
Translate this page into:
An integrated simulation-based early clinical exposure module in cardiovascular physiology
*Corresponding author: Rashmi Jain, Department of Ophthalmology, Yenepoya Medical College, Yenepoya (Deemed to be University), Deralakatte, Mangalore - 575 018, Karnataka, India. drrashjain@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dutt RA, Jain R, Bangera S. An integrated simulation-based early clinical exposure module in cardiovascular physiology. Indian J Physiol Pharmacol 2020:64(2):147-54.
Abstract
Objectives:
A good conceptual understanding of physiology is very important to build a strong foundation for medical students. It is a daunting job for teachers to emphasise the clinical relevance of basic science subjects as exposure to patients invariably starts after these subjects have been taught. With the introduction of early clinical exposure in the newly revised Indian undergraduate medical curriculum, this problem can be addressed to a certain extent. We developed an integrated simulation module for teaching cardiovascular physiology to pre-clinical students as a part of early clinical exposure.
Materials and Methods:
We included 145 medical students of a Private Medical College of a Deemed to be University in Mangalore, Karnataka, India. The teaching module covered the topics of cardiovascular physiology such as functional anatomy, cardiac cycle, normal electrocardiogram (ECG), arrhythmia, arterial pulse examination, heart sounds and hands-on cardiovascular examination using a variety of simulators. The assessment was done by pre-test and post-test. A retro-pre questionnaire was used to assess their self-perceived knowledge gain and level of clinical skills. Feedback on overall experience was collected from the participants.
Results:
The student feedback showed that learning experience was life-like (98.6%), effective, innovative and enjoyable (99.3%) and making the overall experience of learning easier (95.2%). It also improved participation, communication (93.8%), clinical skills and a better understanding of patient care (99.3%). The results of the retro- pre questionnaire to assess their self-perceived knowledge gain (95%) and level of clinical skills (96%) were highly satisfactory. The assessment of knowledge domain showed 100% of the students achieved pass percentage (>50%) with significant difference among pre- and post-test scores. Faculty (100%) opined that simulation-based teaching resulted in effected learning.
Conclusions:
The use of simulation-based teaching in cardiovascular physiology as part of early clinical exposure leads to enhanced learning and clinical application. This will stimulate interest in subject and promote better learning.
Keywords
Cardiovascular
Manikins
Medical education
Simulation training

INTRODUCTION
Physiology is a foundation for health professional students which require a lucid understanding of the concept. It is a core and mandatory subject for students of medical, dental, nursing and allied health sciences, which is considered as a difficult yet interesting at multiple levels by the students.[1] At present, physiology is being taught to undergraduate pre-clinical medical students in India using didactic lectures, small group tutorials, web-based e-learning and project-based methods.[2] The purpose of these different teaching-learning methods is to make the students understand the clinical application of physiology in interactive and innovative style.
Till 2018, early clinical exposure was not a norm in most Indian medical colleges, which has now become an integral component of a new competency-based medical education curriculum. Lack of direct patient encounter and knowledge regarding actual health-care setting, it is a daunting task for educators to find a bridge to fill this lacuna.[3] The traditional model of teaching is being supplemented with different innovative techniques, to link the pre-clinical and clinical topics. This has not been effectively implemented everywhere due to multiple constraints at various levels.[2] There is a need to find ways to make undergraduate physiology learning experience more interesting, stimulating and enthusiastic with ‘in action’ student engagement using simulators. The use of mannequins, especially High Fidelity patient simulators promotes active and experiential learning.
Simulations are defined as ‘approximations to the reality that require trainees to react to problems or conditions as they would under genuine circumstances.’[4] The simulation- based learning has been accepted as an established method for honing clinical competencies of medical, dental, nursing and other health sciences students worldwide.[5] Training in a stress-free and no-risk environment enhances students’ emergency response. This results in a confident health professional.[6] ‘Shows how’ level of Miller’s assessment framework requires the learner to demonstrate the integration of knowledge and skills into successful clinical performance. Simulation-based assessment tests a student at this level and has attained an important educational value by profoundly enhancing the learning environment for undergraduate students.[7]
Due to all these benefits, high fidelity human patient simulators have expanded their horizons into high school and college levels too. Here, it aids the students in problem- solving and critical thinking.[8] This mode of training is equipment demanding, needs sophisticated technology and trained simulation educators.
