
Translate this page into:
A comparative mixed-method study of flipped classroom and traditional lecture for teaching rational drug prescription among undergraduates in pharmacology

*Corresponding author: Jitha S, Department of Pharmacology, Government Medical College, Thiruvananthapuram, Kerala, India. jitha.sus@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Jitha S, Thomas SP. A comparative mixed-method study of flipped classroom and traditional lecture for teaching rational drug prescription among undergraduates in pharmacology. Indian J Physiol Pharmacol. 2024;68:246-51. doi: 10.25259/IJPP_263_2023
Abstract
Objectives:
Rational drug prescription is a very important competency an Indian Medical Graduate (IMG) should acquire during his undergraduate training. Irrational prescriptions lead to drug resistance, adverse drug reactions (ADRs) and drug interactions. The study was aimed to determine the effectiveness of flipped classroom compared to lecture class in teaching rational drug prescription and to compare the perception of students about either methods.
Materials and Methods:
This was a prospective interventional mixed – method study where students were pseudo-randomised to either Traditional Lecture (TL) or Flipped Classroom (FC) based on the date of their academic session. For the study purpose, 250 phase 2 MBBS students in Pharmacology were divided into two groups. Allocation into 2 groups was done by lot method one week before the scheduled class so that the online study materials could be sent to the students belonging to the flipped classroom method in the form of case scenarios and videos.
Results:
A total of 198 students participated in the study with 103 in the TL group and 95 in the FC group. Acquisition of higher order cognitive skills like application and analysis was assessed by measuring an academic score obtained from a series of exercises on rational prescription for given clinical scenarios. The academic score of the TL group (5.99 ± 2.34) vs FC group (5.59 ± 1.39 ) thus obtained was not statistically significant p > 0.05, Effect size- 0.08.
Conclusion:
A questionnaire -based assessment of students’ perceptions of TL and FC showed a statistically significant difference in favour of FC in terms of their perceptions to improve academic scores, generate peer-interaction, facilitate team- work and improve teacher- student interaction.
Keywords
Flipped classroom
Pharmacology
Rational drug prescription
Medical undergraduates

INTRODUCTION
Rational drug prescription is a very important competency an Indian Medical Graduate which should acquire during his undergraduate training. It has a great impact on the health of the patients as well as the community as a whole. Irrational prescriptions lead to drug resistance, adverse drug reactions (ADRs) and drug interactions. Proper training in writing prescriptions and rational use of drugs helps in improving patient safety, lessens the litigations on doctors, reduces the incidence of ADRs and drug interactions as well as builds trust in the doctors.
Flipped classroom (FC) originated in the American Woodland Park High School in 2007. The flipped or inverted classroom is a blended learning approach that reverses traditional teaching.[1] When learning is flipped, didactic lectures are pre-recorded and made available for students to watch before class and class time is used for active learning strategies to deepen their understanding and knowledge.[2] The technological movement has enabled the amplification and duplication of information at an extremely low cost.[3]
The effective delivery of a traditional lecture (TL) class poses a major challenge for the faculty members, especially in the field of medical education, due to the involvement of vast knowledge and complicated concepts.[4] The FC has emerged as one of the most effective ways to impart curricular delivery during a large group teaching session.[5] The core elements of this learning include pre-class content, assessments, working on gaps and developing competency. The teacher’s role is like a guide. It makes the real implementation of transformation from teacher-centred to student-centred. It makes the students from passive recipients of knowledge to active searchers for knowledge.
Some researches show that the FC method has a positive impact as an active learning method on various attitudes and behaviours, such as student success, motivation, dependency, critical thinking, capability, creativity and problem-solving capability, whereas some others have inconclusive results related to academic scores.[6] Even though it is quite an effective approach to teaching-learning, the implementation of the same requires careful planning and support from the faculty members.[7] FC has also been found to be advantageous in the improvement of higher-order cognitive skills such as application, analysis, synthesis and evaluation.[8]
A literature search shows that very few studies gauge student perception on multiple parameters and measure the acquisition of higher-order cognitive skills with FC versus TL in pharmacology. The study aims to find the change in immediate outcomes, such as the improvement in prescription writing and perception by students in the new teaching-learning method.
Objectives
The objectives of this study were as follows:
To determine the effectiveness of FC compared to lecture class in teaching rational drug prescription
To compare the perception of students about either method.
