
Translate this page into:
A randomised controlled trial of mindfulness-based stress reduction programme for substance abuse patients in deaddiction centre

*Corresponding author: S. Kala Bharathi, Department of Nursing, Saveetha College of Nursing, Saveetha Institute of Medical and Technical Sciences, Chennai, Tamil Nadu, India. drmadhan@care.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Solomon DA, Bharathi SK, Vijayaraghavan R, Krishnan M. A randomised controlled trial of mindfulness-based stress reduction programme for substance abuse patients in deaddiction centre. Indian J Physiol Pharmacol. 2024;68:237-42. doi: 10.25259/IJPP_373_2022
Abstract
Objectives:
This study aimed to see whether a stress reduction programme based on mindfulness could reduce stress in substance-dependence patients. A randomised control design was used.
Materials and Methods:
At the addiction centre, 100 drug addicts were receiving treatment. Using a simple random sampling method, samples are split into 50 experimental drug abuse patient groups and 50 control drug abuse patient groups. Perceived stress scale (PSS) is used to assess the pre-test stress used to analyse the results. The mindfulness-based stress reduction (MBSR) program spanned 8 weeks and catered to a maximum of 25 participants. Each day, two sessions lasting 1 h each were conducted. At the end of the programme, the PSS would be completed once more to assess post-test perceived stress levels and compare them to the outcomes.
Results:
The mean values for the control pre-test, experimental pre-test, control post-test and experimental post-test are 36.9, 36.0, 33.4 and 18.9, respectively. A two-way repeated-measures analysis of variance revealed significant differences among the groups (control and experimental), the tests (pre-test and post-test) and the interaction between the group and test (P < 0.001, < 0.001 and < 0.001, respectively). The control group’s pre-test and post-test did not demonstrate significance (P = 0.265). Conversely, the experimental group exhibited a significant decrease in PSS Score from the pre-test to the post-test (P < 0.001). This shows that the intervention is beneficial in decreasing the PSS score of the participants.
Conclusion:
Individuals receiving treatment at the addiction facility may discover that MBSR proves to be an efficient approach for alleviating stress.
Keywords
Mindfulness-based stress reduction
Substance abuse patients
Perceived stress scale

INTRODUCTION
The history of substance use is extensive, and daily trends in substance use are evolving. It can be challenging to recognise the substance at an earlier level until it starts to exhibit bodily and mental alterations because it is changing the dimension of usage. As a result, it has an adverse influence on public health as a result, and a large number of studies support this.[1] The use of any psychoactive substance or drug, including prescription medications and illicit drugs, is referred to as ‘substance usage’ when it is not medically necessary. In addition to endangering people’s health, using psychoactive substances also threatens the social and economic fabric of their families, communities and nations. Rapid scenario analyses can be useful for analysing patterns in drug use. In India, marijuana (40%), alcohol (30%) and opioids (15%) were the three most frequently used substances, as per a Research Study Analysis conducted by the United Nations Office on Drugs and Crime in 2002 involving 4648 individuals with substance use disorder.[2] Based on a Rapid Situation and Response Assessment involving 5800 male individuals with substance use disorder, 76% of opioid users presently inject heroin, 76% inject buprenorphine, 70% chase and 64% use propoxyphene. The majority of individuals with substance use disorder also drink alcohol concurrently (80%).[3] Despite their job, age or gender, the majority of persons who consume these substances impose a financial strain on the nation due to the costs associated with treating their effects and helping them rehabilitate. Drug use is becoming more prevalent as a result of shifting cultural ideals, escalating economic hardship and deteriorating social ties. Today, drug addiction and drug trafficking are a global scourge that affects every region of the globe. Millions of drug addicts live miserable lives on the edge of death all over the world. India is considerably affected by the trend of drug abuse, and the number of drug users there is increasing daily. Addiction can be effectively controlled. People can recover control of their lives and battle the damaging consequences that addiction has on their brains and behaviour through treatment. Chronic diseases must be treated by correcting engrained behaviours. The deaddiction centre plays a key role in the treatment of people who have addiction or substance dependence. Because addiction is a chronic disorder, relapse or a return to drug use after an attempt to stop can be a part of the process for some individuals. However, current treatments are designed to help prevent recurrence. Relapse rates for drug usage are comparable to those for other chronic illnesses. If individuals stop following their medical treatment plan, people are more prone to relapse.