Simulation-based teaching has been effectively adapted in clinical specialties such as anaesthesia, emergency medicine, intensive care medicine, surgery, obstetrics, paediatrics, ophthalmology and radiology.[9] The simulators can be used to teach basic anatomy and physiology integrating with clinical aspects, in close to real-life settings. However, effectively using the same for teaching the basic science concepts to undergraduate pre-clinical students is not yet an established practice. The reasons could be due to lack of pre-existing framework and adequately trained simulation educators.
Gordon et al. and Harris et al. have shown that human patient simulators when used for undergraduate medical students to teach physiology, improves their learning process and helps in the retention of concepts.[10,11] The feedback obtained from the students who have undergone this process showed a deep satisfaction as shown in Harvard Summer Preclinical Institute by Gordon et al.[12]
In a study by Agha et al. to evaluate medical students’ satisfaction with simulation-based learning strategy at College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia, showed significant difference between the satisfaction scores among genders as female students’ preference for simulation-based teaching was more compared to their counterparts.[13]
There are limited studies regarding the implementation and learning outcomes of simulation-based physiology teaching as part of early clinical exposure using High Fidelity simulators in the Indian setup. The needs assessment of students showed that they preferred simulation-based learning. Hence, we aimed to develop an integrated simulation-based module with assessment blueprint for teaching cardiovascular physiology to undergraduate pre-clinical medical students as part of early clinical exposure. We also evaluated the training process to assess whether it is beneficial for understanding the concepts and acquiring clinical skills. We studied any gender-wise preference in simulation-based learning among the students.
MATERIALS AND METHODS
This module was developed and implemented for 1st-year undergraduate pre-clinical medical students (n = 145) of Yenepoya Medical College of one cohort for teaching cardiovascular physiology. The simulation training was conducted at Advanced Comprehensive Clinical Training and Simulation Centre (ACTS-YEN), Yenepoya (Deemed to be University), Mangalore, Karnataka, India. The Institutional Ethics committee approval was obtained for the study.
The needs assessment was done in consultation with the stakeholders including the student fraternity before module development. The students were explained about different teaching-learning strategies which included large group interactive teaching, small group teaching, E-learning, simulation-based and project-based learning. These teaching-learning methods were discussed with the students highlighting the advantages and limitations of each. This was then followed by written feedback. The feedback was collected to determine the order of their preference for learning cardiovascular system. The analysis showed that 95% of them opted for simulation-based learning as their topmost preference.
Development of simulation-based module
Brainstorming sessions were conducted with the teaching faculty from physiology, department of internal medicine and medical education unit. The module hence created consisted of the goals and learning objectives for each simulation sessions which were defined with learning outcomes and assessment methods [Figure 1].
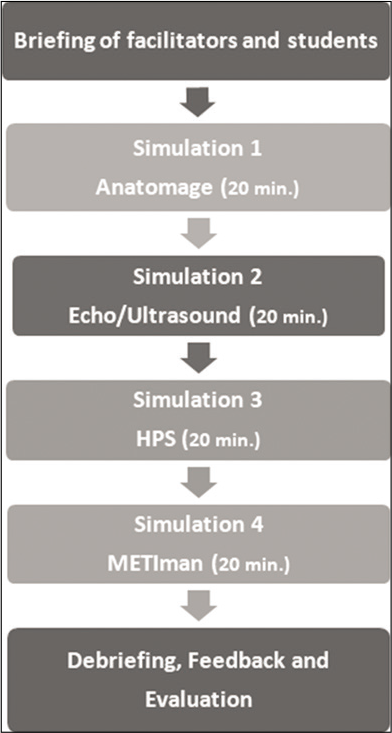
- Steps involved in the implementation of the simulation module.
A plan was prepared for the briefing, scenarios, simulations, debriefing and evaluation. A team of simulation educators was selected and trained for the implementation of plan. A pilot session was conducted on a group of 2nd-year students and their feedback was collected. Based on these results, few changes were made to the plan.
Students were introduced to the topics of cardiac cycle and electrocardiogram (ECG) by large group interactive method. An electronic pre-test that comprised 15 multiple choice questions from the topics of cardiovascular physiology was administered to the students.
The actual process at the simulation centre
The students (n = 145) were giving a briefing about the learning outcomes, the working of simulators and facilities available at the simulation centre for 20 min. This included hands-on experience with mannequins, techniques, scenarios and procedural skills. The students were then divided into five groups of 30 each having a team leader and timekeeper for smooth transition between the sessions. Students were rotated in an orderly pre-planned fashion across the four simulation stations. Each station was of 20 min duration. [Figure 1] Each station had one simulation educator to facilitate learning. A brief description of each station is as follows.
