
Translate this page into:
A study of outcome in COVID-19 patients receiving casirivimab-imdevimab
*Corresponding author: Prabhanjan Kulkarni, Department of Medicine, Government Medical College, Aurangabad, Maharashtra, India. prabhanjankulkarni1994@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kulkarni P, Chintale KN, Bhattacharya M, Kulkarni M, Chape S. A study of outcome in COVID-19 patients receiving casirivimab-imdevimab. Indian J Physiol Pharmacol 2023;67:100-4.
Abstract
Objectives:
In December 2019, coronavirus disease 2019 (COVID-19) was first identified in Wuhan, China, as a respiratory tract infection causing symptoms, such as fever, chills, dry cough, fatigue, and shortness of breath. Despite the low mortality rate of COVID-19, patients with comorbidities such as hypertension, cardiovascular disease, and diabetes mellitus seem to be prone to more severe symptoms and to a higher mortality rate than others. Such patients are shown to benefit from usage of monoclonal antibodies. Casirivimab-imdevimab is a cocktail made up of two non-competing, neutralizing human immunoglobulin G1 antibodies that target the receptor binding domain of the severe acute respiratory syndrome coronavirus 2 spike protein and block viral entry into human cells. We assessed the clinical profile and outcome of 42 patients who received the antibody cocktail.
Materials and Methods:
Casirivimab-imdevimab was administered to COVID-positive patients with mild severity. Forty-two patients who satisfied the inclusion criteria received casirivimab-imdevimab and were included in the study. Demographic and clinical data were tabulated in Microsoft Excel and statistics were run in OpenEpi software.
Results:
No adverse reactions were seen in any of the patients. Among the 42 patients, there were no deaths. Twenty-two (52.3%) patients improved, while 20 (47.6%) worsened after receiving the antibody cocktail. Out of 21 (50%) patients who did not have any comorbidity, 13 (30.9%) worsened after receiving the drug and 8 (19%) improved, while among those with comorbidities, 7 (16.6%) worsened and 14 (33.3%) improved (P < 0.05). Thirteen (30.9%) unvaccinated patients improved, while 14 (33.3%) worsened, whereas 6 (14.2%) fully vaccinated patients improved while only 2 (4.7%) worsened. Among the patients who were administered the cocktail within 5 days of onset of symptoms, 12 (28.5%) improved and 10 (23.8%) worsened, whereas among those who received the drug between 6 and 10 days of symptom onset, ten improved, and ten worsened. There was no statistically significant association between vaccination status and outcome, and infusion interval and outcome in these patients.
Conclusion:
None of the 42 patients developed any reaction to casirivimab-imdevimab. There were no deaths in the study population. About 52.3% of the patients improved and 47.6% worsened after receiving the cocktail. About 33.3% of the comorbid patients improved. There was no statistically significant association between vaccination status and outcome, and infusion interval and outcome in these patients.
