
Translate this page into:
A quasi-experimental study to compare the acquisition of basic clinical skills in novice medical students taught by George and Doto’s five-step method compared to those taught by the traditional approach (SODOTO)
*Corresponding author: Swapnil Paralikar, Associate Professor, Department of Physiology, Government Medical College, Bhavnagar, Gujarat, India. drsparalikar@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Paralikar S, Shah C, Kapoor A, Parmar U. A quasi-experimental study to compare the acquisition of basic clinical skills in novice medical students taught by George and Doto’s five-step method compared to those taught by the traditional approach (SODOTO). Indian J Physiol Pharmacol 2022;66:75-80.
Abstract
Objectives:
The aim of this study was to compare the acquisition of basic clinical skills by George and Doto’s five step method compared to the Traditional SODOTO approach, and to ascertain the perception of the students regarding these diverse methods.
Materials and Methods:
Fifty-four 2nd MBBS 1st semester students posted in the Department of Medicine at GMERS, Gotri, were enrolled for the study. After teaching the theory, both groups were taught per abdomen (P/A) examination and respiratory system (R/S) examination – one system by the five-step method and the other by the SODOTO approach. Skill acquisition was tested by pre-validated checklists. Finally, feedback was collected on the perception of students using a pre-validated questionnaire. The data were analysed using GraphPad.
Results:
There was an average 20% improvement (P < 0.001) in the group taught by the five-step method compared to the one taught by the traditional approach (P/A – 45.14/60 [5.64] vs. 57.86/60 [1.83] [Group B vs. Group A]) (R/S examination – 26.17/40 [6.65] vs. 34.79/40 [3.56] [Group A vs. Group B]).
Conclusion:
George and Doto’s five-step method has been found to be more effective than the traditional SODOTO approach.
Keywords
Basic clinical skills
Medical education
Andragogy

‘The most important innovation in medicine in the next 10 years is the power of the human hand to touch, to comfort, to diagnose and to bring about treatment’ – The renowned Stanford physician, Abhraham Verghese in his 2011 TED talk: A Doctor’s Touch
INTRODUCTION
Acquisition of competency in procedural skills is a fundamental remit of medical training. The National Medical Commission has rolled out a competency-driven curriculum from the academic year 2019–20. This new curriculum lays emphasis on skill development in all phases. In fact, skill development is the ‘soul’ of this competency-driven curriculum.[1]
‘Skill’ has been defined as the ability to perform a task leading to a specific predefined outcome in several domains. In this paper, we refer to basic clinical skills (procedural skills) such as examination of the radial pulse, palpation of the liver, and auscultation of breath sounds.
The challenge of teaching clinical skills is to teach students in such a manner that they learn effectively. The traditional method for teaching clinical skills to medical students is the well-known Halstedian mantra called as ‘See one, do one, teach one’ or popularly called the SODOTO approach. According to this approach, students watch an expert performing the skill, practice themselves and teach their peers [Table 1]. On most occasions, the learning experience is poorly structured and results, in poor acquisition and retention of the clinical skill. Hence, the SODOTO approach is no longer considered appropriate for teaching clinical skills to health professionals.[2,3] Click or tap here to enter text. In addition, a large and growing body of evidence in quality improvement literature suggests the benefits of educational strategies based on sound educational principles over this traditional (and haphazard) approach.[4]
| Steps | Traditional approach (SODOTO) | George and Doto’s five-step method |
|---|---|---|
| 1 2 3 4 5 |
The tutor explains theory and demonstrates procedure The students practice with feedback from the tutor |
Conceptualisation – The tutor explains the cognitive aspects of the skill –when it is done, why it is done Demonstration – The tutor demonstrates the skill exactly as it should be done without talking through the procedure Demonstration with commentary – The tutor repeats the procedure but takes time to describe in detail each step in the process Verbalisation – The student talks through the skill Practice – The students perform the skill. The tutor provides feedback or coaching as needed Following a successful attempt, students should continue to practice until they reach the desired level of proficiency |
In 2001, John H. George and Frank X. Doto proposed a simple five-step method called as ‘George and Doto’s Five-Step Method,’ based on the principles for teaching psychomotor skills.[5] [Table 1]. This method is tailored based on several theories of adult learning. According to Knowles’ ‘Andragogy,’ adults learn better if they know why they need to know a skill, and when they are likely to apply it in the delivery of care. In addition, Albert Bandura’s social cognition theory posits that adults learn by observing someone else performing a task (vicarious experience).[6] However, there is only one study in India, in dental undergraduate students, which has evaluated the effectiveness of this five-step method.[7]
