
Translate this page into:
Capecitabine-induced lupus erythematosus: A rare occurrence
*Corresponding author: Rishu Sarangal, Department of Dermatology, Government Medical College, Patiala, Punjab, India. sarangalr@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dhanju NK, Gupta S, Sarangal R, Chopra D. Capecitabine-induced lupus erythematosus: A rare occurrence. Indian J Physiol Pharmacol. 2025;69:96-8. doi: 10.25259/IJPP_13_2024
Abstract
Drug-induced lupus erythematosus (LE) is an autoimmune event where the patient develops cutaneous LE-like symptoms after exposure to certain drugs. Capecitabine is an antineoplastic drug that is used in the treatment of various cancers. Here, we report a case of a 36-year-old female, a known case of stage-4 metastatic breast carcinoma, who presented with photosensitive erythematous plaques on the face, neck and forearms along with thrombocytopenia after the fourth cycle of capecitabine. Clinical presentation and dermoscopy of the rash were consistent with subacute cutaneous lupus erythematosus (SCLE), which was confirmed by skin biopsy and serology. Skin lesions, as well as thrombocytopenia, improved after stopping capecitabine. This is the first case report of SCLE induced by capecitabine from our country.
Keywords
Capecitabine
Chemotherapy
Drug-induced subacute lupus erythematosus

INTRODUCTION
Lupus erythematosus (LE) is a diverse group of autoimmune connective tissue disorders characterised by the existence of autoantibodies against nuclear and cytoplasmic antigens.[1] Drug-induced erythematosus (DILE) forms 6–12% of all lupus cases, which is an autoimmune phenomenon where patients develop LE-like features after exposure to certain drugs. More than 100 drugs have been associated with DILE, such as procainamide, hydralazine, interferon alpha, isoniazid, minocycline, phenytoin, penicillamine, carbamazepine and ethosuximide, and the list is increasing with the advancement of newer biologic agents.[2]
Capecitabine is an orally administered antimetabolite chemotherapeutic drug used for various cancers, including metastatic breast and bowel cancer.[3] The most common side effects include low white blood cell (WBC) count, anaemia, hand-foot syndrome, diarrhoea, elevated liver enzymes, skin rashes, itching and abdominal pain.[4] There are few case reports on the association of DILE with capecitabine in the current literature and none from our country.[5-11] We report a case of drug-induced subacute cutaneous lupus erythematosus (SCLE) in a patient receiving capecitabine for metastatic breast carcinoma.
CASE REPORT
A 36-year-old female, who was under treatment in radiation oncology for metastatic breast carcinoma for 2 years, presented to our outpatient department with photosensitive skin rash from 1 week. Her oncology record showed that she was diagnosed with a case of breast carcinoma in 2020, for which a modified radical mastectomy with axillary lymphadenectomy was done, and she was started on tamoxifen. However, after 2 years, her contrast-enhanced computerised tomography pelvis showed signs of osseous metastasis, and whole abdomen ultrasonography showed hepatic metastasis as well. The patient was then started on palliative treatment with oral capecitabine as monotherapy 1250 mg/m2 twice daily for 2 weeks, followed by a 1-week rest period in 3 3-week cycles and anastrozole 1 mg once daily.
After completing 4th cycle of chemotherapy, she developed a skin rash and thrombocytopenia. The skin lesions were multiple, polycyclic, erythematous, mildly scaly plaques distributed on photoexposed areas, including the face, neck and extensors of forearms [Figure 1a and b]. A single blister on the erythematous plaque was seen on the left arm [Figure 1c]. She had no other features of LE. On dermoscopy, patchy white scales on a pink-red background and red structureless areas suggestive of SCLE were seen [Figure 2a]. Histopathology showed thinning of the epidermis exhibiting spongiosis along with basal layer vacuolation. Dermis showed collagenisation with pigment incontinence and focal lymphocyte inflammatory infiltrate [Figure 2b and c], confirming the diagnosis of LE. The autoimmune profile workup revealed a positive antinuclear antibody (ANA) titre of >1:100. Her blood counts were haemoglobin – 7.9 g, WBC – 5210 and platelet count – 62000 (thrombocytopenia). We could not perform anti-histone antibody testing due to non-availability in our hospital. However, there was a clear temporal relationship between the appearance of photosensitive SCLE and thrombocytopenia with capecitabine.
