
Translate this page into:
Breaking the monotony: Exploring the approach of game-based learning in students’ understanding of antimicrobials and antimicrobial resistance

*Corresponding author: Vidya Mahalmani, Department of Pharmacology, Jawaharlal Nehru Medical College, KAHER, Belagavi, Karnataka, India. vidyapattanshetti88@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mahalmani V, Angadi NB, Pattanshetti S. Breaking the monotony: Exploring the approach of game-based learning in students’ understanding of antimicrobials and antimicrobial resistance. Indian J Physiol Pharmacol. 2025;69:107-11. doi: 10.25259/IJPP_100_2024
Abstract
Objectives:
The primary objective of the study was to evaluate students’ understanding of the subject through GBL compared to traditional didactic lectures. The secondary objective was to evaluate the perception and feedback of students regarding the GBL.
Materials and Methods:
After didactic lectures over a month, a pre-test was conducted for the whole batch. Following this, GBL was conducted for the entire batch. A virtual board numbered from 1 to 100 was prepared and played with virtual dice and game pieces. The board had colour-coded antibiotics (blue in colour), microorganisms (yellow in colour) and mutated organisms (red in colour). The player had to move either ahead or back based on the block he landed on. A set of questions were prepared, which varied from lower-order questions to higher-order thinking. The lower order questions included drug of choice, mechanism of action, uses and adverse effects, WhatsApp emoji-based questions, match the following, word puzzle and image-based questions. The higher-order questions included case scenarios with irrational antibiotic prescriptions and drug-resistant cases. The students had to analyse the treatment given and comment upon it. Furthermore, questions related to antimicrobial stewardship were asked so that students were able to understand the importance of the antimicrobial stewardship programme as well. After every question, a brief discussion about the condition and different options was done so that the students understand the subject and learn to critically evaluate the antimicrobials prescribed. After this activity, a post-test was conducted.
Results:
On comparing the pre-test (14.46 ± 0.29) and post-test scores (17.55 ± 0.26*), it was noted that students performed better in the post-test (*P < 0.0001). Students’ feedback regarding GBL revealed that this innovative teaching learning method was enjoyable. It helped them to interact and understand the concepts better.
Conclusion:
Therefore, virtual board game on antimicrobials is easy, affordable and can be implemented at every institution, especially in developing countries where there is rampant usage of antimicrobials.
Keywords
Antimicrobial resistance
Antimicrobials
Game-based learning
Global burden

INTRODUCTION
Antimicrobial resistance (AMR), being one of the most challenging global health issues, poses a significant threat to mankind. AMR is more prevalent in developing countries where there is a lack of proper healthcare systems and access to basic sanitation and hygiene. Tackling AMR is a multidisciplinary approach as it involves the active participation of major stakeholders such as doctors, nurses, pharmacists and other healthcare workers. The last few decades have witnessed the emergence of multidrug-resistant and extensively drug-resistant bacterial strains, making most of the antimicrobials obsolete.
Medical undergraduates require adequate knowledge about various antimicrobials, their mechanism of action, uses, adverse effects and AMR as these students shall be medical practitioners in future. Good prescribing skills enable rational and judicial prescribing, improve patient compliance and reduce healthcare-associated costs.[1] A study by Okedo-Alex et al. revealed that poor prescribing skills among medical practitioners are due to inadequate training during their undergraduate.[2] However, one of the major obstacles in medical teaching is the vast amount of knowledge students have to acquire in a limited duration of time. Although antimicrobials and AMR have been a part of the medical curriculum, medical students have an attitude of indifference towards these topics as they were unable to correlate between the organisms, pathology and treatment effectively. The reason could be due to the lack of alignment between the topics taught across Microbiology, Pathology and Pharmacology in the traditional curriculum. Fortunately, with the implementation of Competency-Based Medical Education (CBME), this limitation is overcome and the students can now correlate well and understand better. CBME has also included a separate competency for 2nd-year medical undergraduates that highlights the importance of AMR and antimicrobial stewardship programme (AMSP). However, imparting traditional didactic lectures on antimicrobials and antibiotic resistance would be boring and cumbersome as well.