Hence, the aim of this study was to compare the acquisition of basic clinical skills by the third semester medical students (IInd MBBS) taught by George and Doto’s five-step method compared to those taught by the traditional approach (SODOTO) and to evaluate the perception of these students regarding these two diverse methods. Undergraduate medical students in India were previously given only an orientation to basic clinical skills in 1st MBBS (2nd semester). Hence, these students have been considered novices regarding these clinical skills.[8]
MATERIALS AND METHODS
Design of the study
The study employed a quasi-experimental design. It was conducted in the Department of Medicine at GMERS, Gotri, in Vadodara, Gujarat. The study was approved by the Institutional Ethics Committee of the college and was also granted a consent waiver. Fifty-four third semester students posted in the department of medicine were enrolled for the study. The students were apprised of the purpose of the study. Participation in the study was voluntary. Participants were assured that all data obtained would be treated anonymously. The group of 54 students was divided into two groups – Group A (n = 25) and Group B (n = 29) based on their roll numbers. Per abdomen (P/A) and respiratory system (R/S) examinations were selected for providing training and assessing the development of clinical skills. Thus, a total of 10 skills – 6 from P/A and 4 from R/S – which are part of the ‘core’ area of internal medicine, were taught to each group.
These skills are part of the ‘core’ area of internal medicine in the new competency-driven curriculum proposed by the National Medical Commission.[9] Click or tap here to enter text.Both these sets of skills are part of the ‘core’ area of the physiology curriculum as well. However, according to the revised guidelines, the R/S examination also needs to be certified in physiology so that the candidate may be eligible for the University Examination at the end of 1st MBBS.[10] Each of the 10 skills was standardised and demonstrated to the medicine faculty who was part of the study. Scripts for teaching each skill by the five-step method were prepared. Group A was taught P/A by George and Doto’s five-step method and R/S by the traditional approach; while Group B was taught R/S by George and Doto’s five-step method and P/A by the traditional approach.
Interactive lecture
Before the skill teaching session, each group was taught the theory related to the practical. These lectures were conducted in an interactive format with questioning being used as the main method of interaction. Students were questioned after about every 15 min of didactic teaching during a 1 h lecture. Questions were designed before the lecture and focussed on the higher levels of Bloom’s taxonomy, namely application, and analysis.[11]
Skill teaching session
Students were divided into groups of 8–10 for the clinical skill teaching session. To ensure reliability, all the skills were taught by the principal investigator. In one session, an examination of one of the systems was taught. Thus, a total of six skill teaching sessions were conducted for George and Doto’s five-step method. It took about 60–90 min to teach a set of skills by George and Doto’s five-step method. Each student verbalised the sequence of steps in each skill. Each student was also provided feedback when he practised the skill. It took about 20 min to teach a set of skills by the traditional approach. Only one or two students practised the skill in front of the examiner before going on to teach the others in the group. Students were given 2 days to practice independently and under supervision during which feedback was provided by the faculty member.
Assessment
Skill acquisition was tested by two examiners using checklists that were prior validated by a senior medicine faculty from another college. The assessment comprised four sessions – two sessions for the skills taught by George and Doto’s five-step method and two sessions for the skills taught by the traditional approach. Each of the examiners assessed half of the students during each assessment session. The examination was conducted after the practice sessions of the students ended. The examination was conducted on patients admitted to the medicine wards, but not necessarily having clinical features related to the particular organs being examined.
Perception of the students
The perception of students regarding George and Doto’s five-step method was evaluated using a pre-validated semi-structured questionnaire.[12]
Data analysis
Data were entered into an electronic spreadsheet (Microsoft Excel®, Microsoft Corporation, Redmond, WA). The entering of the data was cross-checked. The data were analysed using the statistical software R version 4.0.2. The normality of data was checked by Shapiro–Wilk test. Data distribution was found to be non-Gaussian. The median and interquartile range were calculated for each method in both groups separately. The median scores of the traditional approach were compared with that of the five-step method scores by Mann–Whitney U-test and P ≤ 0.05 with 95% confidence interval was considered for statistical significance.