MATERIALS AND METHODS
Study population
This was a prospective interventional mixed-method study where students were pseudo-randomised to either TL or FC based on the date of their academic session. The study was initiated after obtaining approval from the Institutional Human Ethics Committee (HEC No.01/17/2022/MCT dated 26 February 2022). Phase II MBBS students undergoing pharmacology training willing to give informed consent were included in the study.
The study was conducted in the Department of Pharmacology of a Government Medical College in South India.
Study design
Prescriptions of the common disease conditions in the general population as well as special groups such as children and pregnant ladies are usually taught by lecture method. For the study purpose, 250 phase two MBBS students in pharmacology were divided into two groups. Allocation into two groups was done by lot method 1 week before the scheduled class so that the online study materials could be sent to the students belonging to the FC method 1 week prior in the form of case scenarios and videos of 15 common disease conditions. The first group was taught rational drug prescriptions for these 15 disease conditions by the TL method, and the second group dealt with the FC method. During the FC session, student discussion was promoted to find the answers to the given clinical conditions. About 100 students who were present in the session were subdivided into 15 subgroups and each of the group was asked to take a lot of one disease from 15 disease conditions. Although they had to prepare all 15 disease conditions before the class using the study materials provided 1 week before the class, each subgroup discussed one particular disease condition. The discussion was highlighted in the areas of how to write a good prescription, what drugs to be given for each of the disease conditions, and the dose, route and duration of administration of drugs for that disease. Discussion on concomitantly administered drugs in certain conditions where multiple drugs have to be administered and the rationale of not co-administering some drugs so as to prevent drug interactions and, thereby, ADRs were also done. Directions for the use of drugs, as well as proper communication regarding non-pharmacological approaches and preventive strategies to be conveyed to patients, were also discussed. Students attending the lecture session were taught the same topic in the TL method on the very next day. At the end of each session, a short test in the form of an objective-structured practical examination (OSPE) was conducted to write prescriptions for the given two clinical conditions. The questions were from the discussed disease scenarios and the marks scored were assessed in both groups. The questions given to all the students in one arm were the same. The questions given to both groups were peer-reviewed and validated. Marks were assigned for the format of prescription writing, such as superscription, inscription, transcription, and subscription and for the prescribed drugs, their dose, duration and route of administration. Marks were also assigned for writing directions of use wherever needed and for writing communication matters in the answer. A feedback form in the form of a Likert questionnaire, which was framed with the help of experts and peer validated, was given to the students to assess how the students perceived each type of teaching method with respect to peer interaction, organisation of topic, level of teacher-student interaction, enhancing understanding of the topic, creating interest in the topic, improving communication skills, promoting teamwork and developing motivation to learn rational prescription. The questionnaire also enquired if a teaching–learning method was expected to enhance their academic score and also if they would recommend the method to their juniors. The confidentiality of the students was maintained throughout the study about their feedback as they did not have to write their names or roll numbers in the feedback form. The marks scored in the study were not used in the final assessment in internal or University examinations. Both sessions were conducted by the same facilitator on consequent days. To avoid ethical issues, the lecture class was delivered later for all students who had FC sessions.
Statistical analysis
The data collected using OSPE and feedback form were entered in a Microsoft Excel sheet, and analysis was done using the Statistical Package for the Social Sciences (SPSS) software (IBM SPSS Statistics Version 20). The academic scores, as well as student perception scores on a Likert scale, were analysed using the Mann–Whitney U-test. Statistical significance in different parameters between the two methods was analysed using mean and P-values. The perception of students obtained from feedback forms was also expressed as percentages.
RESULTS
A total of 198 students participated in the study, with 103 in the TL group and 95 in the FC group. Acquisition of higher-order cognitive skills such as application and analysis was assessed by measuring an academic score obtained from a series of exercises on rational prescription in a given clinical scenario. The academic score of the TL group (5.99 ± 2.34) vs FC group( 5.59 ± 1.39) thus obtained was not statistically significant p > 0.05, Effect size- 0.08.