If one quits following their medical treatment plan, they are more likely to experience a relapse. When patients quit taking drugs for the 1st time, they may experience a variety of physical and psychological symptoms, such as agitation or insomnia, as well as sadness, anxiety and other mental health problems. Additional elements, including a prolonged stay in a rehab facility, being away from family, a protracted period of unemployment, a reduction in income, a lack of self-esteem and uncertainty about the future all raise the stress levels of people receiving treatment for addiction. According to Cleck and Blendy, prolonged exposure to diverse psychological stresses might increase neuropsychiatric illnesses such as drug addiction. Addiction is a chronic brain condition in which people are unable to control their need for substances despite adverse health and social repercussions. Addicts’ brains are changed, and they respond to stress considerably differently from non-addicts’ brains. The impacts of stress and drug usage are frequent throughout the addiction cycle. This higher than normal stress level affects the prognosis and creates an unpleasant scenario that could lead to relapse and a poor therapeutic response. In the fields of clinical science, social-cognitive-affective neuroscience, and basic emotion research, the idea of mindfulness has garnered interest. MBSR includes a variety of mindfulness exercises, such as hatha yoga and both formal and casual meditation. The formal practice includes attention that is breath-centred and body-scanning-based, changing focus among sensory cues and open observation of immediate experience, strolling meditation and mindful eating. Brief pauses during casual practice involve voluntarily changing focus to the present time. These mindfulness exercises are intended to improve one’s capacity for seeing the immediate content of experience, particularly the fleeting character of thoughts, emotions, memories, mental images and bodily sensations.
The MBSR identifies two different categories of brief, attention-focused meditations
(a) Focused attention, which is described as present-time, object-based (for instance, sensations brought on by breathing), intentional selective attention with continuing focus quality evaluation; and (b) open monitoring, characterised by directing attention to a state of simple and direct observation or monitoring of any experience such as thought, emotion or physical sensation.[4] Theoretically, MBSR may enhance emotional regulation and minimise stress, anxiety and depressive symptoms. The Process Model of Emotion Regulation encompasses categories of emotion regulation strategies referred to as Situation Selection, Situation Modification, Attentional Deployment, Cognitive Change and Response Modulation.[5] Extended mindfulness meditation practice and MBSR may have a direct impact on how attention is used, particularly on the capacity to exert cognitive control over negative rumination and greater emotional flexibility and an enhancement in the ability to detach from unpleasant emotional stimuli are both benefits of MBSR.[6,7]
Stress is the outcome of a person’s inability to react correctly to real or imagined dangers to their bodily or emotional well-being. Stress causes a number of physiological reactions, for example, experiencing a state of alarm and an adrenaline rush, employing short-term resistance as a coping mechanism, weariness and irritability, muscle spasms, difficulty concentrating, headaches and an elevated heart rate. Therefore, the present study’s objective was to determine whether an 8-week MBSR programme helped examine the dynamics of changes in the perceived stress, a crucial outcome for participants’ mental health. We predicted that mindfulness would help to reduce the perceived stress, which was in line with earlier findings. In keeping with current concepts that contend that mindfulness programmes serve as a mediator of treatment outcomes. According to the researchers, the MBSR program was delivered over 8 weeks, with two 1-h sessions every day. For 8 weeks following the orientation, participants engaged in structured mindfulness practices aimed at cultivating present-moment awareness and reducing reactivity to stressors.[8,9]
MATERIALS AND METHODS
Participants
In this study, the influence of MBSR on perceived stress was examined. The addiction centre housed 100 substance abuse patients undergoing treatment. Using a simple random sampling method, the samples consist of two groups: 50 individuals who have undergone experimental drug abuse and 50 individuals who serve as controls with substance abuse histories. After being fully informed about the study, participants in the experimental group provided their informed consent. Cohen et al.[10] perceived that the stress scale (PSS) is used to assess and analyse the perceived stress. After the trial period, patients in the control group were taught about MBSR, and they followed the deaddiction facility’s routine during MBSR sessions. The study excludes substance abusers who have recently been admitted, admitted because recently admitted patients are taking detoxification drugs. A separate study examines the results of a 21-day inpatient drug detoxification and rehabilitation programme, assessing factors such as duration of stay, transition to additional treatment and engagement in HIV risky behaviour. The study concludes that 21-day detox programmes when succeeded by residential drug-free treatment, hold promise in diminishing relapse rates among individuals with drug addiction[11] as well as those who have a medical background of seizure disorder. Severe physical illness, aggressive behaviour, hallucinations or hostile behaviour. The study was conducted after getting approval from the Institutional Ethical Committee of Saveetha Medical College and Hospital (005/08/2020/IEC/SMCH) dated 7 August 2020.