Keywords
Severe acute respiratory syndrome coronavirus 2
Cocktail
Antibody
Casirivimab
Imdevimab

INTRODUCTION
In December 2019, coronavirus disease 2019 (COVID-19) was first identified in Wuhan, China, as a respiratory tract infection causing symptoms, such as fever, chills, dry cough, fatigue, and shortness of breath. Despite the low mortality rate of COVID-19, patients with comorbidities such as hypertension, cardiovascular disease, and diabetes mellitus seem to be prone to more severe symptoms and to a higher mortality rate than others.[1]
COVID-19 infection is categorized as asymptomatic, mild, moderate, and severe. Asymptomatic illness is incidentally detected with no other signs or symptoms. A patient is said to be having mild illness if he has no shortness of breath, no difficulty in breathing, respiratory rate <24/min, and oxygen saturation (SpO2): ≥94% on room air. Moderate illness is one where patient has shortness of breath, difficulty in breathing, respiratory rate more than 24 but <30/min, and SpO2: 90–93% on room air. Severe illness is characterized by severe shortness of breath, difficulty in breathing, respiratory rate of more than 30/min, and SpO2: <90% on room air.[2]
Risk factors for disease progression and worse outcomes are increasingly being spelled out and subgroups of patients at added risk merit careful monitoring and therapy. Monoclonal antibodies that target spike proteins of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been evaluated in outpatients with mild-to-moderate disease and risk factors for severe disease. Casirivimabimdevimab is a cocktail made up of two non-competing, neutralizing human immunoglobulin G1 antibodies that target the receptor binding domain of the SARSCoV-2 spike protein and block viral entry into human cells.[3] Food and Drug Administration issued an emergency use authorization (EUA) for the investigational monoclonal antibodies casirivimab and imdevimab for the treatment of mild-to-moderate COVID-19 in adults and pediatric patients with positive results of direct SARS-CoV-2 viral testing who are ≥12 years of age weighing ≥40 kg, and who are at high risk for progressing to severe COVID-19 and/or hospitalization. High-risk factors include obesity, pregnancy, chronic kidney disease, diabetes, immunosuppressive disease or immunosuppressive treatment, cardiovascular disease (including congenital heart disease) or hypertension, chronic lung diseases, sickle cell disease, and neurodevelopmental disorders or other conditions that confer medical complexity (for example, genetic or metabolic syndromes and severe congenital anomalies) or having a medical-related technological dependence (for example, tracheostomy, gastrostomy, or positive pressure ventilation [not related to COVID-19]).[4]
Government of India approved the antibody cocktail under EUA in May 2021. The cocktail is available as a vial which has adequate dose for administration to two individuals. Once opened and reconstituted, it should be administered within 48 h after storage at 4–8°C.[5]
We assessed the clinical profile and outcome of 42 patients who received the cocktail at the institute.
MATERIALS AND METHODS
The antibody cocktail casirivimab-imdevimab was made available through government supply and it was administered to the patients free of cost. The drug was given as per the guidelines by the manufacturer. Approval from institutional ethics committee (IEC) was obtained (IEC approval no. 01/2022). Written and informed consent from the patients was obtained before infusion.
Inclusion criteria
Mild COVID-19 infection, age more than 12 years, weight at least 40 kg, patients having comorbidities or at high risk for severe COVID-19, elderly patients, and patients having rapid antigen test/reverse transcription polymerase chain reaction (RTPCR) positive report presenting within 10 days of symptom onset were included in the study.
Exclusion criteria
Pregnant and lactating females, RTPCR-negative patients, presentation more than 10 days after onset of symptoms, and patients having severe or critical COVID-19 infection were excluded from the study.
It was administered in the in-patient COVID-19 ward. Standard operating procedure guidelines were prepared for the administration of antibodies. Casirivimab 600 mg and imdevimab 600 mg were reconstituted in 100 mL of normal saline and infused intravenously over 20 min. Patients were observed for adverse drug reactions for 4 h after administration in the ward and then were isolated at home as per Government of India guidelines for mild COVID-19 patients.[6] They were provided with self-monitoring charts, in which their symptoms and vital parameters such as pulse rate, SpO2, and urine output were recorded. They were asked to report immediately in case of development of symptoms such as fever, rash, breathlessness, palpitations, chest pain or reduced urine output, or signs like pulse rate >100 beats/min, resting SpO2 <94%, or a positive 6-min walk test.[7] Clinical worsening and recovery were considered as outcome parameters. Fall in SpO2 <94% on room air requiring supplemental oxygen (and mandating the use of remdesivir as standard of care) was considered as clinical worsening. Relief from symptoms and stable vital parameters with a negative 6-min walk test was considered as recovery.
Data were collected in the Google sheet and a live data were captured. Demographic and clinical data were tabulated in Microsoft Excel and statistics were run in OpenEpi software using percentages. P < 0.05 was considered significant.
