
Translate this page into:
Alterations in heart rate variability before and after percutaneous coronary intervention in patients with ischaemic heart disease

*Corresponding author: Vinutha Shankar MS, Department of Physiology, Sri Devaraj Urs Academy of Higher Education and Research, Kolar, Karnataka, India. vinutha.shankar@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Seetharam SP, Shankar VMS, Udupa K, Reddy N, Raveesha A. Alterations in heart rate variability before and after percutaneous coronary intervention in patients with ischaemic heart disease. Indian J Physiol Pharmacol 2022;66:188-95.
Abstract
Objectives:
Heart rate variability (HRV) is the beat-to-beat variation of heart rate and an important non-invasive tool to study the cardiac autonomic nervous system activity. Ischaemic heart disease (IHD) patients are often considered to have a state of sympathetic predominance. Elimination of myocardial ischaemia with percutaneous coronary intervention (PCI) could restore autonomic balance. Hence, this study aimed to evaluate HRV measures, after successful revascularisation among IHD patients.
Materials and Methods:
A total of 145 male IHD patients planned for coronary angiography were recruited. Fifteen minutes of electrocardiogram recording was done. Short-term HRV analyses of all the patients were acquired and time-domain indices (standard deviation of normal-to-normal intervals [SDNN], root-mean-squared differences of successive R-R intervals [rMSSD]) and frequency-domain indices (low-frequency [LF] power, high-frequency [HF] power and total power [TP]) were analysed. Before and after PCI, all measurements were made.
Results:
This study included 145 male IHD patients with the mean age of 54.57 ± 10.81 years. There was a significant decrease in SDNN, rMSSD, LF, HF and TP whereas increase in LF/HF ratio following revascularisation. These changes in measures of neurocardiac regulation correlated with risk factors and medication on regression analysis.
Conclusion:
Increase in LF/HF ratio with the decrease in SDNN, rMSSD, LF, HF and TP in patients with IHD who underwent coronary intervention infers changed cardiac autonomic balance with this surgical procedure. These measures could be potentially used as prognostic measures in the future studies.
Keywords
Ischaemic heart disease
Cardiac autonomic function
Myocardial infarction
Heart rate variability

INTRODUCTION
Heart rate variability (HRV) is the beat-to-beat difference in heart rate and it occurs as a result of active influence of the sympathetic and parasympathetic nerve fibres on the sinoatrial node.[1,2] It is a vital non-invasive tool, an indirect marker to quantify cardiac autonomic nervous system activity.[1-4] Higher HRV indicates good compliance with environmental and physiological requirements while lower HRV shows the probable occurrence of cardiovascular morbidity threats and risks.
Coronary artery disease patients tend to have increased sympathetic activity as ischemic event induces this enhanced sympathetic function.[5-8] Elimination of myocardial ischemia could bring back the autonomic balance state to normal.[6-9] Only a few studies looked at the role of HRV analyses in the restoration of cardiac autonomic balance in patients with ischaemic heart disease (IHD).[5,9] Accordingly, in a study by Gomes et al.[5] among stable angina patients, by a combination of methods involving muscle sympathetic nerve activity (MSNA), neurochemical (plasma catecholamine levels) and HRV (time-domain and frequency-domain indices), sympathetic nervous system activity was measured before and 1-month post-percutaneous coronary intervention (PCI). They observed that there was a decline in sympathetic activity with a significant reduction in MSNA and a low frequency/ high frequency (LF/HF) ratio associated with a reduction in plasma norepinephrine levels after PCI. On the other hand, Abrootan et al.[9] the study analysed short-term HRV (only time-domain indices) among stable angina patients and found that there was a significant difference only between the pre-and post-PCI standard deviation of normal-to-normal intervals (SDNN) HRV variable. Furthermore, the autonomic behaviour of males and females are different[10] and could be influenced by different phases of the menstrual cycle. In this regard, we aimed to evaluate the state of cardiac autonomic function with PCI among male IHD patients using HRV measures.
MATERIALS AND METHODS
Study setting
This observational study was conducted at Coronary Care Unit (CCU), R. L. Jalappa Hospital, in association with the Department of Physiology, attached to Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
Ethical consideration
The study was approved by the Central Ethics Committee (CEC No. SDUAHER/KLR/R and I/91/2021-22 dated 9 March 2021). Written informed consent was obtained from all the study participants.
Sample size
The sample size was calculated[9] using nMaster 2.0 software and was estimated with 0.8 as power and <0.05 as a significant P-value [Figure 1].