RESULTS
Fifty-four (n = 54) medical students were included in the study. They were divided into two groups, Group A = 29 and Group B = 25. Examination of the P/A system was taught to Group A by George and Doto’s five-step method and to Group B by the traditional approach.
The mean scores for the P/A system were 57 ± 2/60 versus 45 ± 6/60 (George and Doto’s five-step method vs. the traditional approach, respectively) (P < 0.001). The mean scores for the R/S were 34 ± 4.5/40 versus 25 ± 10.5/40 (George and Doto’s five-step method vs. the traditional approach, respectively) (P < 0.001) [Graph 1].
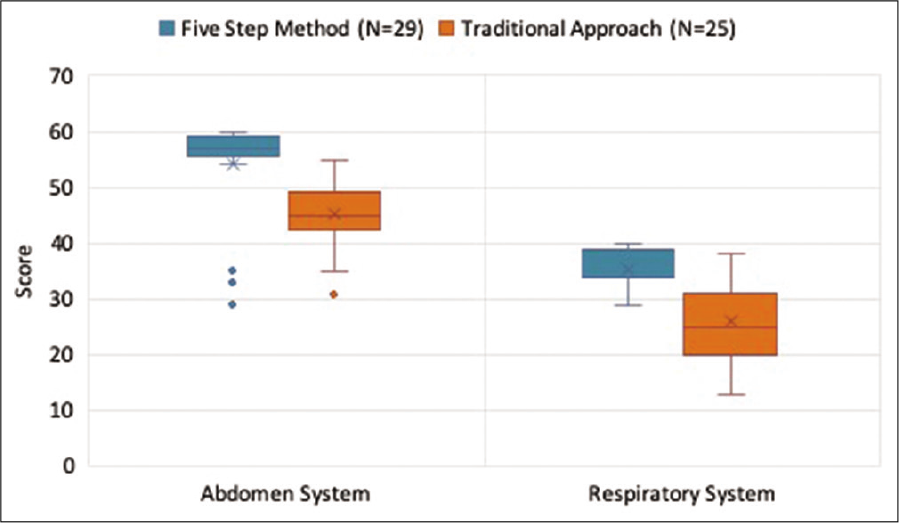
- Median scores of per abdomen system and respiratory system with the five-step method compared to the traditional approach.
The median scores of each of the six skills of P/A system examination were significantly higher in students taught by George and Doto’s five-step method compared to those taught by the traditional approach (P < 0.001) [Graph 2].
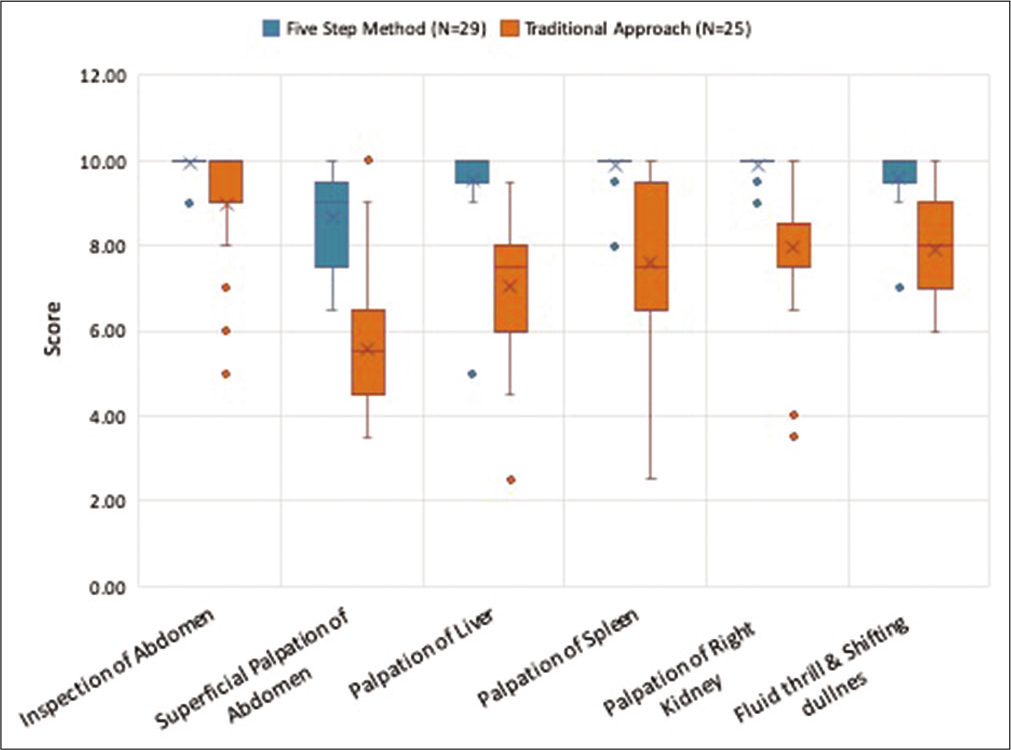
- Comparison of scores of each of the six skills of per abdomen system by the two methods.