A questionnaire assessed students’ perceptions of TL and FC. There was a statistically significant difference in favour of FC for the following perceptions: the ability to improve academic scores, generate peer interaction, facilitate teamwork, and improve teacher-student interaction [Table 1]. Table 2 explains the number of responses obtained for each Likert score for the ten parameters that were used for assessing perception of students to TL and FC. In Figure 1, stacked bar chart is used to compare the overall scores of different parameters. The ten perceptions which were assessed among students is graphically represented here.
| Perception | Lecture | Flipped | P-value | Effect size | ||
|---|---|---|---|---|---|---|
| Mean* | SD | Mean* | SD | |||
| Ability to improve academic score | 2.04 | 0.88 | 1.67 | 0.68 | 0.003 | 0.21 |
| Enhance communication skills | 1.90 | 0.82 | 1.66 | 0.67 | 0.054 | 0.14 |
| Create interest in topic | 1.74 | 0.83 | 1.50 | 0.58 | 0.064 | 0.13 |
| Increase motivation to learn | 1.83 | 0.79 | 1.66 | 0.69 | 0.176 | 0.09 |
| Better organisation of topic | 1.81 | 0.79 | 1.59 | 0.59 | 0.054 | 0.14 |
| Generate peer interaction | 1.89 | 0.85 | 1.55 | 0.62 | 0.005 | 0.2 |
| Promote teamwork | 1.89 | 0.89 | 1.55 | 0.62 | 0.01 | 0.18 |
| Recommend to juniors | 1.74 | 0.99 | 1.58 | 0.59 | 0.78 | 0.02 |
| Facilitate teacher–student interaction | 1.59 | 0.60 | 1.39 | 0.55 | 0.016 | 0.17 |
| Greater understanding of a topic | 1.55 | 0.67 | 1.49 | 0.52 | 0.45 | 0.05 |
TL: Traditional lecture, FC: Flipped classroom, SD: Standard deviation, *In the study, while using Likert scale Strongly Agree was given score 1. ‘*’ is used to highlight this effect.
| Perception | Method | Likert Scale – No of responses (%) | Total responses | ||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||