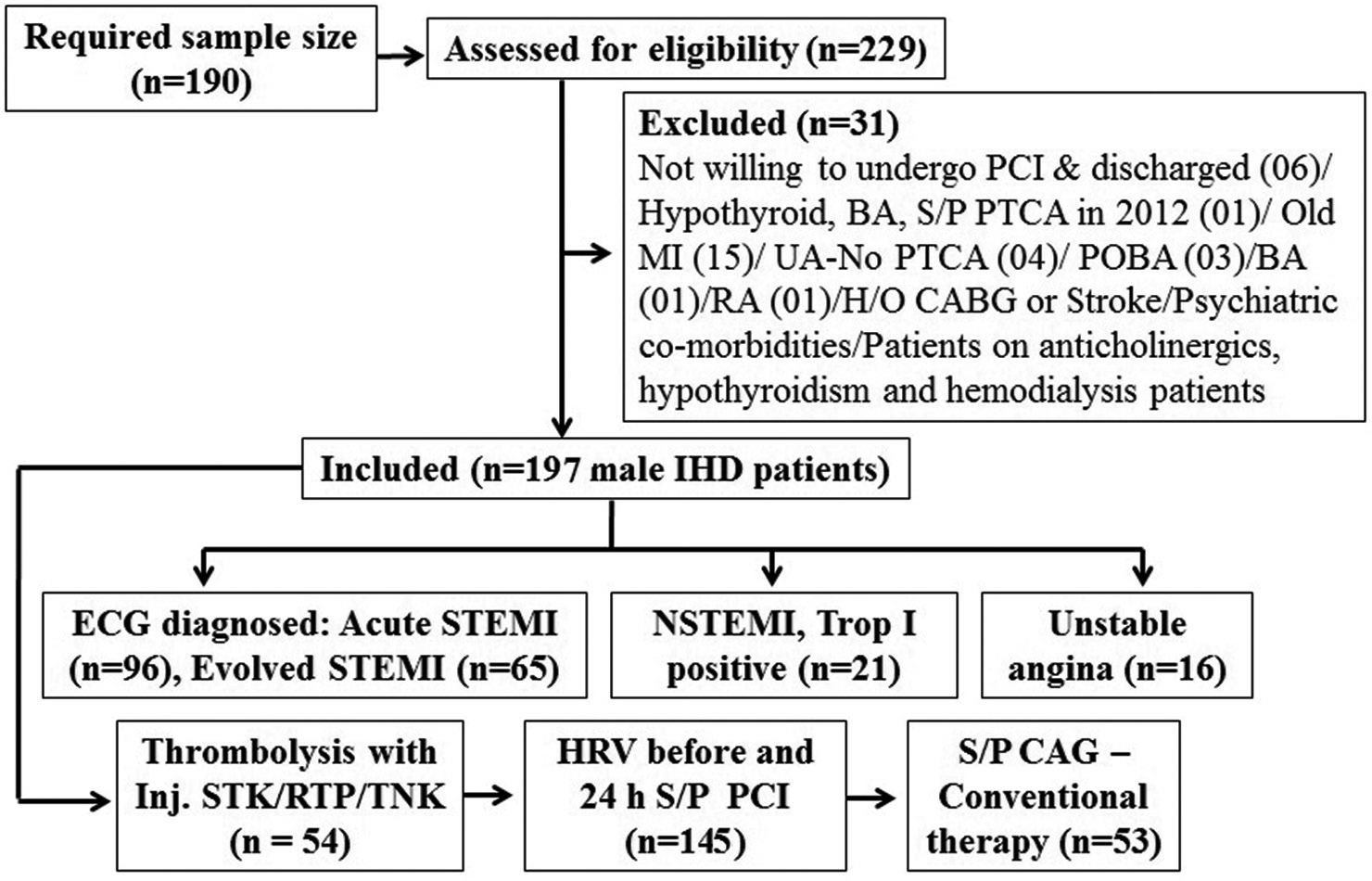
- Study flow chart before and after percutaneous coronary intervention (PCI). BA: Bronchial asthma, S/P PTCA: Status post-percutaneous transluminal coronary intervention, MI: Myocardial infarction, UA: Unstable angina, POBA: Percutaneous old balloon angioplasty, RA: Rheumatoid arthritis, CABG: Coronary artery bypass graft, IHD: Ischaemic heart disease, STEMI: ST elevation myocardial infarction, NSTEMI: Non-ST elevation myocardial infarction, STK: Streptokinase, RTP: Reteplase, TNK: Tenecteplase, CAG: Coronary angiogram.
Study population
Type of study
This was a prospective cohort study.
Study design
The selection of study participants was done as per systematic random sampling.