Station 1
This was a Virtual Dissection Table by Anatomage Inc. (California, USA, 2016.) This table provides a visualisation of human anatomy with high-level accuracy and dissectible in 3D format. Using this, students were shown the structural anatomy and relations of heart and major blood vessels. Students were encouraged to individually identify the structural relations of the heart.
Station 2
This station had an ultrasound simulator-Vimedix (CAE Healthcare, Canada, 2016). The simulation educator explained the flow of blood through chambers of heart, cardiac cycle with pressure and volume changes. The production of the heart sounds was also explained.
Station 3
A clinical case scenario of ventricular fibrillation admitted in an intensive care unit was created on a High Fidelity Human Patient Simulator (HPS) (CAE Healthcare, Canada, 2014). The students were briefed regarding the working of HPS and the usage of various equipment, drugs and monitors connected to it. The learning objective of this station was to teach the electrical conduction system of the heart, its relation to ECG, normal ECG and identifying the abnormalities of rhythm in ECG.
Station 4
This station aimed at teaching clinical examination of the cardiovascular system using METIman (Medical Education Technologies Inc, CAE Healthcare, Canada, 2014), which is a High Fidelity patient simulator. With this simulator, arterial pulse examination including all peripheral pulses, heart sounds, apex beat, cardiac borders examination and breath sounds was demonstrated. The students were asked to practice individually on this mannequin.
The student doubts were addressed throughout the interactive sessions as well as at the end of the entire process.
Debriefing, feedback and evaluation
After the students completed the entire process, they were administered a questionnaire regarding their learning experience at the simulation centre [Table 1] and feedback was sought at each station [Figure 2]. An electronic post- test was conducted to evaluate the change in knowledge. A retro-pre questionnaire, based on the Dreyfus Model of skill acquisition was administered. They were asked to rate their self-perceived change in understanding of concepts in cardiovascular physiology. They also rated their confidence levels in clinical skills before and after the simulation training. The feedback from faculty involved in the planning and implementation of this integrated teaching module was also collected [Figure 3].
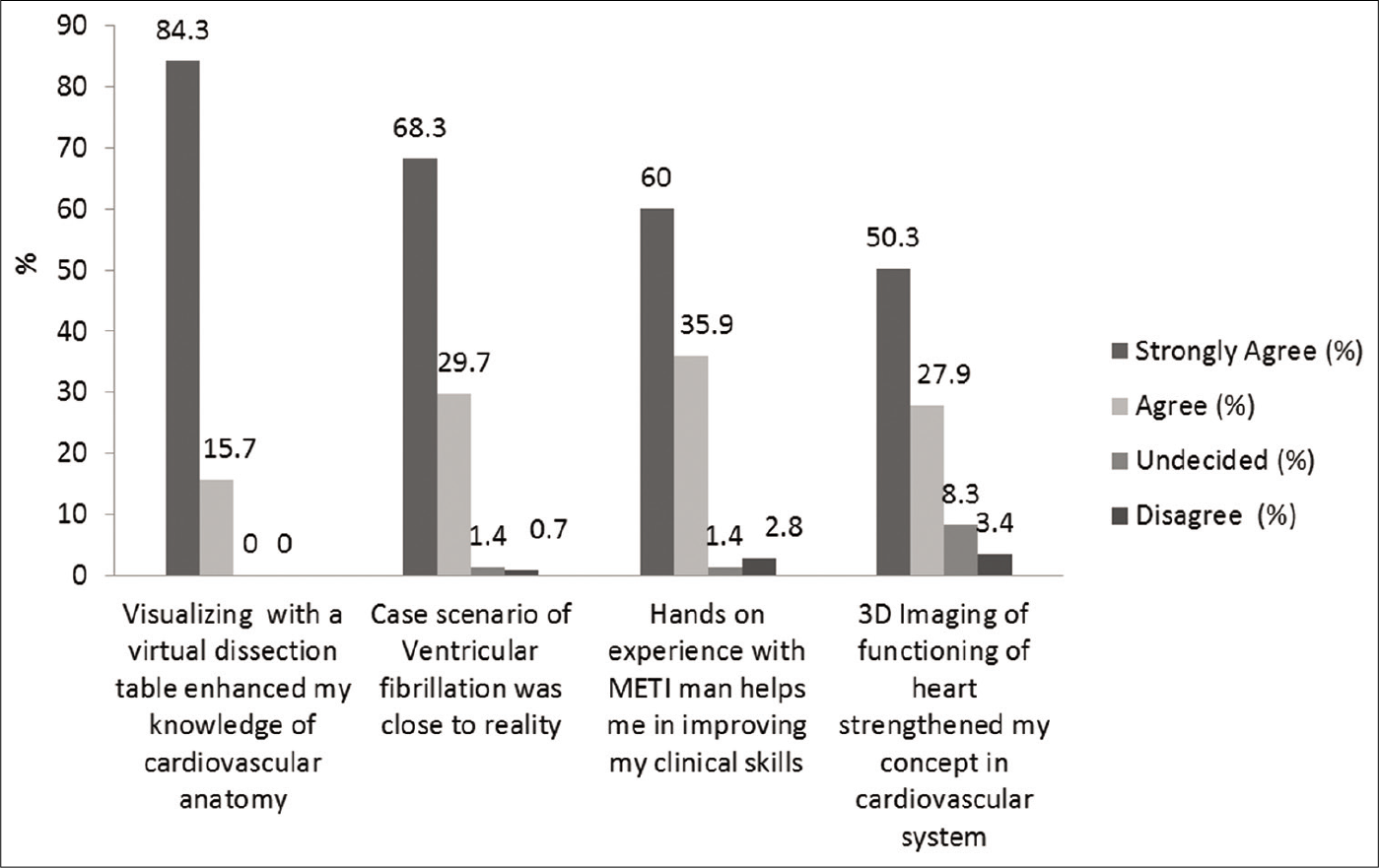
- Student feedback on the utility of simulation stations.
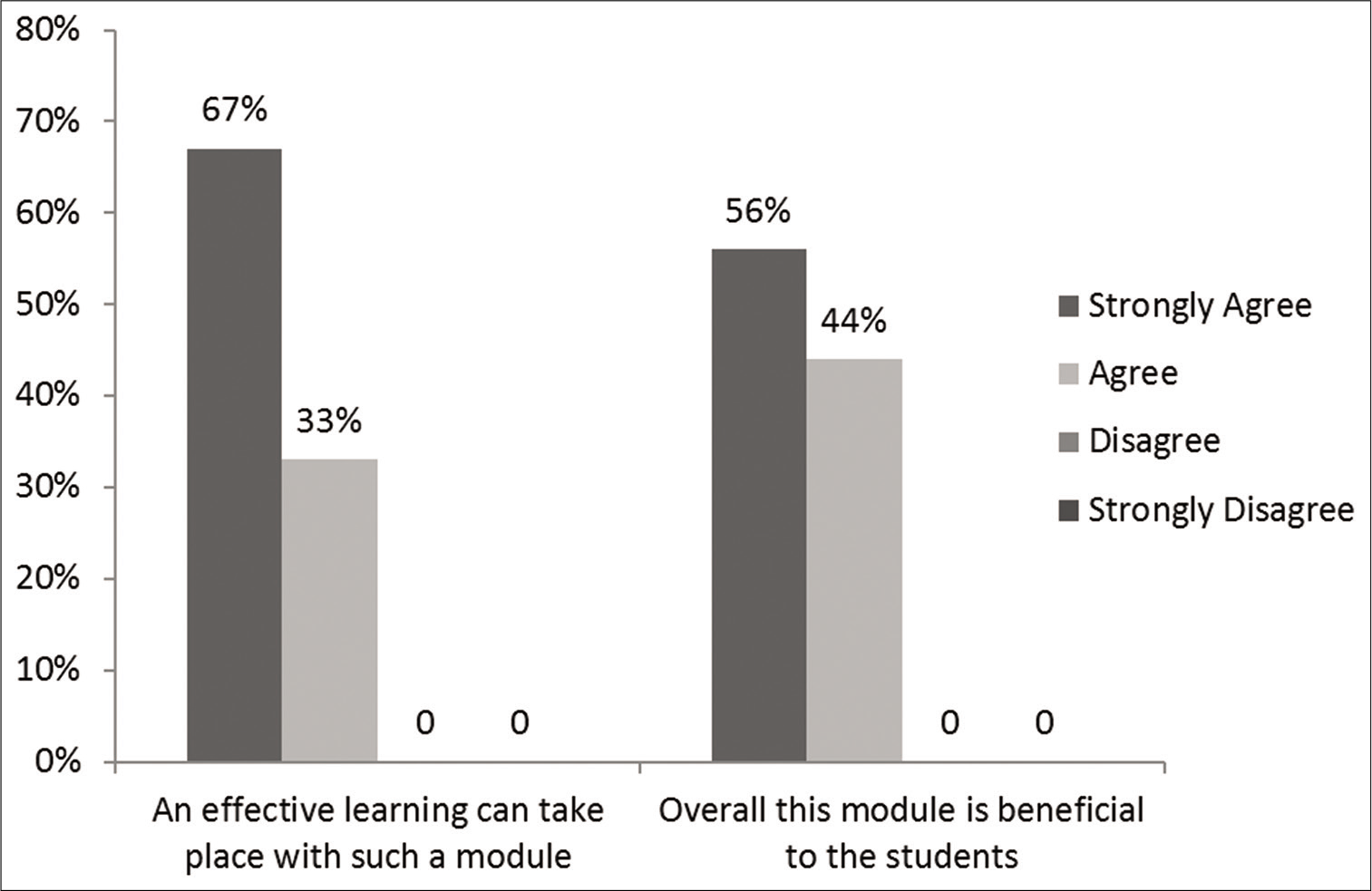
- Faculty feedback on simulation-based teaching module (n=14).