RESULTS
Out of 101 patients considered for infusion of the cocktail, casirivimab-imdevimab cocktail was given to 42 patients satisfying the inclusion criteria [Figure 1]. The median age was 57.5 ± 15.79 years. There were 28 male and 14 female patients.
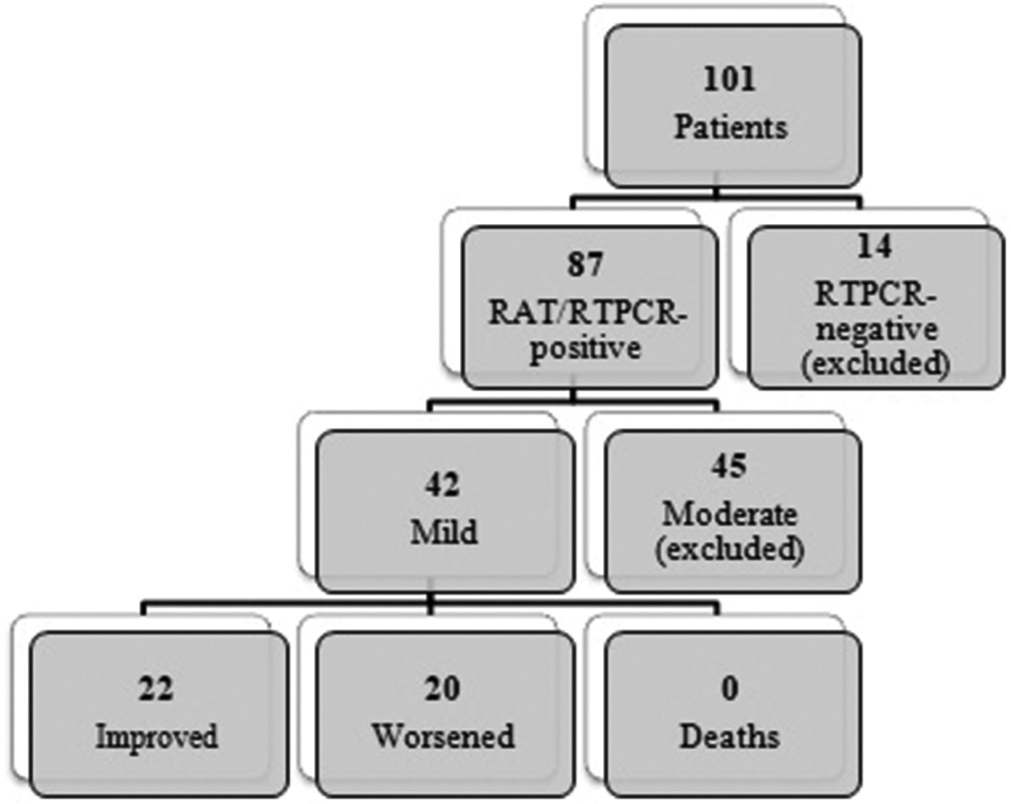
- Distribution of study population. RAT: Rapid antigen test, RTPCR: Reverse transcriptase polymerase chain reaction.
Results are shown in [Table 1 and Figures 2-4]. The duration between onset of symptoms and infusion of the drug is labeled as infusion interval.
| Improved (n1=22) (%) | Worsened to require oxygen and remdesivir (n2=20) (%) |
Total (42) (%) | |
|---|---|---|---|
| Comorbidities (Graph 1) | |||
| None | 8 (19) | 13 (30.9) | 21 (50) |
| Comorbid (DM/HTN/heart disease/others) | 14 (33.3) | 7 (16.6) | 21 (50) |
| Chi-square: 3.3436, P=0.03189 (<0.05) | |||
| Vaccination status (Graph 2) | |||
| None | 13 (30.9) | 14 (33.3) | 27 (64.2) |
| 1 dose | 3 (7.1) | 4 (9.5) | 7 (16.6) |
| 2 doses | 6 (14.2) | 2 (4.7) | 8 (19) |
| Chi-square: 2.089, degrees of freedom: 2, P=0.3518 | |||
| Infusion interval (Graph 3) | |||
| Within 5 days | 12 (28.5) | 10 (23.8) | 22 (52.3) |
| After 5 days | 10 (28.5) | 10 (28.5) | 20 (47.6) |
| Chi-square: 0.08678, P=0.3842 | |||
DM: Diabetes mellitus, HTN: Hypertension, n is the total number of subjects (42). n1 and n2 is the number of patients who improved (22) and worsened (20) after administration of the drug respectively.