The MBSR program had a maximum of 25 participants, two 1-h sessions per day, and it lasted for 8 weeks. The stress level was assessed at the beginning and end of the MBSR programme using the Cohen et al.[10] PSS and compared to the results. Patients were instructed to record their practice time for exercises such as meditation, walking meditation and body scans for 8 weeks after the orientation. Patients were instructed to engage in formal practice for a minimum of 15–45 min during the initial session. By the 8th week, patients attended a 2-hour session, which encompassed a practice session and a nutrition discussion following the KabatZinn programme. The Stress Reduction and Relaxation Clinic at the Massachusetts Medical Centre served as the foundation for the programme developed by Jon Kabat-Zinn et al.,[12] on which the MBSR intervention was constructed. Mindfulness involves the ability to redirect one’s complete attention from thoughts to present awareness. MBSR is a therapeutic regimen designed to empower individuals in self-regulating their arousal levels when confronted with stressful circumstances or symptoms. Through meditation practice, the programme aims to heighten patients’ awareness of their thoughts and emotions. In addition, it provides techniques for monitoring and managing emotions and thoughts during stressful situations to prevent emotional distress.
PSS
The PSS, developed by Cohen et al.[10] in 1983, was utilised in this study. It employs a 14-question format to gauge overall stress perception within the previous month, as well as attitudes and emotions regarding stressful events, perceived control, coping mechanisms and overcoming stress. Responses are rated on a 5-point Likert scale ranging from 0 to 4, with descriptors such as ‘never’ (0 points), ‘almost never’ (1 point), ‘occasionally’ (2 points), ‘fairly frequently’ (3 points) and ‘very frequently’ (4 points). Notably, items 4, 5, 6, 7, 9, 10 and 13 are scored in reverse order (never = 4, very frequently = 0). The scale yields a range of scores from 0 to 56, with higher scores indicative of greater perceived stress. Extensive research has been conducted to assess the reliability and validity of the PSS, with a reported Cronbach’s alpha of 0.86 for the 14-item version.
Statistical analysis
For statistical analysis, the mean ± standard error of the mean of the PSS total was presented for items showing both decreases and increases in score separately. The analysis employed a two-way repeated-measures analysis of variance (RM ANOVA) for within-factor repetition and Bonferroni’s t-test for post hoc multiple comparisons. Factor A represented the groups (control and experimental) for between-group comparison, while Factor B represented tests (pre-test and post-test) for within-group comparison (repetition factor). Statistical significance was established at a probability level of 0.05 or lower. Sigma Plot version 14.5 (Systat Software Inc., San Jose, USA) was employed for both statistical analysis and graph plotting.