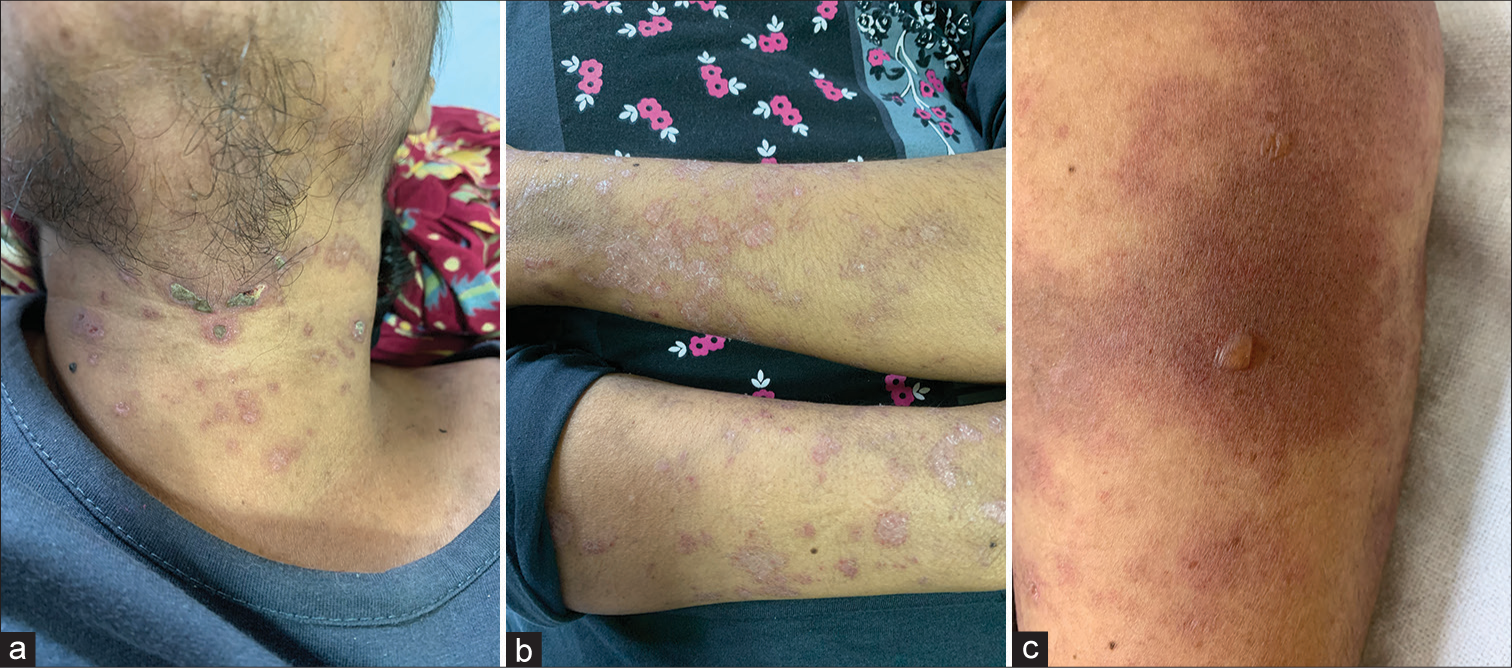
- (a-b) Multiple, polycyclic, erythematous, mildly scaly, plaques distributed on photoexposed areas. (c) Single blister on erythematous plaque was seen on the left arm.