Inclusion criteria
One hundred and forty-five IHD[11] (Killip class I to IV)[12] male patients with first acute myocardial infarction (ST-segment elevation myocardial infarction/STEMI, n = 72 and nonST-elevation myocardial infarction (NSTEMI), n = 18); evolved MI (n = 44); unstable angina (n = 11) admitted at CCU, between March and November 2021 were included in the study. Among them, 39.31% (n = 57) had anterior wall myocardial infarction. Furthermore, 93.05% of the patients had a history of angina and 8.33% had dyspnoea. Patients who smoked cigarette/beedi,[13,14] tobacco chewers and alcoholics[15] were also included in the study. Among the included, 28.47% of them were diabetics and 38.19% of them were hypertensive. Patients on diuretics (56.25%)[16] were also allowed to participate in the present study. All the subjects underwent reperfusion therapy using PCI. All the recruited participants were COVID-19 negative.
Exclusion criteria
Patients with chronic stable angina, effort/exertional angina, old myocardial infarction, previous PCI, previous bypass surgery and patients who had a stroke were excluded from the study. Self-reported various psychiatric comorbidities or patients who were on anticholinergics were excluded from the study. Patients with atrial fibrillation, ventricular tachycardia, frequent ectopics or pacemaker that could interfere with precise HRV analysis were excluded from this study. Self-reported dysautonomias such as Parkinson’s disease, multiple sclerosis, rheumatoid arthritis, systemic lupus erythematosus, psoriasis, amyloidosis and malignancies were also excluded from the study. In addition, haemodialysis patients were also not included in the study.
Study design
We prospectively studied consecutive patients admitted to our CCU with a first myocardial infarction, who underwent PCI (primary/elective) of the culprit coronary artery within 6–24 h of symptom onset in the case of acute STEMI patients, with 70% within 6 h of symptom onset. NSTEMI patients underwent elective PCI within 24 h of symptom onset. Patients were also included if they underwent earlier failed thrombolysis (rescue PCI), as indicated by the persistent ST-segment elevation. Symptom-to-door timing in case of evolved MI/unstable angina patients was 2 h to a month’s duration.
Acute STEMI was diagnosed in patients presenting with typical chest pain lasting ≥30 min and associated with ST-segment elevation ≥0.1 mV in ≥2 contiguous leads on the admission electrocardiogram (ECG). NSTEMI was diagnosed in patients presenting with typical chest pain lasting ≥30 min and associated with ST-segment depression ≥0.1 mV in ≥2 contiguous leads on the admission ECG; T wave inversion, with the cardiac biomarker troponin-I positive. Evolved MI was diagnosed with the symptom onset from a few hours to 1 week; from hyperacute T waves to ST elevation, then T wave inversion in ≥2 contiguous leads on the admission ECG. Unstable angina was diagnosed with the on and off symptom onset from a few hours to 1 month.
The clinical and laboratory parameters recorded for each patient were as follows: Age, body mass index (BMI), cardiovascular risk factors, site of infarction, symptom-to-door timing, culprit coronary artery vessels/number of diseased coronary artery vessels (defined as the presence of diameter stenosis >50%), thrombolytic therapy before PCI, thrombolysis in myocardial infarction (TIMI) coronary flow grade post-PCI, peak values of markers of myocardial necrosis (creatine kinase-myocardial band [CK-MB] or troponin I) and drug therapy. Left ventricular ejection fraction was measured on admission and 24 h post-PCI by 2-D echocardiography based on the Simpson method.
Thirty-one patients (22%) received thrombolytic therapy with streptokinase (15000 UI/h) or reteplase or tenecteplase. In addition, 79 patients (54.50%) underwent primary PCI within 12–24 h from the chest pain onset, 65 patients went through elective PCI (45%), rescue PCI was done in an IHD patient and was associated with procedural success in all subjects.
HRV measurements
All patients underwent Lead-II ECG recording on admission and 24-h post-PCI to obtain both time domain and frequency domain short-term HRV indices. Fifteen minutes of ECG recording was done using 4-Channel PowerLab15T for all the recruited participants. Consequently, power spectral density is obtained by Fast Fourier transform analysis. Accordingly, both the time and the frequency domain linear HRV parameters were analysed using Lab Chart 7 data analysis software and the MLS310 HRV module developed by AD Instruments, Australia.
Time domain HRV indices assessed in this study included SDNN and root-mean-square differences of successive N-N intervals (rMSSD). In the frequency domain, the amplitudes of RR interval oscillations in the frequency range of LF (LF: 0.04– 0.15 Hz), HF (HF: 0.15–0.40 Hz), low frequency in normalised units (LFnu) and high frequency in normalised units (HFnu) were obtained and LF/HF ratio was calculated. LFnu and HFnu were calculated based on the formulae: LF norm = LF/ (TP-VLF)*100 => LF/(LF + HF)*100 and HF norm = HF/(TPVLF)*100 => HF/(LF + HF)*100, respectively.