Existing literature portrays that games could be a better way to engage students in joint learning.[3] Games have proven to enhance learning by stimulating players’ interest and motivation.[4] A study conducted by Aboalshamat et al. amongst students showed that game-based learning (GBL) using an antimicrobials board game significantly improved AMR knowledge, with better retention when compared to a traditional lecture.[5] GBL enhances the active participation of students and promotes their critical thinking and problem-solving skills.[6] This is a novel study, where the virtual board game was designed by the authors. We modified the traditional snake and ladder game. The ladder was not used here to remove bias due to luck and wanted students to move further only by answering correctly. Therefore, the proposed game ‘Drugs versus Bugs’ was planned to integrate various aspects of pharmacological knowledge and critical thinking and intended to be a supplemental tool for the formal learning of the subject.
MATERIALS AND METHODS
About the game
Initially, traditional didactic lectures related to antimicrobials were scheduled across a month. The students were informed in prior about the conduct of GBL on completion of the topics. Informed consent and institutional ethics committee approval were taken.
The game ‘Drugs versus Bugs’ consists of a virtual board and is played with virtual dice and pawns. Figure 1 depicts the image of a virtual board. The board consists of 100 squares (blocks) numbered from 1 to 100. A square might have ‘a pill’ or ‘a microbe’ or ‘a mutated microorganism’. The board contains 100 numbered squares, out of which 50 random blocks contain antibiotics (blue or white in colour), 13 contain microorganisms (yellow in colour), and 5 contain mutated organisms (red in colour).
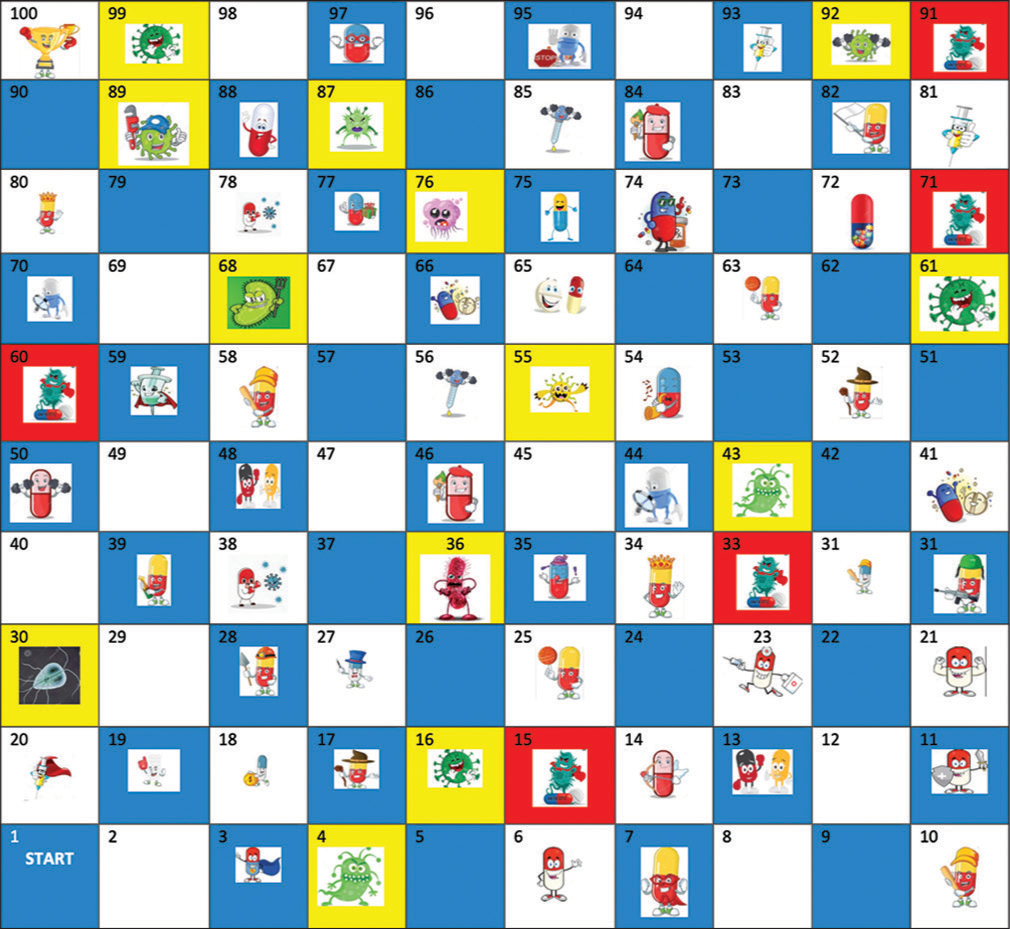
- Figure depicts a virtual board containing drugs, microorganisms (bugs) and mutated micro-organisms. (Blocks containing antibiotics- Blue/white in colour, microorganisms -yellow in colour, mutated organisms- red in colour).