| Questions | Strongly agree (%) | Agree (%) | Undecided (%) | Disagree (%) | Strongly disagree (%) |
|---|---|---|---|---|---|
| The training session resembled a real-life situation | 90 (62.1) | 53 (36.6) | 1 (0.7) | 1 (0.7) | 0 |
| Cardiovascular physiology concepts were easily learnt by simulation | 85 (58.6) | 53 (36.6) | 4 (2.8) | 3 (2.1) | 0 |
| Initial briefing helped me to learn better | 64 (44.1) | 76 (52.4) | 4 (2.8) | 0 | 1 (0.7) |
| I feel that simulation is essential in understanding diseases of cardiovascular system | 99 (68.3) | 44 (30.3) | 1 (0.7) | 1 (0.7) | 0 |
| Small group teaching with simulation is a better way of teaching learning | 105 (72.4) | 34 (23.4) | 4 (2.8) | 1 (0.7) | 1 (0.7) |
| Integrating anatomy with physiology facilitated my learning | 93 (64.1) | 50 (34.5) | 2 (1.4) | 0 | 0 |
| Small group teaching with simulation keeps us to be more involved in learning | 96 (66.2) | 40 (27.6) | 8 (5.5) | 1 (0.7) | 0 |
| Simulation training can improve patient safety and quality of healthcare | 95 (65.5) | 49 (33.8) | 0 | 1 (0.7) | 0 |
| Simulation can improve effective participation and communication | 87 (60) | 49 (33.8) | 6 (4.1) | 2 (1.4) | 1 (0.7) |
| Simulation in healthcare has advantages for training and gaining the competencies for students | 81 (55.9) | 61 (42.1) | 3 (2.1) | 0 | 0 |
| The training session was enjoyable | 113 (77.9) | 31 (21.4) | 0 | 1 (0.7) | 0 |
| I would prefer to have more of simulation-based teaching in addition to traditional teaching methods in learning | 124 (85.5) | 21 (14.5) | 0 | 0 | 0 |
(The top value is the number of students and in parentheses is the % of the total).
The feedback from students and faculty along with assessment scores were analysed statistically using the Chi-square test, with P < 0.05 taken as statistically significant (Statistical software IBM SPSS Version 23). MS Excel was used for data entry and generation of graphs. Yengage, an online learning portal of Yenepoya (Deemed to be University), which is created on the ILIAS platform was used for assessment and feedback.
RESULTS
The student feedback on simulation-based learning shows that the cardiovascular physiology concepts and clinical skills were better understood in a near real-life situation (98.7%). Integrating anatomy, physiology with internal medicine in small groups was well appreciated. It made learning enjoyable for them (89.3%). The students’ feedback was highly satisfactory for all the simulation stations. The majority of the students agreed that simulation sessions at every station addressed their need to integrate basic cardiovascular concepts with clinical applications effectively [Figure 2].
They also felt that it helped them in improving their communication skills (93.8%) and would prefer to have more simulation based teaching [Table 1].