| Ability to improve academic score | TL | 28 (27.2) | 51 (49.5) | 18 (17.5) | 4 (3.9) | 2 (1.9) | 103 |
| FC | 41 (45.1) | 39 (42.9) | 11 (12.1) | 0 | 0 | 91 | |
| Enhance communication skills | TL | 35 (34) | 48 (46.6) | 15 (14.6) | 5 (4.9) | 0 | 103 |
| FC | 39 (43.3) | 43 (47.7) | 7 (7.7) | 1 (1.1) | 0 | 90 (1 no response) | |
| Create interest in topic | TL | 43 (41.7) | 51 (49.5) | 4 (3.9) | 3 (2.9) | 2 (1.9) | 103 |
| FC | 49 (53.8) | 38 (41.8) | 4 (4.4) | 0 | 0 | 91 | |
| Increase motivation to learn | TL | 37 (35.9) | 52 (50.5) | 10 (9.7) | 3 (2.9) | 1 (1) | 103 |
| FC | 42 (46.2) | 38 (41.8) | 11 (12.1) | 0 | 0 | 91 | |
| Better organisation of topic | TL | 38 (37.2) | 47 (46.1) | 14 (13.7) | 3 (2.9) | 0 | 102 (1 no response) |
| FC | 42 (46.2) | 44 (48.4) | 5 (5.5) | 0 | 0 | 91 | |
| Generate peer interaction | TL | 38 (36.9) | 43 (41.7) | 17 (16.5) | 5 (4.9) | 0 | 103 |
| FC | 47 (51.6) | 38 (41.8) | 6 (6.6) | 0 | 0 | 91 | |
| Promote teamwork | TL | 41 (39.8) | 38 (36.9) | 18 (17.5) | 6 (5.8) | 0 | 103 |
| FC | 47 (51.6) | 38 (41.8) | 6 (6.6) | 0 | 0 | 91 | |
| Recommend to juniors | TL | 53 (51.5) | 34 (33) | 10 (9.7) | 2 (1.9) | 4 (3.9) | 103 |
| FC | 43 (47.7) | 42 (46.6) | 5 (5.5) | 0 | 0 | 90 (1 no response) | |
| Facilitate teacher–student interaction | TL | 48 (46.6) | 49 (47.6) | 6 (5.8) | 0 | 0 | 103 |
| FC | 58 (63.7) | 30 (33) | 3 (3.3) | 0 | 0 | 91 | |
| Greater understanding of the topic | TL | 48 (47.5) | 49 (48.5) | 2 (1.9) | 2 (1.9) | 0 | 101 (2 no response) |
| FC | 47 (51.6) | 43 (47.3) | 1 (1.12) | 0 | 0 | 91 | |
TL: Traditional lecture, FC: Flipped classroom
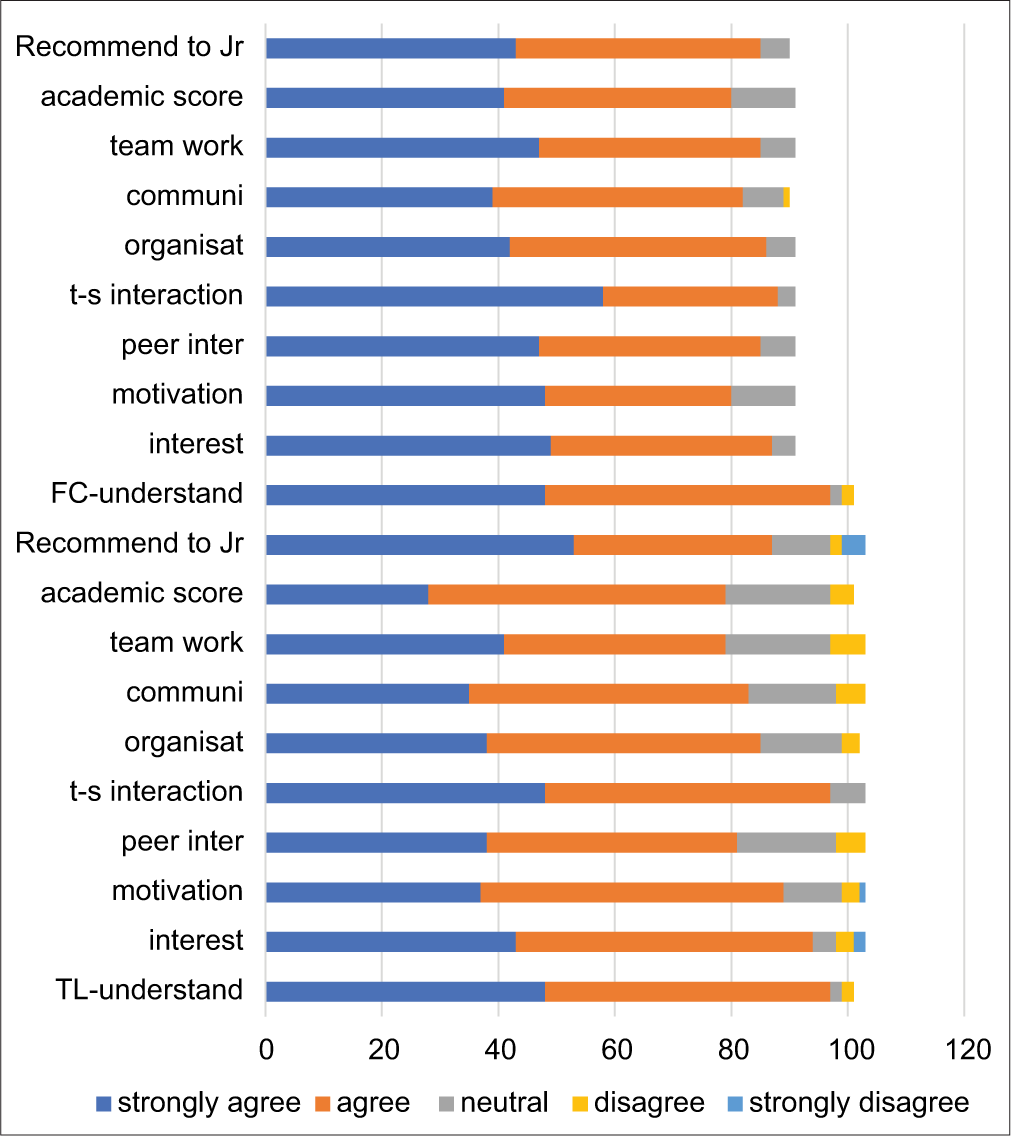
- Perception of traditional lecture and flipped classroom. TL: Traditional lecture, FC: Flipped classroom, t-s: Teacher student interaction.