The median scores of three of the four skills of R/S examination were significantly higher in students taught by George and Doto’s five-step method compared to those taught by the traditional approach (P < 0.001). The median scores for percussion of the R/S were statistically significant at P < 0.02 [Graph 3].

- Comparison of scores of the four skills of the respiratory system by the two methods.
The perception of the students regarding George and Doto’s five-step method was collected on a Likert scale. Ratings 1 and 2 on the Likert scale were combined to represent ‘disagreement.’ Ratings 4 and 5 on the Likert scale were combined to represent ‘agreement.’ Students agreed that George and Doto’s five-step method was a better guided learning activity compared to the traditional approach (57.89%); they would be able to perform the skill in a better way due to breakdown in small steps (75.44%); they were able to recall the steps easily and would remember for a longer time (75.44%) and that the overall learning experience was enjoyable (62.32%) [Graph 4].
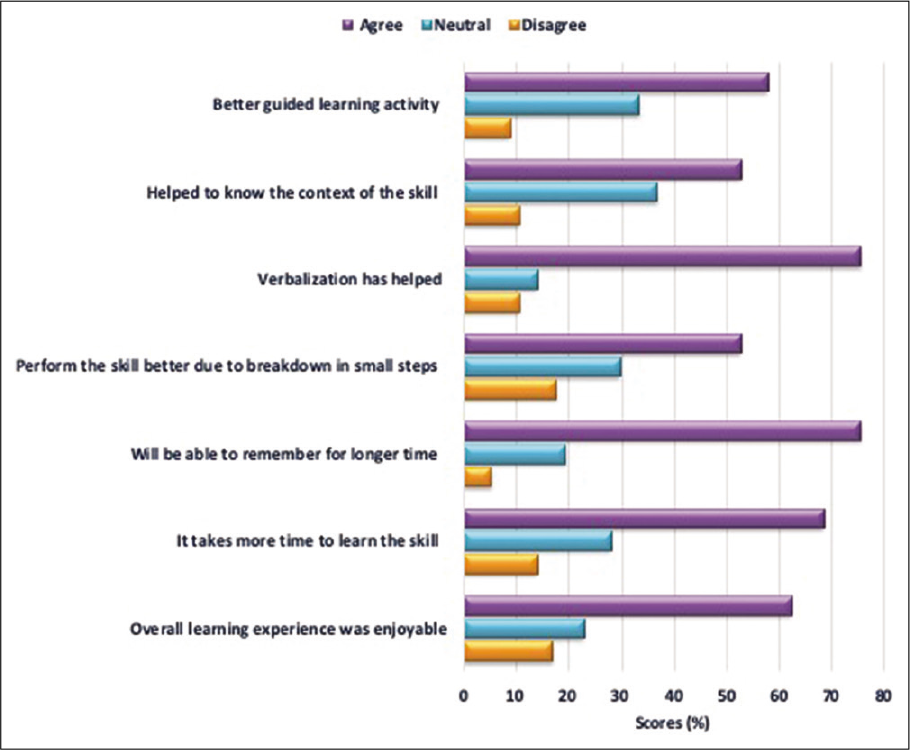
- Perception of students regarding the five-step method (Likert scale – 1=strongly disagree to 5=strongly agree).
DISCUSSION
This study compared the effectiveness of George and Doto’s five-step method compared to the traditional approach for teaching basic clinical skills to novices.