RESULTS
The mean and standard error of the PSS is presented in Table 1. Specifically, the means for the control pre-test, experimental pre-test, control post-test and experimental post-test are 36.9, 36.0, 33.4 and 18.9, respectively. The two-way RM ANOVA indicated significant differences among the groups (control and experimental), among the tests (pre-test and post-test), and in the interaction between group and test (all with P < 0.001). The control pre-test and post-test did not show significance (P = 0.265). The experimental pre-test and post-test showed a decrease in PSS scores and were statistically significant (P < 0.001). This shows that the intervention is beneficial in decreasing the PSS score of the participants [Figure 1].
| S. No. | Groups and comparisons | Groups | PSS |
|---|---|---|---|
| 1 | Control | Pre-test | 38.94±0.5 |
| Experimental | Pre-test | 37.74±0.5 | |
| Control | Post-test | 38.75±0.5 | |
| Experimental | Post-test | 24.04±0.5 | |
| 2 | Significance among groups (Control and Experimental) |
F=94.489 P<0.001 |
|
| Significance among tests (Pre-test and Post-test) |
F=1046.288 P<0.001 |
||
| Significance in the interaction (groups X tests) |
F=457.626 P<0.001 |
||
| 3 | Significance between pre-tests (Control and Experimental) |
t=1.119 P=0.265 |
|
| Significance between post-tests (Control and Experimental) |
t=16.943 P<0.001 |
||
| 4 | Significance within control (Pre-test and Post-test) |
t=0.485 P=0.630 |
|
| Significance within experimental (Pre-test and Post-test) |
t=26.227 P<0.001 |
||
PSS: Perceived stress scale. Table 1 displays the mean and standard error of the PSS. Specifically, the means for the control pre-test, experimental pre-test, control post-test and experimental post-test are 38.94, 37.74, 38.75 and 24.04, respectively. Paired t-tests were employed to compare the means of the pre-test and post-test. The control pre-test and post-test did not show significance (P=0.630). The experimental pre-test and post-test showed a decrease in PSS Score and were statistically significant (P<0.001). This shows that the intervention is beneficial in decreasing the PSS score of the participants
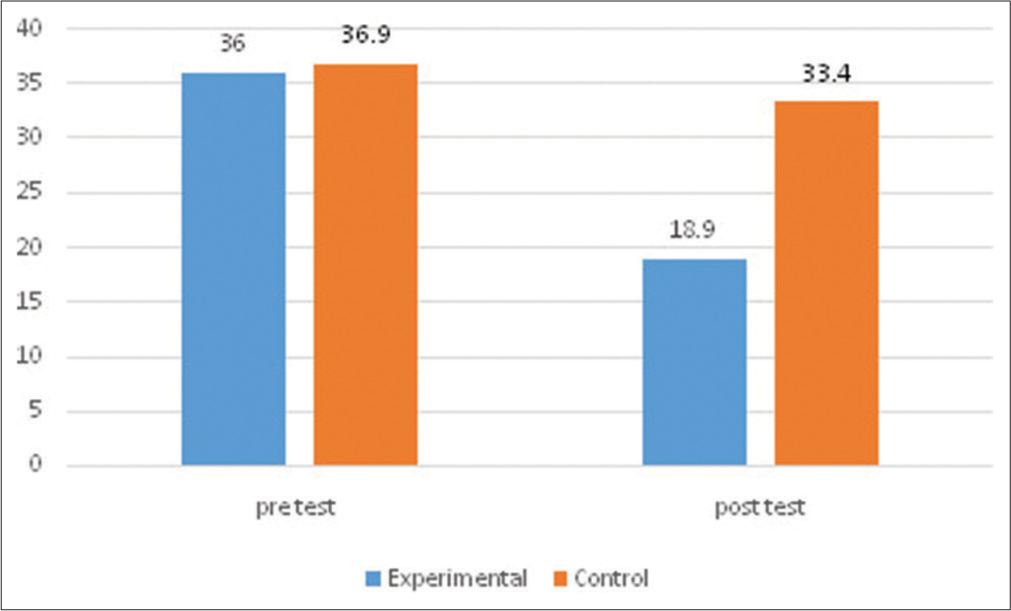
- Effectiveness of mindfulness-based stress reduction programme on perceived stress scale in control (Con) and experimental (Exp) groups.