Methodology
On admission to CCU, a thorough history, and clinical examinations were carried out for all the study participants. Weight in kg (using the KRUPS weighing scale, New Delhi, India) was documented. Systolic and diastolic blood pressures were also measured.
Twelve-lead ECG recording was done in all study subjects to assess the changes in the ST segment to confirm myocardial infarction (STEMI). However, limitations and factors known to alter ECG recordings will be given due weightage throughout the study.
HRV measurements were based on the non-exposure of study subjects to permissible bright light (400–500 nm) or noise. Room temperature was maintained during the study at 22–26°C. During the HRV measurement, study subjects were asked to be in the supine position, close their eyes, awake and calm. Throughout the study, the study subjects were requested to be as normal as possible and not to control their breathing intentionally or for experimentation. For all the recruited subjects, HRV measurements were done at CCU on admission and 24-h post PCI. Throughout the procedure, quality was not compromised. All the parameters were statistically analysed.
Statistical analysis
All quantitative data were presented as mean ± SD. Time domain and frequency domain HRV parameters were tested for Gaussian distribution using Kolmogorov–Smirnov test. The data did not follow normal distribution, and hence, the differences in the mean values of HRV before and after PCI were compared using the non-parametric Wilcoxon-signed rank test. Spearman’s correlation coefficient between age, BMI and baseline HRV variables was used to find out the relationship between anthropometric and physical parameters with causation of disease and alteration of autonomic function. Spearman’s correlations were performed to know the effect of confounding variables such as age, BMI on heart rate. Multivariate tests were done to model the effect of confounding variables such as smoking, alcohol consumption, tobacco chewing, Killip class, diabetes mellitus (DM), hypertension (HTN) and medications on baseline HRV indices. The level of statistical significance was set at P < 0.05. IBM Statistical Package for the Social Sciences version 22.0 software (Chicago, IL) for windows was used for all data analysis.
RESULTS
The study population consisted of 145 male IHD patients with a mean age of 54.57 ± 10.81 years. The baseline characteristics of the study population are given in [Table 1]. Included patients were on antiplatelets (100%), anticoagulants (97%), beta-blockers (36%), diuretics (56%), oral hypoglycaemic agents/insulin (29%), statins (98%), calcium channel blockers (6.25%), angiotensin receptor blockers (4.86%) and ACE inhibitors (2%). Baseline laboratory data are presented in [Table 2].
| Characteristics | Mean±SD |
|---|---|
| Mean age (years) | 54.57±10.81 |
| BMI (kg/m2) | 25.11±4.01 |
| Killip classification (n=134) | |
| Class I | 124 |
| Class II | 1 |
| Class III | 6 |
| Class IV | 3 |
| Clinical Data | |
| Systolic blood pressure (mm Hg) | 128.84±24.04 |
| Diastolic blood pressure (mm Hg) | 80.21±11.02 |
| Basal heart rate (bpm) | 82.24±12.99 |
| Left ventricular ejection fraction (%) | 48.72±9.40 |
| Cardiovascular risk factors | |
| Diabetes mellitus, n(%) | 42 (28.97) |
| Hypertension, n(%) | 55 (37.93) |
| Smoking, n(%) | 43 (29.66) |
| Alcohol consumption, n(%) | 26 (17.93) |
| Tobacco chewing, n(%) | 6 (4.14) |
| Site of Infarction (n=116) | |
| Anterior, n(%) | 56 (48.28) |
| Coronary angiography and PCI data (n) | |
| Primary PCI | 79 |
| Rescue PCI | 1 |
| Elective PCI | 65 |
| Culprit coronary vessels with significant lesions (>50%) | |
| Single vessel disease | 78 |
| Double vessel disease | 33 |
| Triple vessel disease | 16 |
| TIMI flow Grade III (post-PCI) | 145 |
TIMI: Thrombolysis in myocardial infarction
| Before PCI (Mean±SD) | |
|---|---|
| Haemoglobin (gm/dL) | 14.40±2.03 |
| Serum creatinine (mg/dL) | 0.88±0.30 |
| Blood urea nitrogen (mg/dL) | 26.39±12.35 |
| Sodium (mEq/L) | 135.98±16.51 |
| Potassium (mEq/L) | 4.22±0.61 |
| Chloride (mEq/L) | 99.44±9.60 |
| Glucose random blood sugar (mg/dl) | 157.4±64.18 |
| Myocardial necrosis markers (n) | |
| Troponin I (ng/ml), (n=43) | Positive (35) |
| Creatine Kinase-MB (ng/ml), (n=33) | Abnormal (22) |
Time domain and frequency-domain linear HRV indices were measured before and after coronary intervention [Table 3]. There was a statistically significant decrease between pre- and post-PCI SDNN (P = 0.000), rMSSD (P = 0.000), TP (P = 0.000), LF (P = 0.000) and HF (P = 0.000) HRV indices. In addition, HFnu HRV index decreased significantly post-PCI with P = 0.020. Furthermore, the average heart rate between pre- and post-PCI increased significantly with P = 0.003. Hence, the rise in heart rate post-PCI is consistent with enhanced sympathetic activity and a decrease in parasympathetic activity.