A set of questions was prepared in advance that varied from lower-order questions to higher-order thinking. The questions were based on:
Mechanism of action
Uses and adverse effects
Image-based questions
Drug of choice for various conditions
Guess the drug name/adverse effects based on WhatsApp emoji
Match the following
Provide a rationale for the treatment given in various case scenarios
Word Puzzle – identification of 10 antimicrobials.
The case scenarios contained irrational prescription/treatment and drug-resistant cases. The students had to analyse the case scenario and then comment on the treatment given. This helped them to understand the importance/role of AMSP and global burden of AMR. Furthermore, questions related to antimicrobial stewardship were asked so that students were able to understand the importance of AMSP as well. The questions were prepared in the form of Microsoft PowerPoint, each slide contained a question and numbered in chronological order.
A batch of 200 students was divided into 24 groups, each containing 8–9 students. On the day of GBL, a pre-test was conducted to assess their understanding of the topics based on didactic lectures. Instructions were clearly conveyed to the students. The players rolled the dice to decide who started the game. The player with the highest number was allowed to play first. Every player moved his or her pawn according to the number rolled. Whenever a player landed on a square with the name of an antibiotic (pill) on it, he/she had to answer a question. If the player answered correctly, he/she would move 3 blocks ahead, if wrong, would move back by 2 blocks. If he/she landed on a block containing the mutation, move back by 2 blocks. If the player landed in a block containing a microbe, suggests that he/she is infected with microorganism and would take time to recover. So the player would move back by 3 blocks. The question was passed to the next group if any group failed to answer. If the player answered correctly, he/she would move 3 blocks ahead, if wrong, would move back by 2 blocks. If he/she landed on a block containing the mutation, move back by 5 blocks. The game was over when a player reached the last square on the board (cure). The group who reached the target first were considered to be the winners. Furthermore, after every question, there was a discussion regarding different options (drug/disease) of multiple choice questions (MCQ). This was followed by post-test with the same set of questions given for pre-test. The students were also required to provide a feedback questionnaire about the students’ perception regarding the teaching-learning method. The pre-test and post-test scores were compared.
Statistical analysis
The number of right, wrong or unknown answers from the pre-test and post-test were compared for each student using the paired t-test (P < 0.05). The analysis was performed using GraphPad Prism.
RESULTS
A batch of 200 students was randomly divided into 24 groups, each containing 8–9 students. The study population included 2nd-year medical undergraduates. Table 1 depicts a comparison of pre-test and post-test scores of GBL. As indicated in Table 1, there was a significant improvement in post-test scores compared to pre-test scores in GBL (P < 0.0001, n = 200).
| Test scores | Mean±SD |
|---|---|
| Pre-test scores | 14.46±0.29 |
| Post-test scores | 17.55±0.26* |
| P-value | 0.0001 |
Student t-test. *P<0.0001 (n=200). SD: Standard deviation
Table 2 depicts the perception of 2nd-year medical undergraduate students on GBL as a teaching-learning method using a 5-point Likert scale.