DISCUSSION
The objective of the study was to assess the effectiveness of MBSR reduced perceived stress. Even though MBSR is recognised as a successful therapy for stress and emotional symptoms, its effectiveness in the treatment of substance abuse patients must be investigated because stress has a significant impact on prognosis. According to research findings, MBSR is an efficient approach for treating a wide range of psychological disorders. The research investigated the impact of engaging in a mindfulness meditation-centred stress reduction programme on mood disruption and stress indicators among cancer outpatients. Individuals in the intervention group demonstrated significantly reduced overall mood disruption and subscales related to depression, anxiety, anger and confusion, along with increased vitality compared to participants in the control group.[13,14] This finding of the studies carried out in a therapeutic community demonstrates that there were no abrupt decreases in anxiety and rumination after mindfulness-based cognitive therapy and that the average path of change in worry and rumination was likewise quite linear. The findings suggest a dose-response relationship; the more MBSR sessions participants attended and the more days they participated in a structured mindfulness exercise, the greater these findings imply that an MBSR programme may affect people’s physiological reactions to stress.[15]
The study by Carlson et al. suggests that the use of MBSR could improve male drug users’ health-related quality of life (HRQOL). This result agreed with earlier research findings about the positive effects of MBSR on HRQOL. It was found that MBSR significantly improved overall quality of life, symptoms of stress and sleep quality in research on outpatients with breast and prostate cancer.[16] Studies suggest through their impact on stress, MBSR or other mindfulness programmes may be helpful in reducing alcohol problems on college campuses.[17-20] Individuals with a history of trauma were given MBSR practice in a community-based drug rehabilitation environment. The demographic comprised highly marginalised and economically disadvantaged African American and Latina women with a history of trauma. Through an iterative feedback process, the structured methods of MBSR were tailored to meet the specific needs of this population. The community’s low literacy levels were also taken into consideration. Adaptations focused on addressing the role of stress in preventing relapse and targeted common effects of addiction and trauma, such as shortened attention span, heightened sensitivity in certain body areas triggering painful memories and reduced ability to focus. With appropriate modifications, MBSR has the potential to serve as a relapse prevention tool during the early stages of recovery. Client feedback indicated a high level of acceptance and satisfaction with the program.[18]
To improve the patient’s mental state, MBSR employs the following mechanisms: To begin, mindfulness promotes enhanced awareness of what is happening in each moment, with an accepting attitude, rather than being involved in habitual thoughts, emotions and behavioural patterns. Increased awareness then leads to new methods of responding and coping with oneself and the environment around us. Mindfulness cultivates a sense of self that transcends ideas, feelings and physiological sensations such as pain. Clients create an ‘observer-self ’ through mindfulness activities. They can now notice their thoughts and emotions in a non-judgmental and nonreactive way that they earlier prevented. Previously ignored thoughts and feelings may now be viewed objectively and without judgment. Clients learn to be aware of their thoughts without acting on them, being dominated by them or believing them.[19] The strength of this study is the usage of MBSR to relieve stress on a less well-studied problem. Our data show that following an effective administration of the MBSR programme, there is a considerable reduction in the level of stress among substance misuse patients receiving treatment in a de-addiction centre. As a result, persons undergoing long-term treatment in addiction treatment facilities will be able to use this treatment. MBSR will alter the patient’s lifestyle, which will be aggravated by their condition. Future research should assess the efficacy of MBSR and other standard and newer cognitive behavioural therapies in patients receiving treatment in addiction treatment clinics.
Limitations
Smaller sample sizes due to a high number of men were excluded because they had comorbidities. Due to the unavailability of the addiction centre, a large number of people cannot be taken.