| HRV parameters | Before PCI | After PCI | Z-value | P-value |
|---|---|---|---|---|
| Time-Domain parameters | ||||
| SDNN (ms) | 44.82 | 29.64 | –5.197b | 0.000** |
| rMSSD (ms) | 40.61 | 24.41 | –4.240b | 0.000** |
| Frequency-domain parameters | ||||
| TP (ms2) | 1718.68 | 766.83 | –5.070b | 0.000** |
| LF (ms2) | 281.86 | 108.32 | –5.570b | 0.000** |
| HF (ms2) | 293.72 | 86.67 | –4.437b | 0.000** |
| LFnu | 38.87 | 35.23 | –0.134b | 0.894NS |
| HFnu | 29.50 | 25.23 | –2.321b | 0.020* |
| LF/HF ratio | 1.08 | 1.39 | –0.918b | 0.358NS |
| Heart rate (bpm) | 81.69 | 84.92 | –2.989b | 0.003* |
Values expressed as median, *Significance P<0.05, ** P<0.01. NS: Not significant, b: Exact statistic, SDNN: Standard deviation of NN intervals, rMSSD: Square root of the mean squared differences of successive NN intervals, TP: Total power, LF: Low-frequency, HF: High-frequency, LFnu: Low-frequency normalised unit, HF-nu: High-frequency normalised unit
Spearman’s correlation analysis
Spearman’s rank correlation analysis between time domain and frequency domain HRV measures and confounding variables such as age and BMI was performed. Resulting no statistically significant correlation between time domain and frequency domain measures of HRV and age except HFnu (r = 0.245; P = 0.003) and LF/HF ratio (r = –0.245; P = 0.009) frequency domain HRV indices. Besides, there was no statistically significant correlation between time and frequency domain measures of HRV and BMI. Furthermore, there was a significant negative correlation between age and heart rate with r = –0.22 and P = 0.007 [Table 4].
| HRV variables | Spearman’s rho | Age (years) | BMI (kg/m2) |
|---|---|---|---|
| SDNN (ms) | Correlation coefficient | 0.081 | –0.023 |
| P-value | 0.333NS | 0.784NS | |
| rMSSD (ms) | Correlation coefficient | 0.079 | –0.059 |
| P-value | 0.342NS | 0.481NS | |
| TP (ms2) | Correlation coefficient | 0.067 | –0.016 |
| P-value | 0.424NS | 0.848NS | |
| LF (ms2) | Correlation coefficient | –0.024 | –0.016 |
| P-value | 0.774NS | 0.853NS | |
| HF (ms2) | Correlation coefficient | 0.102 | –0.077 |
| P-value | 0.223NS | 0.359NS | |
| LFnu | Correlation coefficient | –0.155 | 0.087 |
| P-value | 0.062NS | 0.299NS | |
| HFnu | Correlation coefficient | 0.245 | –0.126 |
| P-value | 0.003** | 0.132NS | |
| LF/HF ratio | Correlation coefficient | –0.217 | 0.107 |
| P-value | 0.009** | 0.200NS | |
| Heart rate (bpm) | Correlation coefficient | –0.222 | 0.067 |
| P-value | 0.007** | 0.423NS |
*Significance P<0.05, ** P<0.01; NS: Not significant; BMI: Body mass index
Multivariate tests
Multivariate regression analyses were performed to know the possible role of smoking, tobacco chewing, alcohol consumption and Killip class on HRV parameters [Table 5]. Predictors such as smoking, tobacco chewing, alcohol consumption and Killip class had no significant association with the HRV parameters.