| Q. No | Items | Response (%) | ||||
|---|---|---|---|---|---|---|
| 5 | 4 | 3 | 2 | 1 | ||
| 1 | The game-based teaching-learning method is more enjoyable | 51 | 39 | 1.5 | 3.5 | 5 |
| 2 | The game improved your knowledge about antimicrobials compared to the didactic lecture | 49 | 42.5 | 0.5 | 3.5 | 4.5 |
| 3 | The questions framed were useful in reinforcing your theoretical knowledge. | 51.5 | 40 | 1 | 3 | 4.5 |
| 4 | The game enhanced your knowledge about antimicrobials | 50.5 | 44 | 0 | 2.5 | 3 |
| 5 | The game rules were easy to understand | 49 | 38 | 1.5 | 4 | 7.5 |
| 6 | The design of game – drugs, bugs and microbes with mutation was appropriate | 48 | 41.5 | 0.5 | 3.5 | 6.5 |
| 7 | The image-based/WhatsApp emoji-based questions were interesting | 59 | 33.5 | 1 | 2.5 | 4 |
| 8 | The case-based questions related to antimicrobials were useful | 46.5 | 43 | 2 | 3.5 | 5 |
| 9 | There was thematic organisation of content to promote higher-level thinking | 45 | 44 | 1 | 4 | 6 |
| 10 | Group learning and interactive learning enhance your understanding of concepts better | 48 | 41.5 | 0.5 | 4.5 | 5.5 |
| 11 | Such games should be recommended for other topics as well | 46 | 43.5 | 1 | 4.5 | 5 |
| 12 | Were you satisfied with the game? | 49 | 42 | 1.5 | 3 | 4.5 |
5-point Likert scale, where 1: Strongly disagree, 2: Disagree, 3: Neutral, 4: Agree and 5: Strongly agree. (n=200)
Table 3 depicts perception of students on this teaching–learning method.
| Positive comments | Suggestions for improvement |
|---|---|
| Good and perfect | Study duration should have been shorter |
| It was fun to participate in GBL that enabled revision of the topics | Kahoot quiz would have been better with individual participation |
| Good way to learn. Interesting | Should have used timer for everyone |
| GBL should be conducted very often | |
| Should be conducted for every topic | |
| The amount of effort taken by the faculty is really commendable. Able to remember things a lot better |
GBL: Game-based learning
DISCUSSION
This game-based study was basically planned to improve the knowledge of undergraduates about antimicrobials and enhance their interest in joint learning. As per the study conducted in Saudi Arabia, 18.1% of medical undergraduates perceived that antibiotics could be used against viral infections.[7] In addition, a study by Nogueira-Uzal et al. reveals significant gaps in the knowledge of medical students about antibiotics usage, especially for flu and cold.[8] Various studies have revealed that AMR is a global burden and demands serious steps to help combat it.[9,10] As per the study conducted by Wasserman et al., the majority of the students opined lack of knowledge about the spectrum of antibiotics and selection of the correct antibiotics, their dosing and duration.[11] The reason for this might be the lack of adequate antimicrobial education for students, which could have a negative impact on the future generation. As per the World Health Organization report on preclinical and clinical drug development, very few antibiotic agents appear to be in the pipeline, thereby highlighting the importance of saving existing antibiotics to combat drug-resistant infections.[12,13] There exists an urgent need to provide adequate knowledge of various antimicrobials to medical undergraduates. However, it isn’t easy to acquire a vast amount of knowledge about antimicrobials with the traditional method of teaching. Therefore, GBL was chosen to make the topic more interesting and enjoyable. There are various types of games that can be chosen; however, the virtual board game was chosen in our study as it was easily affordable and more convenient. As per the results pertaining to pre and post-test scores, there was a significant improvement in students’ knowledge about antimicrobials after GBL compared to didactic lectures. The probable reason for this improvement could be the design of the study conducted and the teaching-learning method. In our study, we incorporated different types of questions varying from lower-order to higher-order questions. In the beginning, we had a set of questions based on mechanism of action followed by image-based questions. The next set had different fixed-dose combinations where students had to provide rationale for such combinations. We also had MCQs pertaining to the drug of choice in different clinical scenarios and matched the following as well. As the students these days are tech savvy and use WhatsApp, most of the time, we prepared a set of questions based on WhatsApp emojis that depicted a particular antibiotic. We were overwhelmed by the student’s quick response in guessing drug names in this round. The next set of questions was about various aspects of AMSP, where the students had to comment on the treatment given. The questions mainly covered aspects such as double anaerobic coverage, choice of antibiotics in case of resistance to a particular antibiotic, pharmacokinetic parameters of