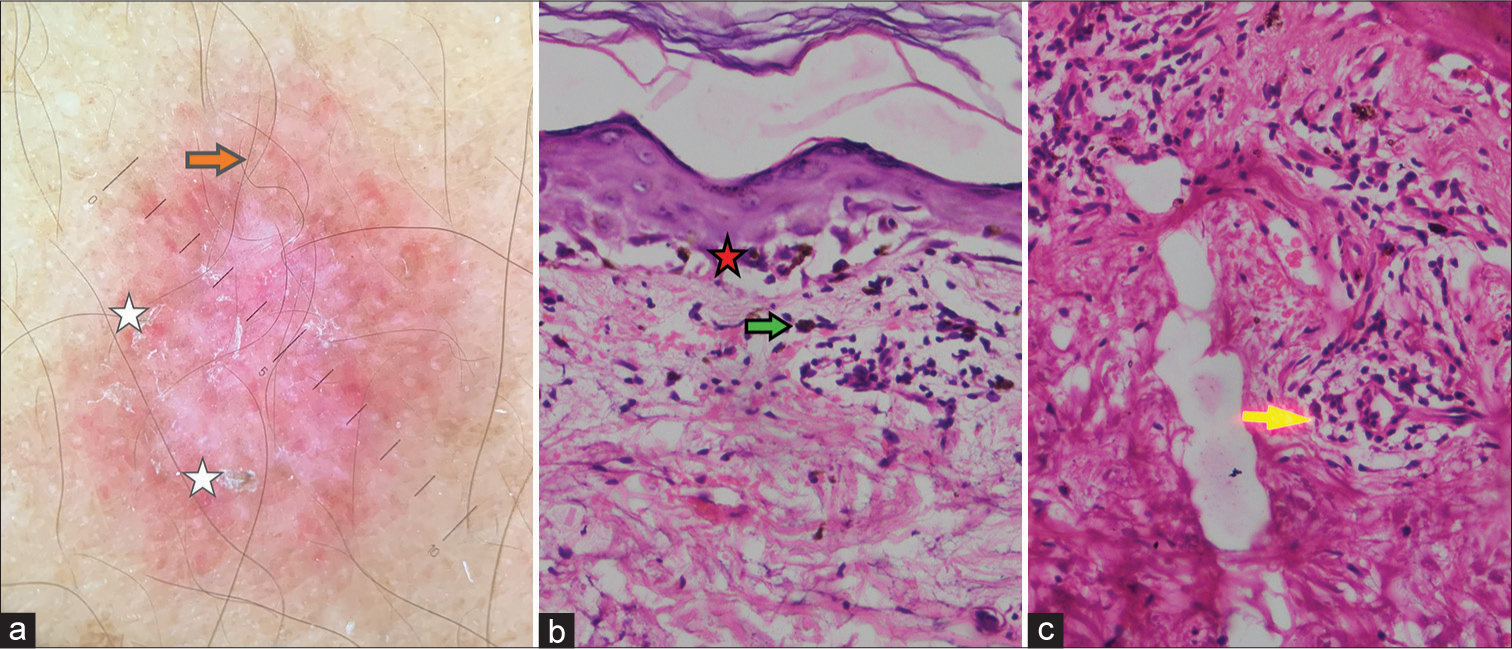
- Dermoscopic examination revealing patchy white scales (white star) on pink red background and red structureless areas (red arrow) (a). (Heine Delta 20T dermatoscope, nonpolarized contact mode, ×0). Basal layer vacuolation (red star) and pigment incontinence (green arrow) (b), Lymphocytic infiltrate (yellow arrow) in the dermis (c) (H and E stain, ×40). H and E: Haematoxylin and Eosin.
Her capecitabine cycles were withheld, and she was started with hydroxychloroquine 200 mg twice a day along with topical corticosteroid and sun protection. Her lesions rapidly improved with the treatment in a week.
DISCUSSION
To diagnose and classify DILE, the following guidelines are used:[1]
Treatment with suspected drug for at least 1 month or longer
Symptoms/organ involvement: myalgia, fever, serositis, arthralgia and dermatological rash
Laboratory findings: ANA titre, anti-histone antibodies positive with other anti-Sm and anti-double-stranded DNA being negative
Improvement in symptoms within days to a week with discontinuation of the drug.