On analysing for gender difference in learning preference, it was noted that the female students preferred hands-on experience with METIman in improving clinical skills and 3D imaging of functioning of heart when compared with the male students which were statistically significant [Table 2].
| Questions | Strongly agree | Agree | Undecided | Disagree | Strongly disagree | P-value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M (n=65) F (n=80) | M | F | M | F | M | F | M | F | M | F | |
| Hands on experience with METIman helps me in improving my clinical skills | 33 (51) | 54 (67) | 26 (40) | 26 (33) | 2 (3) | 4 (6) | - | - | - | 0.02 | |
| 3D Imaging of functioning of heart strengthened my concept in cardiovascular system | 26 (40) | 47 (59) | 30 (46) | 25 (31) | 8 (12) | 4 (5) | 1 (1) | 4 (5) | - | - | 0.04 |
(The top value is the number of students and in parentheses is the % of the total for the significant items only)
The faculty feedback revealed that 67% of the faculty strongly agreed and 37% agreed that effective learning takes place with a simulation-based integrated module. Similarly, 56% of the faculty strongly agreed and 44% agreed that this module is beneficial for student learning [Figure 3].
[Table 3] shows responses of the students to the retro-pre questionnaire to assess their self-perceived knowledge gain and level of clinical skills before and after the integrated teaching session. Most of the students advanced from beginner to proficient in acquiring these skills (95% and 96%, respectively). Their summative assessment scores to test their actual gain in knowledge showed that all the students achieved the minimum pass percentage as desired.
| Retro-pre questionnaire | Results | |
|---|---|---|
| Physiology concepts in cardiovascular system | 95% advanced from beginner to proficient | |
| Confidence levels in clinical skills | 96% advanced from beginner to proficient | |
| Electronic test results | ||
| Number of students who took the tests (n) | 145 | P<0.0001 |
| Average pre-test score | 10.41/15 | |
| Average post-test score | 13.36/15 | |
| Number of students who scored above 75% in post-test | 91 (63%) | |
| Number of students who scored 65–75% in post-test | 54 (37%) |
DISCUSSION
The process of development and evaluation of an integrated simulation-based learning module as part of early clinical exposure to teach cardiovascular system physiology concepts to 1st-year undergraduate pre-clinical medical students was studied. Meticulous blueprinting the topics, using multiple modalities and integrating physiology knowledge with clinical application has helped in improving the students’ academic and clinical performance. Proper understanding of physiology concepts in undergraduate teaching is the foundation basis for most disciplines/subjects in medical field. Learning clinical skills are one of the competencies expected to be attained by 1st-year undergraduate as per Medical Council of India’s new competency-based medical education curriculum.[14] Hence, this module has helped students in improving both knowledge and clinical skills.
The stress-free environment has contributed to an enjoyable learning experience. Before the introduction of the new curriculum in the absence of early clinical exposure, real-life simulation sessions in undergraduate physiology helped the students to link theory to clinical aspects of cardiovascular system. The small group training sessions have the advantage of more interaction among the students which enhance their communication levels among themselves and the teachers. An integrated approach to teaching using simulations was beneficial to the students which gave them a comprehensive picture of learning medicine instead of compartmentalising anatomy and physiology as individual units.[11]
The virtual dissection table has the advantage of performing layer by layer dissection and visualising structures in various views in three dimensions. This has helped the students in integrating structural anatomy with functional physiology in our study. Similar results were found in a study conducted on 1st-year medical students in Canada who perceived enhanced learning with virtual dissection. This proved that virtual dissection augmented cadaveric dissection in medical education.[15]
The students could visualise the chambers of heart, valves, blood flow inside the heart, contraction of cardiac muscle and valvular movements using 3D imaging. Bell FE 3rd et al. have studied the effect of using ultrasound simulation to teach cardiac physiology to 1st-year medical students at the University Of South Carolina School Of Medicine. The post-test scores showed improvement in knowledge and the feedback from them was very positive as a valuable teaching tool for learning.[16] According to educational psychologists, the instructional methods that emphasise guidance with practical approaches are more effective than minimally guided approaches.[17] The use of trained simulation educators to facilitate learning at station could also be a factor contributing to improved student satisfaction.
