship: Nil.
References
- Approach to minimize adverse drug reactions in elderly In: Pharmacovigilance. Vol 2. London: IntechOpen; 2022. Available from: https://www.intechopen.com/chapters/83704 [Last accessed on 2023 Jul 29]
- [CrossRef] [Google Scholar]
- Hospitalisations caused by adverse drug reactions (ADR): A meta-analysis of observational studies. Pharm World Sci. 2002;24:46-54.
- [CrossRef] [PubMed] [Google Scholar]
- Pharmacological interactions in the elderly. Medicina (Kaunas). 2020;56:320.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and associated factors of drug-drug interactions in elderly outpatients in a tertiary care hospital: A cross-sectional study based on three databases. Ann Transl Med. 2023;11:17.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of drug interactions in hospitalised elderly patients: A systematic review. Eur J Hosp Pharm. 2021;28:4-9.
- [CrossRef] [PubMed] [Google Scholar]
- Important drug-drug interactions in the elderly. Drugs Aging. 1998;12:485-94.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of four drug-drug interaction databases for patients undergoing haematopoietic stem cell transplantation. J Clin Pharm Ther. 2022;47:1711-9.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of three commercial knowledge bases for detection of drug-drug interactions in clinical decision support. J Am Med Inform Assoc. 2017;24:806-12.
- [CrossRef] [PubMed] [Google Scholar]
- Real-life drug-drug and herb-drug interactions in outpatients taking oral anticancer drugs: Comparison with databases. J Cancer Res Clin Oncol. 2022;148:707-18.
- [CrossRef] [PubMed] [Google Scholar]
- Screening for severe drug-drug interactions in patients with multiple sclerosis: A comparison of three drug interaction databases. Front Pharmacol. 2022;13:946351.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of five common drug-drug interaction software programs regarding accuracy and comprehensiveness. J Res Pharm Pract. 2016;5:257-63.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of nine tools for screening drug-drug interactions of oral oncolytics. J Oncol Pract. 2018;14:e368-74.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of clinically relevant drug interactions by online programs in renal transplant recipients. J Manag Care Spec Pharm. 2020;26:1291-6.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of eight screening tools to detect interactions between herbal supplements and oncology agents. J Oncol Pharm Pract. 2020;26:1843-9.
- [CrossRef] [PubMed] [Google Scholar]
- Antiretroviral drug-drug interactions: A comparison of online drug interaction databases. J Clin Pharm Ther. 2022;47:1720-4.
- [CrossRef] [PubMed] [Google Scholar]
- Lexi-drugs. Lexicomp app. UpToDate Inc. Available from: https://play.google.com/store/apps/details?id=com.lexi.android&hl=en [Last accessed on 2023 Jul 15]
- [Google Scholar]
- Micromedex drug interaction. Micromedex drug interactions app. Available from: https://play.google.com/store/apps/detailsid=com.truven.druginteractionsnative.customer&hl=en [Last accessed on 2023 Jul 15]
- [Google Scholar]
- Drug interactions checker - Medscape drug reference database. Available from: https://reference.medscape.com/drug-interactionchecker [Last accessed on 2023 Jul 15]
- [Google Scholar]
- Possible drug-drug interactions of hydroxychloroquine with concomitant medications in prophylaxis and treatment of COVID-19: Multiple standard software based assessment. JCDR. 2020;14:FC16-23.
- [CrossRef] [Google Scholar]
- Lexi-Interact data fields. Available from: http://webstore.lexi.com/information/product-information/lexi-interact-fields [Last accessed on 2023 Jul 31]
- [Google Scholar]
- Drug-drug interactions in elderly patients with potentially inappropriate medications in primary care, nursing home and hospital settings: A systematic review and a preliminary study. Pharmaceutics. 2021;13:266.
- [CrossRef] [PubMed] [Google Scholar]
- Potential drug interactions with drugs used for bipolar disorder: A comparison of 6 drug interaction database programs. Pharmacopsychiatry. 2020;53:220-7.
- [CrossRef] [PubMed] [Google Scholar]
- Determination and comparison of potential drug-drug interactions using three different databases in northern Cyprus community pharmacies. Niger J Clin Pract. 2022;25:2005-9.
- [CrossRef] [PubMed] [Google Scholar]
- Drug-drug interactions in an intensive care unit and comparison of updates in two databases. Farm Hosp. 2022;46:290-5.
- [Google Scholar]
- Potential drug-drug interactions of antiretrovirals and antimicrobials detected by three databases. Sci Rep. 2021;11:6089.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of potential drug-drug interactions in outpatients of a general hospital in China: A retrospective investigation. Int J Clin Pharm. 2020;42:1190-6.
- [CrossRef] [PubMed] [Google Scholar]
- Potential drug-drug interactions among elderly patients admitted to medical ward of Ayder Referral Hospital, Northern Ethiopia: A cross sectional study. BMC Res Notes. 2016;9:431.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of drug interactions in elderly patients at ambulatory care in Chonburi Hospital. Chonburi Hosp J. 2022;47:129-38.
- [Google Scholar]
- Clopidogrel and interaction with proton pump inhibitors: Comparison between cohort and within person study designs. BMJ. 2012;345:e4388.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular outcomes and mortality in patients using clopidogrel with proton pump inhibitors after percutaneous coronary intervention or acute coronary syndrome. Circulation. 2009;120:2322-9.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical relevance of clopidogrel-proton pump inhibitors interaction. World J Gastrointest Pharmacol Ther. 2015;6:17-21.
- [CrossRef] [PubMed] [Google Scholar]
- Polypharmacy and severe potential drug-drug interactions among older adults with cardiovascular disease in the United States. BMC Geriatr. 2021;21:233.
- [CrossRef] [PubMed] [Google Scholar]
- American Geriatrics Society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67:674-94.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of three brands of drug interaction software for use in intensive care units. Pharm World Sci. 2010;32:822-8.
- [CrossRef] [PubMed] [Google Scholar]