DILE can present as systemic LE, SCLE, chronic cutaneous LE and cutaneous LE tumidus. Drug-induced SCLE is the most common variant, and its clinical features include annular-polycyclic lesions.[2] It may present weeks to months after initiation of the offending drug.[2,5] According to a PubMed search, there are only 16 case reports of DILE after capecitabine to date. Out of which, SCLE was seen in 11 patients.[5-7] Systemic lupus erythematosus was seen in 2 cases[5,8] and discoid lupus erythematosus was seen in 3 cases.[5,9,10] Most of the cutaneous lesions occurred after 2 cycles of capecitabine.[5] Capecitabine is an antineoplastic drug that is enzymatically converted to 5- fluorouracil (5-FU), which is a pyrimidine analogue and interferes with tumour cell proliferation by inhibiting DNA synthesis. It is taken orally and is used in the treatment of metastatic breast cancer and colorectal cancer.[11] Previous animal studies have demonstrated a link between 5-FU, ultraviolet B (UVB) radiation and the development of cutaneous lupus-like lesions, as 5-FU damages the basal layer of the epidermis and makes the epidermis more susceptible to UVB damage.[12] Studies have also hypothesised that chemotherapeutic agents translocate SSA/Ro to the surface of basal keratinocytes in a manner similar to UVB light.[13,14] These hypotheses can explain the pathogenesis of photosensitive drug-induced SCLE secondary to capecitabine.
CONCLUSION
Till date, only a few cases of drug-induced LE have been reported and none has been reported from India. Considering the increasing use of capecitabine in cancer therapy, an understanding of this under-reported cutaneous manifestation is of utmost importance in this exposed legion of patients.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Drug-induced lupus erythematosus. Autoimmunity. 2005;38:507-18.
- [CrossRef] [PubMed] [Google Scholar]
- Drug-induced lupus erythematosus In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022.
- [Google Scholar]
- Capecitabine: Fulfilling the promise of oral chemotherapy. Expert Opin Pharmacother. 2002;3:733-43.
- [CrossRef] [PubMed] [Google Scholar]
- Photosensitive lichenoid skin reaction to capecitabine. BMC Cancer. 2017;17:866.
- [CrossRef] [PubMed] [Google Scholar]
- Systemic 5-fluorouracil induced lupus erythematosus: A review of the literature. Dermatol Online J. 2019;25:13030/qt3nw0p7hn.
- [CrossRef] [PubMed] [Google Scholar]
- Capecitabine-induced subacute cutaneous lupus erythematosus. An Bras Dermatol. 2019;94:618-9.
- [CrossRef] [PubMed] [Google Scholar]
- Subacute cutaneous lupus erythematosus induced by Capecitabine: Confocal microscopy and dermoscopy findings. Dermatol Ther. 2022;35:e15705.
- [CrossRef] [Google Scholar]
- Toxidermy mimicking acute chemotherapy-induced lupus erythematosus. Pan Afr Med J. 2018;29:66.
- [CrossRef] [PubMed] [Google Scholar]
- Discoid lupus erythematosus lesions associated with systemic fluorouracil agents: A case report and review. Cureus. 2020;12:e7828.
- [CrossRef] [Google Scholar]
- A case of capecitabine-induced discoid lupus erythematosus. Ann Dermatol. 2020;32:348-50.
- [CrossRef] [PubMed] [Google Scholar]
- Spotlight on capecitabine in the management of advanced breast cancer. Am J Cancer. 2003;2:137-40.
- [CrossRef] [Google Scholar]
- Susceptibility of T cell receptor-alpha chain knock-out mice to ultraviolet B light and fluorouracil: A novel model for drug-induced cutaneous lupus erythematosus. Clin Exp Immunol. 2004;136:245-54.
- [CrossRef] [PubMed] [Google Scholar]
- Antinuclear antibody-keratinocyte interactions in photosensitive cutaneous lupus erythematosus. Histol Histopathol. 1999;14:627-34.
- [Google Scholar]
- Anti-SSA/Ro antibody as a risk factor for fluorouracil-induced drug eruptions showing acral erythema and discoid-lupus-erythematosus-like lesions. Dermatology. 2007;214:85-8.
- [CrossRef] [PubMed] [Google Scholar]