The students were able to appreciate the intensive care unit set up which was created to monitor and manage a case of ventricular fibrillation in the simulation sessions using HPS in our study. They understood the diagnosis of the disease using symptoms and electrocardiogram. The students in small groups were able to feel the emergency situation, the behaviour of the staff handling the simulated patient and how he was treated. The web-based and mannequin simulations for learning shock physiology were conducted for 40 students at University of Central Florida, Orlando and Florida, where students rated the mannequin simulation as more effective in teaching shock and its treatment aspects which are in accordance with our observed results.[18] To teach undergraduate pre-clinical medical students in physiology, High Fidelity simulators have been used in the previous studies to teach basic neuroscience concepts,[19] respiratory physiology,[20] hypovolemic shock[21] and renal failure[22] only at selected centres worldwide. By appropriate design of the scenarios, proper training with simulators, drafting specific learning objectives with an assessment component, the desired goal can be attained effectively.[23]
METIman has an advantage of examination of precordium, arterial pulses, peripheral pulses, respiratory sounds and heart sound on a simulator without any discomfort to the subject or a patient. Females preferred hands-on experience with METIman in improving clinical skills while examining cardiovascular system. This might be due to overcoming the inhibition of practicing examination on male colleagues, which is observed in the Indian setup. This gender-wise difference of student feedback on simulation-based learning with different simulators is similar to the studies done in Saudi Arabia.[13]
The previous studies using HPS and METIman at different places have revealed that student satisfaction and learning are maximum with simulation-based teaching.[24] It has resulted in better understanding of the physiological aspects which are directly linked with the pathological conditions which are mimicked using Low and High Fidelity simulators.[25] In addition to the traditional didactic lectures, small group teaching, an integrated simulation-based teaching which includes hands-on experience for real-life-like situations increases the retention of learned knowledge as it involves the concept of ‘learning by doing.’ It has been proposed that in all health specialties, patient simulation with virtual reality blended with e-learning will enable medical students to learn effectively in a greater way.[26]
We found most of the students felt that their self-perceived knowledge and level of clinical skills have increased along with 100% of the students achieving a minimum pass percentage in their assessment. Similar results were seen in a study conducted in Chennai, India with simulation-based teaching. Their results showed that this mode of teaching had a significant impact on the knowledge and skills of both the gender group.[27]
The students in our study enjoyed the whole process of simulation-based learning as it is different from the traditional model of curricular transactions. All the students would like to have more simulation-based teaching programs for other topics in physiology. This innovative method of student teaching-learning strategy is being implemented across the health-care institutions worldwide.[28] In spite of such innovations in teaching-learning strategies, most of the medical colleges in India are following traditional teaching- learning methods.[29] The High Fidelity simulators with a functional physiological model are yet to be effectively utilised and incorporated into our curriculum. The reason for not using simulators may be related to the high operational cost involved. Simulation-based teaching integrated with other traditional methods in basic science education can definitely improve student learning.[30] Simulation-based learning implemented in curriculum helps the students to effectively practice patient care away from the bedside, enhance their theoretical and clinical skill knowledge.[31]
We are in the process of developing simulation-based integrated modules in other topics to cater to the needs of the student community. Such module needs to be incorporated into health medical curriculum to produce competent health-care professionals.
CONCLUSION
An integrated approach to early clinical exposure using simulation is useful for understanding the complex physiological mechanisms of the cardiovascular system. With sufficient infrastructure and clear planning, the learning process of the students can be made more effective and interesting.
Acknowledgments
PSG-FAIMER Regional Institute, Coimbatore, India, for mentoring in this project. Advanced Comprehensive Clinical Training and Simulation Centre – ACTS YEN, Yenepoya (Deemed to be University), Mangalore, for logistic support. Dr. Giuseppe A Marraro, Prof. Emeritus, the University of Milan for training in simulation and providing evaluation assistance in this project. Mr. Rajesh Karkera, Deputy Director, Department of Informational Technology, Yenepoya (Deemed to be University), Mangalore for IT assistance. in Online feedback and evaluation. Teaching faculty of Yenepoya Medical College, Mangalore, for facilitating the simulation sessions.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- What makes physiology hard for students to learn? Results of a faculty survey. Adv Physiol Educ. 2007;31:34-40.
- [CrossRef] [PubMed] [Google Scholar]
- Pedagogical effectiveness of innovative teaching methods initiated at the department of physiology, government medical college, Chandigarh. Adv Physiol Educ. 2004;28:51-8.
- [CrossRef] [PubMed] [Google Scholar]
- Sometimes we do get it right? Early clinical contact is a rewarding experience. Educ Health. 2004;17:42-52.
- [CrossRef] [PubMed] [Google Scholar]
- Simulation in professional competence assessment: Basic considerations In: Tekian A, McGuire CH, McGaghie WC, eds. Innovative Simulations for Assessing Professional Competence. Chicago: Department of Medical Education, University of Illinois at Chicago; 1999. p. :7-22.
- [Google Scholar]
- Simulation-based learning: Just like the real thing. J Emerg Trauma Shock. 2010;3:348-52.