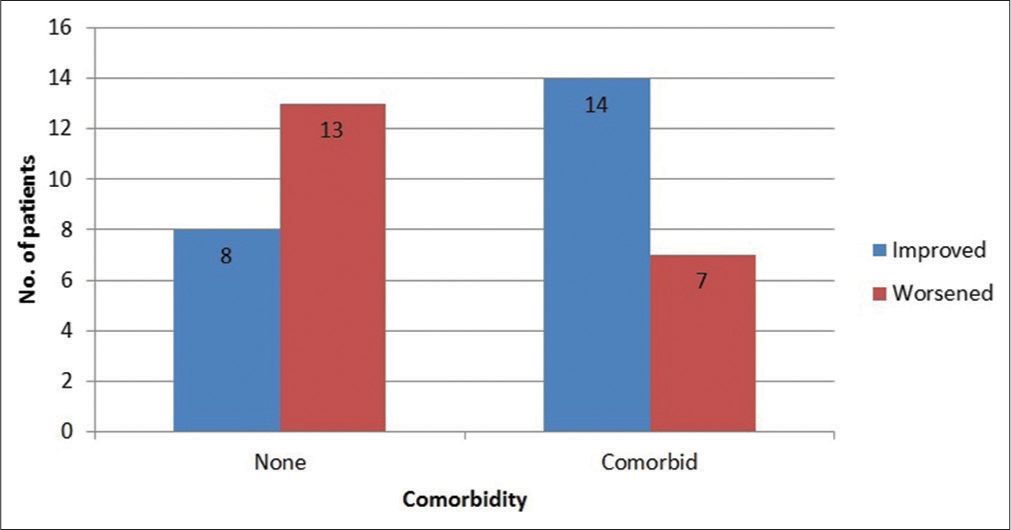
- Association between comorbidity and infusion interval in patients who worsened (n=20).
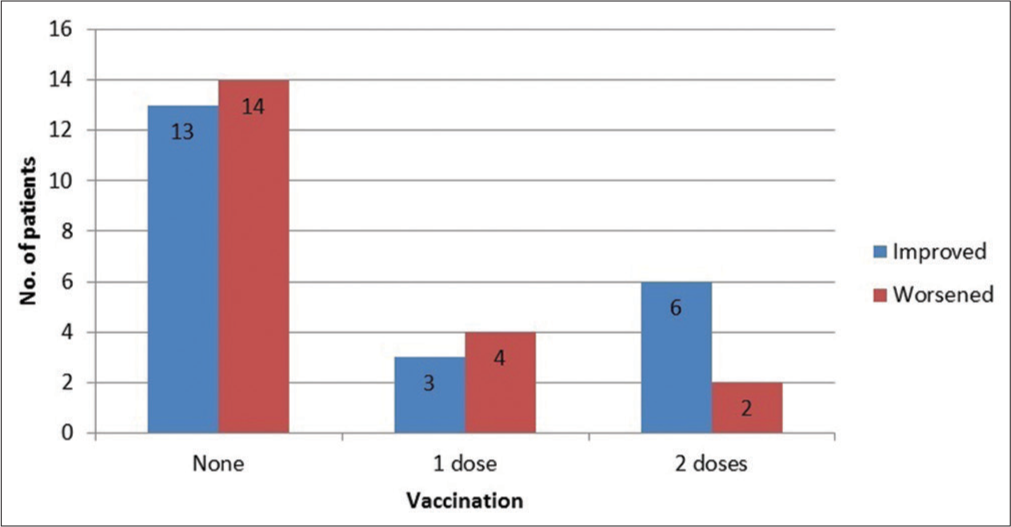
- Vaccination status.