There was a significant improvement in the groups taught by George and Doto’s five-step method compared to the groups taught by the traditional approach. Similar results have been obtained for the five-step method by other researchers.[7,13] Piryani et al. used the five-step method to teach physical examination skills in all major subjects of Phases III and IV at Tribhuvan University, Nepal. The authors reported that, in the objective structured clinical examination, which was conducted after the intervention, 70% of the students scored more than 80%.[13] Virdi and Sood conducted a study on the five-step method in dental undergraduate students. They reported that novice dental students were able to perform the skill effectively just after one teaching session. The authors used sealant retention as an objective evaluation of the skill learnt by students. Sealant retention was 92% when they evaluated at the end of 6 and 12 months; while it was 90% at the end of 18 months.[7] Parmar et al. assessed psychomotor skills in undergraduate medical students taught by Peyton’s four-step method. They reported that this method was superior compared to the traditional method for acquisition of the procedural skills in these fourth semester undergraduate students.[12]
The potential advantages of George and Doto’s five-step method might seem to lie in the combination of the different learning theories for adults embedded in the approach. Step 1 of George and Doto’s five-step method involves telling the learners why they need to learn a specific skill, and when they will be required to apply it for the care of patients. Thus, this step can be said to be effective based on the assumptions of andragogy.[6] During Step 2 of this five-step method, a real-time demonstration of the skill is provided. This step serves to provide a ‘mental model’ or ‘schema’ of the skill. The learner is able to focus on the motor aspect of the skill only, without ‘noise’ from other sensations such as hearing or touch. The mental model also enables the learner to ‘self-evaluate his own performance.’[5,14,15] During Step 3, the preceptor describes each skill while simultaneously performing the skill. Step 3 is an amalgamation of seminal and contemporary skill teaching literature. During Step 4, the student verbalises each step. This process helps him to create a ‘motor map’ of the skill. This map is akin to a pen drive and is a pre-requisite before the skill is then stored in long-term memory (akin to the hard drive of the computer). Finally, during Step 5, the learner performs the skill. The practice of the skill is necessary for the transfer of the skill into long-term memory. Feedback provided at the end of practice ensures that the correct sequences are encrypted into long-term memory.[16,17] The advantages of George and Doto’s five-step method are also supported by the social cognition theory proposed by Albert Bandura. First, setting a clear objective enhances learning. It serves as a guidepost for monitoring and directing progress appropriately. Awareness of the goal increases the energy and effort expended and stimulates the development of strategies to reach the goal. In addition, watching others perform the task enhances an adults’ learning by vicarious capability. An added benefit is that if the initial learning experience is positive, the sense of self-efficacy of the learner is enhanced. Provision of corrective, formative feedback enables the learner to become self-directed, set goals and personal standards, and help him to self-assess himself.[6]
Acceptance ratings were high for the five-step method. The majority of the students expressed the opinion that teaching by the five-step method was a better guided learning activity compared to the traditional approach; they got to understand the context of the skill; they would be able to remember better due to breakdown of the skill in small steps; verbalisation had helped them; they can recall the steps of the skill more easily than with the traditional approach and that they would be able to remember the skill for a longer time. In a study conducted at the Tribhuvan University in Nepal by Piryani et al., the average score on the 5-point Likert scale was a high 4.3.[13] Similar results have been obtained in other studies for Peyton’s 4-step method. Parmar et al. reported a positive experience from the students regarding Peyton’s four-step method. Students expressed the opinion that they could learn clinical skills more effectively. In addition, the students were of the view that the division of the clinical skill in small steps had helped them. The students were also satisfied with the learning experience and suggested that it should be routinely used to teach clinical skills.[12]
In this study, it took more time to teach by George and Doto’s five-step method compared to the traditional approach (60– 90 min vs. 20–30 min). In a study conducted to evaluate the effects of Peyton’s four-step method versus the traditional approach, the length of time required for instruction by Peyton’s 4-step method was comparable to that of the traditional approach. These authors suggested that teachers teaching by the traditional approach may have spent more time explaining the procedure and inviting the participants to ask questions. Thus, the learning experience with the traditional approach may have been augmented. As a result, no significant difference in the scores was observed.[18] In the present study, however, the instructor strictly followed the principles of both approaches; hence, the difference in the scores may be considered more valid.