*In the Likert scale used in the study, 1 = strongly agree and 5 = strongly disagree. Hence, the lower the value more favourable the perception. #Effect size is calculated by test statistic divided by the root of sample size (small effect: 0.1 <r ≤0.3, medium effect: 0.3 <r ≤0.5, and large effect: r > 0.5).
Overall, there was a perception that FC can enhance communication skills and provide a better organisation of the topic to be studied; however, the difference was not statistically significant (P = 0.054).
For all the perceptions, FC had a greater percentage of responses in category 1, that is, strongly agree, compared to TL, whereas the responses in category 2, that is, agree, were more for TL. This denotes that more students favour FC versus TL, though the difference was not much.
DISCUSSION
Medicine involves the complex integration of various subjects and its clinical applications aided by critical thinking. There is a need for self-learning and life-long learning to excel in this field. The FC method involves more interaction, facilitates critical thinking and is a learner-centric approach which is an integral part of adult learning. As a result, FC has gathered a lot of backing from medical and related fields. The present study examined the acquisition of higher-order cognitive skills assessed by prescription writing skills for clinical scenarios; as well as the perception of students toward TL and FC on ten parameters. The marks obtained after evaluating the prescription writing exercise were not significantly different between the TL and FC groups, though the perception that academic score will increase with FC was there. A systematic review by Ramnanan and Pound highlights the same aspect of FC, that is even though the student response toward FC is largely positive, there is no convincing evidence that FC enhances learning.[9] Another study which examined the FC approach to teaching evidence-based medicine did not improve scores compared to its traditional counterpart.[10] The reason for this result in our study may be due to the implementation of FC for just one session. Since the students had no previous experience of FC, they might have been a bit slow to adopt this new method. Another explanation why performance scores generally are not significantly different with FC compared to TL may be due to the testing methods followed which are not adequate in assessing the higher-order cognitive skills.[11]
In this study, there was a statistically significant difference in the perceptions of students in favour of FC with regard to the ability to improve the academic score, generate peer interaction, promote teamwork and facilitate teacher–student interaction, whereas such a significant difference was not seen in reference to the ability to enhance communication skills, create interest in a topic, increase motivation to learn, better organisation of topic or provide them with a greater understanding of the topic and thereby not recommending FC over TL to their juniors. FC is better than TL in acquiring Blooms’ higher-order skills such as analysis while for lower-order skills such as memorising and understanding FC is as good as TL.[12] Blair et al. looked at the knowledge gain as well as change in prescription pattern for type 2 diabetes mellitus among internal medicine postgraduates and found that FC was preferred by the trainees. They also reported an increase in knowledge as well as a change in prescribing pattern following FC.[13] Most studies on FC demonstrate greater student satisfaction which stems from the fact that students can learn at their own pace and at their own convenience. They also enjoy the small group discussions and problem-solving exercises during the face-to-face sessions.[14] It has been suggested that FC model when implemented properly improves both intrinsic and extrinsic learner motivation.[15] A quiz implemented at the beginning of the face-to-face session has been found to increase student motivation to go through the pre-class content and helps in gauging student learning. Tests can be conducted at various points of time such as at the start as well as end of face-to-face session, after a few weeks to even months after the session. While gauging student learning, these tests also increase student scores by test-enhanced learning. Another advantage is that the tests help to evaluate the effectiveness of the teaching method.[16] There is some objective evidence that FC enhances student interest and engagement as seen by the marked increase in attendance from 30% to 80% when lecture classes were flipped.[17] The learner-centric approach of FC has resulted in increased peer interaction and communication during the pre-class review of study materials as well as during the small group discussions and problem-solving sessions. The teacher acts as a facilitator during the face-to-face sessions providing support and a framework as the student’s progress toward their learning objectives. The FC method facilitates greater teacher–student interaction and peer interaction when compared to TL.[18]
Students of medical and allied fields are generally appreciative of the FC method, though they have their apprehensions.[9] There is a need for student to spend in the pre-class phase since there is the need to go through the topic-related content which is time intensive. The preparatory material may not be appropriately aligned to the content covered in the classroom sessions. Some faculty may be overly didactic in the face-to-face sessions which can negate the benefits of FC. Unless the faculty facilitates discussion by all students in each small group, some students may dominate the sessions. These limitations of the FC can be overcome by proper planning and improving the content and method after collecting feedback from students. Phillips and Wiesbauer have in a short communication described an excellent framework for implementation of the FC model as well as given a checklist for the best practices.[19]
CONCLUSION
Due to change in curriculum, there is less formal time for teaching pharmacology. There is also increased emphasis on self-directed learning and small group discussions. The FC method in addition to engaging students in an active and collaborative learning process is also valuable in introducing students to important topics in the subject outside of the formal curricular time. While there is a generally favourable mindset of students toward FC, there was no significant improvement in academic performance. Studies which involve the students for a greater length of time in the FC method in pharmacology are needed.