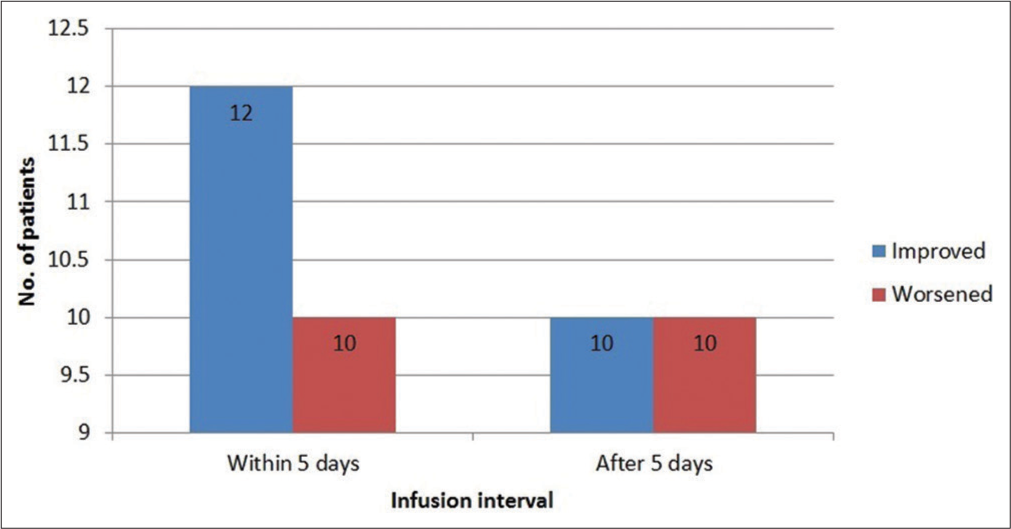
- Infusion interval.
DISCUSSION
No adverse reactions were seen in any of the 42 patients receiving the drug. There were no deaths. Twenty-two (52.3%) patients improved while 20 (47.6%) worsened after receiving the antibody cocktail. Out of 21 (50%) patients who did not have any comorbidity, 13 (30.9%) worsened after receiving the drug and 8 (19%) improved, while among those with comorbidities, 7 (16.6%) worsened, and 14 (33.3%) improved [Figure 2]. This result was statistically significant (P < 0.05). Thirteen (30.9%) unvaccinated patients improved while 14 (33.3%) worsened, whereas 6 (14.2%) fully vaccinated patients improved while only 2 (4.7%) worsened [Figure 3]. Among the patients who were administered the cocktail within 5 days of onset of symptoms, 12 (28.5%) improved and 10 (23.8%) worsened, whereas among those who received the drug between 6 and 10 days of symptom onset, ten improved and ten worsened [Figure 4]. In a similar study by Venkitakrishnan et al., 26 out of 29 patients (89.6%) improved after administration of the drug.[5]
The reason why more patients in the non-comorbid group worsened after administration of the drug as compared to the comorbid group is unclear. Majority of them were unvaccinated, however, that association was not statistically significant [Table 2]. Maximum non-comorbid patients also received the drug after 5 days of onset of symptoms. This association was also not statistically significant [Table 3]. Eight of the 13 patients who were non-comorbid and worsened after the infusion had a computed tomography (CT) severity score of more than 8/25 before infusion, suggestive of presence of advanced disease process before infusion itself. This may be the reason for the observed worsening in non-comorbid patients as compared to comorbid patients receiving the drug. As routine CT scans for mild disease are not recommended as per Government of India guidelines,[2] CT imaging of all patients was not done; hence, we were unable to determine whether the association of pre-infusion CT severity score and worsening of disease was significant.