The limitation of this study is that it was conducted on medical students in their third semester. These students were novices even with regard to basic clinical skills. A similar study should be conducted on senior medical students (6–9 semesters), who could be classified as advanced beginners according to the Dreyfus model.[8] Another limitation was it took a total of six sessions to teach the clinical skills of P/A and respiratory system, by George and Doto’s five-step method. In addition, only one teacher taught all the skills to the students, which may introduce individual bias. Further exploration of this approach should involve a longitudinal study to assess the retention of clinical skills. It would be desirable to address the lacunae of this study during future research.
CONCLUSION
Thus, George and Doto’s five-step method is more effective to teach basic clinical skills compared to the traditional approach (SODOTO). Students perceived a positive learning experience with this approach. This method and other similar approaches, which are based on the principles of adult learning, should be routinely used to teach basic clinical skills to medical students. A paradigm shift in the training of clinical skills from the traditional SODOTO approach to such educational strategies based on sound psychomotor principles will enhance the quality of medical care in the future.
Acknowledgement
I thank Dr. Tejinder Singh (former Director CMC Ludhiana, FAIMER Regional Institute) and currently Professor of Medical Education and Paediatrics, SGRD Institute of Medical Sciences and Research, Amritsar, for his encouragement and support. I thank Dr. Dinesh Badyal, Director (CMC Ludhiana FAIMER Regional Institute) and Professor and Head, Pharmacology, CMC Ludhiana, for his support. I thank, Dr. Varsha Godbole, Professor and Head, Department of Medicine, GMERS Medical College and Reseasrch Centre, Gotri, Vadodara for her support in the implementation of the project. I thank, Dr. Rajesh Kathrotia, Addl. Professor, Department of Physiology, AIIMS Rajkot, for assisting with the statistical analysis. I thank Dr. Sadiya Campwala (formerly – Tutor, Department of Physiology, GMERS Medical College, Gotri, Vadodara) for her assistance in preparing the checklists and for assisting in the assessment.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Seven principles for teaching procedural and technical skills. Acad Med. 2001;76:1080.
- [CrossRef] [PubMed] [Google Scholar]
- Procedural instruction in invasive bedside procedures: A systematic review and meta-analysis of effective teaching procedures. BMJ Qual Saf. 2016;25:281-94.
- [CrossRef] [PubMed] [Google Scholar]
- Teaching and learning in medical education: How theory can inform practice In: Swanwick T, ed. Understanding Medical Education: Evidence, Theory and Practice (2nd ed). New York, United States: Wiley Blackwell; 2013. p. :7-29.
- [CrossRef] [Google Scholar]
- Effectiveness of a five-step method for teaching clinical skills to students in a dental college in India. J Dent Educ. 2011;75:1502-6.
- [CrossRef] [Google Scholar]
- Competency Based Undergraduate Curriculum for the Indian Medical Graduate. India: Medical Council of India. 2018;2:60-142.
- [Google Scholar]
- Competency based Undergraduate Curriculum for the Indian Medical Graduate. India: Medical Council of India. 2018;1:95-98.
- [Google Scholar]
- Taxonomy of Educational Objectives In: The Classification of Educational Goals. Green: Longmans; 1956.
- [Google Scholar]
- Effectiveness of four step approach for procedure (skill) teaching: RCT. SEAJCRR. 2013;2:1-288.
- [Google Scholar]
- Introduction of structured physical examination skills to second year undergraduate medical students. F1000Research. 2013;2:16.
- [CrossRef] [PubMed] [Google Scholar]
- Skill learning and the development of expertise In: Athanou J, ed. Adult Education Psychology. Wentworth Falls, NSW: Social Science Press; 2008. p. :263-8.
- [Google Scholar]
- The evolution of cognitive load theory and its application to medical education. Perspect Med Educ. 2015;4:119-27.
- [CrossRef] [PubMed] [Google Scholar]
- Teaching psychomotor skills in the twenty-first century: Revisiting and reviewing instructional approaches through the lens of contemporary literature. Med Teach. 2016;38:1056-63.
- [CrossRef] [PubMed] [Google Scholar]
- Learning-performance distinction and memory processes for motor skills: A focused review and perspective. Behav Brain Res. 2012;228:219-31.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of Peyton's four-step approach on objective performance measures in technical skills training: A controlled trial. Teach Learn Med. 2011;23:244-50.
- [CrossRef] [PubMed] [Google Scholar]