CONCLUSION
The study’s findings, which reveal that persons in the experimental group who received an MBSR programme had less stress than those in the control group, provide strong evidence for MBSR’s effectiveness in stress reduction. The observed reduction in participants’ stress levels demonstrates the efficacy of MBSR procedures in improving coping strategies and emotional regulation, both of which are critical components of the recovery process. Furthermore, including mindfulness techniques in addiction treatment programmes not only relieves stress but also promotes general well-being and resilience, both of which are necessary for long-term sobriety. These findings highlight the importance of using mindfulness-based techniques as a supplemental therapeutic tool in the comprehensive care of drug misuse patients, providing hope for better treatment outcomes and stress reduction.
Ethical approval
The study was conducted after getting approval from the Institutional Ethical Committee of Saveetha Medical College and Hospital (005/08/2020/IEC/SMCH) dated 7 August 2020.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Substance use and addiction research in India. Indian J Psychiatry. 2010;52:S189-99.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence, pattern and familial effects of substance use among the male college students-a north Indian study. J Clin Diagn Res. 2013;7:1632-6.
- [CrossRef] [PubMed] [Google Scholar]
- Rapid situation and response assessment of drugs and HIV in Bangladesh. Bhutan, India, Nepal and Srilanka: A regional report; Available from: https://www.unodc.org/pdf/india/26th_june/rsra%20report%20(24-06-08).pdf [Last accessed on 2009 Dec 20]
- [Google Scholar]
- Attention regulation and monitoring in meditation. Trends Cogn Sci. 2008;12:163-9.
- [CrossRef] [PubMed] [Google Scholar]
- The emerging field of emotion regulation: An integrative review. Rev Gen Psychol. 1998;2:271-99.
- [CrossRef] [Google Scholar]
- The effects of mindfulness meditation on cognitive processes and affect in patients with past depression. Cogn Ther Res. 2004;28:433-55.
- [CrossRef] [Google Scholar]
- Attention regulation and monitoring in meditation. Trends Cogn Sci. 2008;12:163-9.
- [CrossRef] [PubMed] [Google Scholar]
- Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J Behav Med. 2008;31:23-33.
- [CrossRef] [PubMed] [Google Scholar]
- Using self-report assessment methods to explore facets of mindfulness. Assessment. 2006;13:27-45.
- [CrossRef] [PubMed] [Google Scholar]
- A global measure of perceived stress. J Health Soc Behav. 1983;24:385-96.
- [CrossRef] [PubMed] [Google Scholar]
- Outcomes of a 21-day drug detoxification program: Retention, transfer to further treatment, and HIV risk reduction. Am J Drug Alcohol Abuse. 1995;21:1-16.
- [CrossRef] [PubMed] [Google Scholar]
- Four-year follow-up of a meditation-based program for the self-regulation of chronic pain: Treatment outcomes and compliance. Clin J Pain. 1985;2:159-73.
- [CrossRef] [Google Scholar]
- Mindfulness-based stress reduction in Massachusetts correctional facilities. Prison J. 2007;87:254-68.
- [CrossRef] [Google Scholar]
- Managing cancer pain with nonpharmacologic and complementary therapies. J Am Osteopath Assoc. 2007;107(12 Suppl 7):ES15-21.
- [Google Scholar]
- Mindfulness-based interventions for anxiety and depression. Psychiatr Clin North Am. 2017;40:739-49.
- [CrossRef] [PubMed] [Google Scholar]
- Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosom Med. 2003;65:571-81.
- [CrossRef] [PubMed] [Google Scholar]
- Mindfulness and alcohol problems in college students: The mediating effects of stress. J Am Coll Health. 2013;61:371-8.
- [CrossRef] [PubMed] [Google Scholar]
- Adaptation of mindfulness-based stress reduction program for addiction relapse prevention. Humanist Psychol. 2009;37:192-206.
- [CrossRef] [Google Scholar]
- Mieux vivre avec la douleurchroniquegrâce à la thérapied'acceptationetd'engagement [Acceptance and commitment therapy in the treatment of chronic pain] Sante Ment Que. 2013;38:131-52.
- [CrossRef] [PubMed] [Google Scholar]
- Making a bad thing worse: Adverse effects of stress on drug addiction. J Clin Invest. 2008;118:454-61.
- [CrossRef] [PubMed] [Google Scholar]