Acknowledgement
We thank the faculty of the Department of Pharmacology, undergraduate students and the Medical Education Unit for their relentless support and encouragement in the successful completion of the study. There are no conflicts of interest.
Ethical approval
The research/study approved by the Institutional Review Board at Government Medical College, Thiruvananthapuram, number HEC No.01/17/2022/MCT dated 26 February 2022.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Inverted classroom by topic-A study in mathematics for electrical engineering students. Int J Eng Pedag. 2014;4:11-7.
- [CrossRef] [Google Scholar]
- The flipped classroom improves student achievement and course satisfaction in a statistics course: A quasi-experimental study. Teach Psychol. 2016;43:10-5.
- [CrossRef] [Google Scholar]
- Flipped classroom versus traditional textbook instruction: Assessing accuracy and mental effort at different levels of mathematical complexity. Technol Knowl Learn. 2014;20:231-48.
- [CrossRef] [Google Scholar]
- Evaluation of a flipped classroom approach to learning introductory epidemiology. BMC Med Educ. 2018;18:63.
- [CrossRef] [PubMed] [Google Scholar]
- Flipped classroom: Do students perceive readiness for advanced discussion? J Nurs Educ. 2018;57:163-5.
- [CrossRef] [PubMed] [Google Scholar]
- A novel integration of online and flipped classroom instructional models in public health higher education. BMC Med Educ. 2014;14:181.
- [CrossRef] [PubMed] [Google Scholar]
- The effectiveness of the flipped classroom on students' learning achievement and learning motivation: A meta-analysis. Educ Technol Soc. 2020;23:1-15.
- [Google Scholar]
- Facing the challenges in ophthalmology clerkship teaching: Is flipped classroom the answer? PLoS One. 2017;12:e0174829.
- [CrossRef] [PubMed] [Google Scholar]
- Advances in medical education and practice: Student perceptions of the flipped classroom. Adv Med Educ Pract. 2017;8:63-73.
- [CrossRef] [PubMed] [Google Scholar]
- Randomised controlled trial of a blended learning evaluation intervention for teaching evidence-based medicine. BMC Med Educ. 2015;15:39.
- [CrossRef] [PubMed] [Google Scholar]
- A meta-analysis of outcomes comparing flipped classroom and lecture. Am J Pharm Educ. 2018;82:6898.
- [CrossRef] [PubMed] [Google Scholar]
- Measuring the impact of the flipped anatomy classroom: The importance of categorizing an assessment by Bloom's taxonomy. Anat Sci Educ. 2017;10:170-5.
- [CrossRef] [PubMed] [Google Scholar]
- A flipped classroom in graduate medical education. Clin Teach. 2020;17:195-9.
- [CrossRef] [PubMed] [Google Scholar]
- An introduction to the inverted/flipped classroom model in education and advanced training in medicine and in the healthcare professions. GMS J Med Educ. 2016;33:Doc46.
- [Google Scholar]
- Motivation and cognitive load in the flipped classroom: Definition, rationale and a call for research. Higher Educ Res Dev. 2015;34:1-4.
- [CrossRef] [Google Scholar]
- Test-enhanced learning in medical education. Med Educ. 2008;42:959-66.
- [CrossRef] [PubMed] [Google Scholar]
- Lecture halls without lectures-a proposal for medical education. N Engl J Med. 2012;366:1657-9.
- [CrossRef] [PubMed] [Google Scholar]
- Enhancing teacher-student interaction and students' engagement in a flipped translation classroom. Front Psychol. 2021;12:764370.
- [CrossRef] [PubMed] [Google Scholar]
- The flipped classroom in medical education: A new standard in teaching. Trends Anaesth Crit Care. 2022;42:4-8.
- [CrossRef] [PubMed] [Google Scholar]