| Effect | Value | F | Hypothesis df | Error df | Sig. |
|---|---|---|---|---|---|
| Intercept | 0.264 | 43.154b | 8.000 | 124.000 | 0.000 |
| Smoking | 0.962 | 0.616b | 8.000 | 124.000 | 0.763NS |
| Tobacco Chewing | 0.988 | 0.183b | 8.000 | 124.000 | 0.993NS |
| Alcohol consumption | 0.960 | 0.644b | 8.000 | 124.000 | 0.739NS |
| Killip classification | 0.899 | 0.421 | 32.000 | 458.885 | 0.998NS |
| Intercept | 0.045 | 355.565b | 8.000 | 134.000 | 0.000 |
| Diabetes mellitus | 0.921 | 1.444b | 8.000 | 134.000 | 0.184NS |
| Hypertension | 0.943 | 1.008b | 8.000 | 134.000 | 0.433NS |
*Significance P<0.05; NS: Not significant, bExact statistic
Multivariable regression analyses were done to know whether DM and HTN have got any effect on HRV parameters [Table 5]. Both DM and HTN had no significant association with any of the HRV indices. Whereas with the corrected model, rMSSD (P = 0.026), LFnu (P = 0.011), HFnu (P = 0.033) and LF/HF ratio (P = 0.007) HRV indices seem to be affected by the risk factors.
Multivariate tests were run to know whether various drugs have got any effect on HRV parameters [Table 6]. Resultantly, no significant association of drugs with any of the HRV indices was found except diuretics with P = 0.012. In addition, with the corrected model also, rMSSD (P = 0.033) HRV index seems to be affected by the diuretics.
| Effect | Value | F | Hypothesis df | Error df | Sig. |
|---|---|---|---|---|---|
| Intercept | 0.227 | 52.415b | 8.000 | 123.000 | 0.000 |
| On antianginal drugs | 0.963 | 0.589b | 8.000 | 123.000 | 0.786NS |
| On anticoagulants | 0.986 | 0.225b | 8.000 | 123.000 | 0.986NS |
| On thrombolytics | 0.883 | 2.028b | 8.000 | 123.000 | 0.048NS |
| On beta blockers | 0.988 | 0.188b | 8.000 | 123.000 | 0.992NS |
| On diuretics | 0.857 | 2.573b | 8.000 | 123.000 | 0.012* |
*Significance P<0.05, NS: Not significant, bExact statistic
DISCUSSION
The major finding of the present study is the significant increase in LF/HF ratio with the significant decrease in SDNN, rMSSD, LF, HF and TP after successful revascularisation. We observed that there was an overall decrease in HRV indicated by the significant increase in LF/HF ratio post- PCI. In addition, the significant decrease in SDNN, rMSSD, LF, HF and TP suggested a decrease in parasympathetic activity in patients with IHD following revascularisation. These findings could be explained by the heightened state of sympathetic hyperactivity prompted due to acute stress or anxiety of surgical procedure, which might have prevented HRV increase even after successful revascularisation. The increase of SDNN post-PCI was significantly higher in subjects without pre-procedural anxiety compared with those with anxiety.[6] In the present study, during pre-PCI ECG recordings, angina/dyspnoea/anxiety persisted in a few patients. In another study by Delewi et al.,[17] anxiety levels were measured using the self-reported visual analogue scale and observed that the pre-procedural anxiety scores obtained were the highest. In addition, in their study, other elements associated with greater levels of anxiety were age <65 years, lesser education and an acute primary PCI. Hence, we need to dissect the influence of anxiety or stress on neurocardiac autonomic regulation by measuring before and after the procedure. Furthermore, the rise in average heart rate is consistent with enhanced sympathetic activity and a decrease in parasympathetic activity post-PCI.
Another study by Wennerblom et al.[18] included 48 patients with angina and 41 age-matched healthy controls, 24 h Holter recordings were done before coronary intervention, 1 and 6 months post-revascularisation. The authors observed normal SDNN, SDANN and LF/HF ratio with the significant reduction in rMSSD, pNN50, total power (TP), LF and HF peak among angina patients compared to controls. Hence, it was shown that successful revascularisation would cause only a partial stabilisation of vagal tone indicating that ischaemia could be one of the mechanisms of the reduction in HRV among chronic coronary artery disease patients.
Gomes et al.[5] found that in patients with myocardial ischaemia, cardiac revascularisation reduced central sympathetic activity. Two-channel Holter was used in their study to calculate the mean LF/HF ratio as a frequency domain HRV index during a 10-min period recording and presented that the ratio reduced after revascularisation. Besides, in a study by Abrootan et al.,[9] a significant increase in SDNN was found after successful revascularisation in patients with stable angina pectoris. Another study by Aydinlar et al.[19] found that the HF, rMSSD and SDNN components of HRV were increased significantly after PCI. In their study, to calculate short-term HRV parameters before and after balloon inflation, the Holter monitoring system was used. In the present study, we used Limb Lead-II ECG monitoring to measure short-term HRV indices and calculated those parameters during a 5-min period.