| Comorbidity | Vaccination status (1 dose is also considered as vaccinated) | Improved (n1=22) (%) | Worsened to require oxygen and remdesivir (n2=20) (%) | Total (42) (%) |
|---|---|---|---|---|
| Comorbid | Vaccinated | 7 (16.6) | 4 (9.52) | 11 (26.1) |
| Unvaccinated | 7 (16.6) | 3 (7.14) | 10 (23.8) | |
| Non-comorbid | Vaccinated | 2 (4.76) | 2 (4.76) | 4 (9.52) |
| Unvaccinated | 6 (14.2) | 11 (26.1) | 17 (40.4) |
Chi-square: 3.802, degrees of freedom: 3, P=0.2836, Amongst the patients who worsened, the number of non-comorbid patients who were unvaccinated were more than the number of comorbid patients who were unvaccinated, however this result was not statistically significant. It suggests that there was no statistically significant association between vaccination status and outcome in this study population.
| Comorbidity | Infusion interval 1–5 days (%) |
Infusion interval 6–10 days (%) |
Total (20) (%) |
|---|---|---|---|
| Non-comorbid | 5 (25) | 8 (40) | 13 (65) |
| Comorbid | 5 (25) | 2 (10) | 7 (35) |
Mid-P exact: 0.1018, Amongst the patients who worsened, the number of non-comorbid patients who were administered the drug after 5 days (i.e. between 6-10 days) of symptom onset were more than the number of comorbid patients who were administered the drug in the same interval, however this result was not statistically significant. It suggests that there was no statistically significant association between infusion interval and outcome in this study population.
Limitations of the study
This is just an observational study. Efficacy of the drug could not be assessed by this study. Ideally, a case–control study needs to be undertaken to assess efficacy.
CONCLUSION
In this study, none of the 42 patients developed any reaction to casirivimab-imdevimab. About 52.3% of the patients improved after the administration of the cocktail along with a standard care treatment. About 33.3% of comorbid patients improved, while 47.6% of patients continued to worsen after receiving the antibody cocktail, but there was no mortality in this group of patients. Further, clinical outcome studies need to be undertaken to assess efficacy of the drug in the Indian population.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Risk factors for COVID-19 severity and fatality: A structured literature review. Infection. 2020;49:15-28.
- [CrossRef] [PubMed] [Google Scholar]
- Comprehensive Guidelines for Management of COVID-19 Patients. 2021. Available from: https://www.dghs.gov.in/writereaddata/news/202105270436027770348comprehensiveguidelinesformanagementofcovid-1927may2021dteghs.pdf [Last accessed on 2023 Mar 07]
- [Google Scholar]
- REGN-COV2, a neutralizing antibody cocktail, in outpatients with covid-19. N Engl J Med. 2021;384:238-51.
- [CrossRef] [PubMed] [Google Scholar]
- Fact Sheet for Health Care Providers Emergency Use Authorization (Eua) of Regen-Cov® (Casirivimab and Imdevimab) REGENERON. Available from: https://www.regeneron.com/downloads/treatment-covid19-eua-fact-sheet-for-hcp.pdf [Last accessed on 2022 Feb 05]
- [Google Scholar]
- Casirivimab-imdevimab in Covid 19-early Indian experience. Indian J Tuberc 2021
- [CrossRef] [PubMed] [Google Scholar]
- Revised Guidelines for Home Isolation of mild/asymptomatic COVID-19 Cases [PDF file] 2021. Available from: https://www.mohfw.gov.in/pdf/revisedhomeisolationguidelines05012022.pdf
- [Google Scholar]
- Unmasking hypoxia in COVID 19-six minute walk test. J Assoc Physicians India. 2020;68:50-1.
- [Google Scholar]