- [CrossRef] [PubMed] [Google Scholar]
- Are simulated patients effective in facilitating development of clinical competence for healthcare students? A scoping review. Adv Simul. 2016;1:6.
- [CrossRef] [PubMed] [Google Scholar]
- The assessment of clinical skills competence performance. Acad Med. 1990;65:63-7.
- [CrossRef] [PubMed] [Google Scholar]
- Using immersive healthcare simulation for physiology education: Initial experience in high school, college, and graduate school curricula. Adv Physiol Educ. 2011;35:252-59.
- [CrossRef] [PubMed] [Google Scholar]
- Simulation based medical education: An opportunity to learn from errors. Med Teach. 2005;27:193-9.
- [CrossRef] [PubMed] [Google Scholar]
- Bringing good teaching cases to life: A simulator-based medical education service. Acad Med. 2004;79:23-7.
- [CrossRef] [PubMed] [Google Scholar]
- Using a high-fidelity patient simulator with first-year medical students to facilitate learning of cardiovascular function curves. Adv Physiol Educ. 2012;36:213-9.
- [CrossRef] [PubMed] [Google Scholar]
- Perspective: Fostering biomedical literacy among America's youth: How medical simulation reshapes the strategy. Acad Med. 2008;83:521-3.
- [CrossRef] [PubMed] [Google Scholar]
- Satisfaction of medical students with simulation based learning. Saudi Med J. 2015;36:731-6.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://www.mciindia.org/CMS/information-desk/for-colleges/ug-curriculum [Last accessed on 2019 Aug 13]
- Integrated virtual and cadaveric dissection laboratories enhance first year medical students' anatomy experience: A pilot study. BMC Med Educ. 2019;366:1-6.
- [CrossRef] [PubMed] [Google Scholar]
- Using ultrasound to teach medical students cardiac physiology. Adv Physiol Educ. 2015;39:392-96.
- [CrossRef] [PubMed] [Google Scholar]
- Why minimal guidance during instruction does not work: An analysis of the failure of constructivist, discovery, problem-based, experiential, and inquiry-based teaching. Educ Psych. 2006;41:75-86.
- [CrossRef] [Google Scholar]
- Enhancing learning through optimal sequencing of web-based and manikin simulators to teach shock physiology in the medical curriculum. Adv Physiol Educ. 2011;35:402-7.
- [CrossRef] [PubMed] [Google Scholar]
- Large group high-fidelity simulation enhances medical student learning. Med Teach. 2009;31:206-10.
- [CrossRef] [PubMed] [Google Scholar]
- A simulator-based respiratory physiology workshop. Acad Med. 1996;71:526-7.
- [CrossRef] [PubMed] [Google Scholar]
- Teaching respiratory physiology: Clinical correlation with a patient simulator. J Clin Monit Comput. 2000;16:465-70.
- [CrossRef] [Google Scholar]
- Human patient simulation to teach medical physiology concepts: A model evolved during eight years. J Teach Learn Technol. 2013;2:79-89.
- [Google Scholar]
- Medical student attitudes toward kidney physiology and nephrology: A qualitative study. Ren Fail. 2016;38:1683-93.
- [CrossRef] [PubMed] [Google Scholar]
- Progress in the utilization of high-fidelity simulation in basic science education. Adv Physiol Educ. 2016;40:143-44.
- [CrossRef] [PubMed] [Google Scholar]
- Teaching residents the two-challenge rule: A simulation-based approach to improve education and patient safety. Simul Healthc. 2009;4:84-91.
- [CrossRef] [PubMed] [Google Scholar]
- See one, do one, teach one: Advanced technology in medical education. Acad Emerg Med. 2004;11:1149-54.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of simulation-based teaching of applied physiology of the cardiovascular system on the undergraduate medical student. Natl J Physiol Pharm Pharmacol. 2017;7:323-7.
- [CrossRef] [Google Scholar]
- Current trends and future implications in the developing role of clinical skills centres. Med Teach. 2001;23:483-89.
- [CrossRef] [PubMed] [Google Scholar]
- Change in learning preferences from pre-clinical to clinical course of undergraduate medical students-a longitudinal study. Indian J Physiol Pharmacol. 2017;61:65-9.
- [Google Scholar]
- Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Acad Med. 2011;86:706-11.
- [CrossRef] [PubMed] [Google Scholar]
- Simulation-based medical education: Using best practices and curriculum mapping to maximise educational benefits in the context of shift toward competency-based medical education. Arch Med Health Sci. 2017;5:9-15.
- [Google Scholar]