Pivatelli et al.[20] found that parasympathetic activity had been reduced in patients with coronary artery disease and that some HRV indices (HF in absolute units, root mean square differences of successive N-N intervals [rMSSD] and several pairs of adjacent N-N intervals differing by more than 50 ms [NN50]) could be used for prognostic purposes in patients with chronic stable angina. Miyase et al.[21] disclosed that calculating the LF/HF ratio immediately before coronary angiography may predict the coronary artery disease presence. It has been revealed that a significant decrease in HRV parameters is a predictor of mortality in the case of coronary artery disease. Forslund et al.[22] found that frequency domain (using 24-h Holter monitoring) HRV indices had vital prognostic value concerning the risk of cardiovascular death in chronic stable angina. It was also shown that irrespective of other comorbidities, a low HRV was the strongest predictor of angiographic coronary disease and was valuable clinically as a risk predictor in patients with sinus rhythm.
In a study by Zang,[23] it was revealed that TP decreased consistently from the age groups 10+ to 80+ years (P < 0.001). Both the low-frequency and high-frequency HRV indices decreased (P < 0.05) as age increased. The older age group had steadily lower HRV than younger people. In the present study, age had a statistically significant negative correlation with heart rate (r = –0.24; P = 0.004). In addition, age had a significant association with the HFnu and LF/HF ratio HRV indices.
Bassi et al.[24] found that patients with T2DM and HTN exhibited lower values of mean R-R intervals when compared with patients who had only T2DM. Accordingly, HTN has got a negative influence on the cardiac autonomic function in DM. However, the present study results revealed that both DM and HTN had no significant association with any of the HRV measures. Review by Benichou et al.[25] included 25 case-control studies; which consisted of 1356 patients with T2DM and 1576 healthy controls. T2DM patients had significantly lower R-R intervals, lower SDNN, lower rMSSD, lower pNN50, lower TP, lower LF and lower HF. Several HRV parameters were found to be associated with levels of blood glucose and HbA1c, along with time from the diagnosis of T2DM. The overall decrease in the HRV of T2DM patients could be explained by the detrimental effects of varied glucose metabolism on HRV, leading to cardiac autonomic neuropathy. In the present study, 28.47% were diabetic and 38.2% of the IHD patients were hypertensive. We analysed HRV excluding those with DM within IHD patients. Accordingly, there was a statistically significant difference between pre-PCI and post-PCI HRV indices [SDNN (P = 0.000); rMSSD (P = 0.000); TP (P = 0.001); LF (P = 0.002) and HF (P = 0.005)]. Hence, it was found that T2DM was associated with an overall decrease in the HRV, due to the toxic effects of altered glucose metabolism on HRV, causing cardiac autonomic neuropathy.
Investigating the effects of cardiac medications on HRV, a study by Sandrone et al.[26] observed that beta-blocker-induced bradycardia was associated with a significant increase in the average 24 h values of TP and of the HFnu parameter, whereas the LF parameter was critically reduced. Therefore, it could be said that, with the β-blockade, a decrease in signs of sympathetic activation and the rise in vagal tone explain the valuable effects of β-blockers after myocardial infarction. Patients who were on β-blockers in the present study did not have any effect on HRV indices. On the other hand, a study by Tomiyama et al.[16] investigated the effects of short-acting (furosemide 40–60 mg/day) and long-acting (azosemide 60–90 mg/day) loop diuretics on HRV in 19 patients with chronic congestive heart failure. Analysis of time-domain and frequency-domain HRV indices was accomplished using 24 h Holter monitoring. The SDNN and the rMSSD were significantly reduced with furosemide when compared to azosemide. Hence, furosemide has a greater influence on HRV than azosemide, in patients with mild-to-moderate chronic congestive heart failure. Similar results were obtained in the present study with the lasilactone diuretic (spironolactone, a potassium-sparing diuretic and furosemide, a loop-diuretic) had a statistically significant association with HRV (P = 0.014).
Limitations
The present study was a single-centre cohort study. Hence, multi-centric large-scale randomised trials are essential for further validation of the usefulness of HRV as one of the prognostic evaluators for IHD. Further follow-up assessment may yield better results and validate the study findings in gauging the prognostic/predictive value of HRV measures in patients with IHD. In addition, pre-procedural anxiety was not assessed in the present study, which would have enlightened us about the decrease in HRV indices post-PCI.
CONCLUSION
An increase in LF/HF ratio with the decrease in SDNN, rMSSD, LF, HF and TP in patients with IHD who underwent coronary intervention infers changed cardiac autonomic balance with this surgical procedure. These measures could be potentially used as prognostic measures in future studies.
Enhanced pre-procedural information regarding coronary intervention or pharmacological approaches could reduce anxiety in patients undergoing revascularisation for IHD. Furthermore, investigating the potential introduction of yoga and exercise training could be studied to comprehend the modulation of cardiac autonomic balance in these patients in future directions.