antibiotics like blood-brain barrier penetration, concepts of time-dependent killing, concentration-dependent killing and pharmacological antagonism (antiretroviral drugs). The major advantage was after every question we had a brief discussion about the condition and different options. Hence, the concepts were made clear to the students through group discussions. As it was GBL, they participated actively and with great enthusiasm. Finally, we had a ‘puzzle round’, which was open to all groups. The students had to identify ten hidden antimicrobials. The group which identified first and correctly was given bonus points. Another advantage of our study, we used a virtual board game, which is affordable and accessible to almost all institutions, instead of expensive software. The students also provided feedback regarding their perception of GBL as a teaching-learning method. Hence, most of them found it interesting and enjoyable and believed it reinforced their theoretical knowledge. They opined that interactive learning through group discussions helped them in better understanding of the concepts, game design was quite simple, and rules were easy to understand. The limitations of the study were that we could have divided the entire batch into two groups. Didactic lectures could be delivered to one group and GBL method to the other and then compared between both the groups. However, because of time constraints and not depriving one group of being involved in GBL, we involved the entire batch and then assessed them based on pre and post-test scores. Results from the previous study also suggest that GBL helps in better retention of subjects through active participation. However, a longer follow-up time is required to validate this parameter. Again, because of time constraints, we could not assess the retention time. Overall, our study results suggest that GBL can be an excellent mode of teaching-learning method for understanding concepts about antimicrobials and can be adapted for other topics as well.
CONCLUSION
The game improved knowledge about antimicrobials and AMR through active learning. A virtual board game is easy and affordable to use in developing countries. Hence, such studies can be conducted further to validate the results and follow up to evaluate retention time as well.
Ethical approval
The research/study was approved by the Institutional Review Board at JNMC Institutional Ethics Committee, Jawaharlal Nehru Medical College, KAHER, Belagavi, number MDC/JNMCIEC/242, dated 9th November 2022.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Topical (local) antibiotics for respiratory infections with sore throat: An antibiotic stewardship perspective. J Clin Pharm Ther. 2019;44:829-37.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge of antibiotic use and resistance among students of a medical school in Nigeria. Malawi Med J. 2019;31:133-7.
- [CrossRef] [PubMed] [Google Scholar]
- Understanding the lives of problem gamers: The meaning, purpose, and influences of video gaming. Comput Human Behav. 2019;97:291-303.
- [CrossRef] [Google Scholar]
- Special series on “effects of board games on health education and promotion” board games as a promising tool for health promotion: A review of recent literature. Biopsychosoc Med. 2019;13:5.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of gamification on antimicrobial resistance knowledge and its relationship to dentistry in Saudi Arabia: A randomized controlled trial. BMC Public Health. 2020;20:680.
- [CrossRef] [PubMed] [Google Scholar]
- Game-based e-learning is more effective than a conventional instructional method: A randomized controlled trial with third-year medical students. PLoS One. 2013;8:e82328.
- [CrossRef] [PubMed] [Google Scholar]
- Perceptions of medical students towards antibiotic prescribing for upper respiratory tract infections in Saudi Arabia. BMJ Open Respir Res. 2015;2:e000078.
- [CrossRef] [PubMed] [Google Scholar]
- Does the problem begin at the beginning? Medical students' knowledge and beliefs regarding antibiotics and resistance: A systematic review. Antimicrob Resist Infect Control. 2020;9:172.
- [CrossRef] [PubMed] [Google Scholar]
- Resisting antimicrobial resistance. Nat Rev Microbiol. 2020;18:259-60.
- [CrossRef] [PubMed] [Google Scholar]
- The ongoing threat of antimicrobial resistance. Infect Dis Clin North Am. 2020;34:13-4.
- [CrossRef] [PubMed] [Google Scholar]
- South African medical students' perceptions and knowledge about antibiotic resistance and appropriate prescribing: Are we providing adequate training to future prescribers. S Afr Med J. 2017;107:405-10.
- [CrossRef] [PubMed] [Google Scholar]
- Antibacterial agents in clinical development: An analysis of the antibacterial clinical development pipeline Geneva: World Health Organization; 2019.
- [Google Scholar]
- Antibacterial agents in preclinical development: An open-access database Geneva: World Health Organization; 2019.
- [Google Scholar]