Declaration of patient consent
Institutional review board (IRB) permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Heart rate variability standards of measurement physiological interpretation, and clinical use task force of the European society of cardiology and the North American society of pacing and electrophysiology. Eur Heart J. 1996;17:354-81.
- [CrossRef] [Google Scholar]
- Clinical Guide to Cardiac Autonomic Tests. Dordrecht: Kluwer Academic Publishers; Dordrecht: Kluwer Academic Publishers; 1998
- [CrossRef] [Google Scholar]
- Measuring heart rate variability in patients admitted with ST-elevation myocardial infarction for the prediction of subsequent cardiovascular events: A systematic review. Medicina (Kaunas). 2021;57:1021.
- [CrossRef] [PubMed] [Google Scholar]
- Improving myocardial perfusion by percutaneous coronary intervention reduces central sympathetic activity in stable angina. Clin Cardiol. 2009;33:E16-21.
- [CrossRef] [PubMed] [Google Scholar]
- Increased heart rate variability following elective percutaneous coronary intervention in patients with stable coronary artery disease and preprocedural anxiety. Cardiol Res Pract. 2019;2019:3696825.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of coronary revascularization by elective percutaneous coronary intervention on cardiac autonomic modulation assessed by heart rate variability: A single-center prospective cohort study. Am J Cardiovasc Dis. 2021;11:164-75.
- [Google Scholar]
- Short-term effect of percutaneous coronary intervention on heart rate variability in patients with coronary artery disease. Entropy (Basel). 2021;23:540.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in heart rate variability parameters after elective percutaneous coronary intervention. J Tehran Heart Cent. 2015;10:80-4.
- [Google Scholar]
- Gender differences in the activity of the autonomic nervous systems of healthy and hypertensive patients in Russia. J Appl Biotechnol Bioeng. 2017;3:459-63.
- [CrossRef] [Google Scholar]
- Ischemic Heart Diseases I20-I25. Available from: https://www.icd10data.com/ICD10CM/Codes/I00-I99/I20-I25 [Last accessed on 2022 Aug 25]
- [Google Scholar]
- Available from: https://www.healio.com/cardiology/learn-theheart/cardiology-review/topic-reviews/killip-classification [Last accessed on 2022 Aug 25]
- U.S. Department of Health and Human Services. The Health Consequences of Smoking-50 Years of Progress: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. 2014.
- [Google Scholar]
- Low cigarette consumption and risk of coronary heart disease and stroke: meta-analysis of 141 cohort studies in 55 study reports. BMJ. 2018;360:j5855.
- [CrossRef] [PubMed] [Google Scholar]
- Chronic heavy drinking and ischaemic heart disease: A systematic review and meta-analysis. Open Heart. 2014;1:e000135.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of short-acting and long-acting loop diuretics on heart rate variability in patients with chronic compensated congestive heart failure. Am Heart J March. 1999;137:543-8.
- [CrossRef] [Google Scholar]
- Anxiety levels of patients undergoing coronary procedures in the catheterization laboratory. Int J Cardiol. 2017;228:926-30.
- [CrossRef] [PubMed] [Google Scholar]
- Reduced heart rate variability in ischemic heart disease is only partially caused by ischemia an HRV study before and after PTCA. Cardiology. 2000;94:146-51.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of percutaneous transluminal coronary angioplasty on QT dispersion and heart rate variability parameters. Cardiovasc J Afr. 2009;20:240-4.
- [Google Scholar]
- Sensitivity, specificity and predictive values of linear and nonlinear indices of heart rate variability in stable angina patients. Int Arch Med. 2012;5:31.
- [CrossRef] [PubMed] [Google Scholar]
- The ratio of low-frequency to high-frequency in ambulatory electrocardiographic monitoring immediately before coronary angiography as a predictor of the presence of coronary artery disease. J Clin Med Res. 2014;6:36-43.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic implications of autonomic function assessed by analyses of catecholamines and heart rate variability in stable angina pectoris. Heart. 2002;87:415-22.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of age and sex on heart rate variability in healthy subjects. J Manipulative Physiol Ther. 2007;30:374-9.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of coexistence hypertension and Type II diabetes on heart rate variability and cardiorespiratory fitness. Arq Bras Cardiol. 2018;111:64-72.
- [CrossRef] [PubMed] [Google Scholar]
- Heart rate variability in Type 2 diabetes mellitus: A systematic review and meta-analysis. PLoS One. 2018;13:e0195166.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of beta blockers (atenolol or metoprolol) on heart rate variability after acute myocardial infarction. Am J Cardiol. 1994;74:340-5.
- [CrossRef] [Google Scholar]




