
Translate this page into:
Introduction to early clinical exposure as learning tool in physiology
*Corresponding author: Anil B. Warkar, Department Physiology, Government Medical College, Akola - 444 001, Maharashtra, India. warkar.anil@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Warkar AB, Asia AA. Introduction to early clinical exposure as learning tool in physiology. Indian J Physiol Pharmacol 2020;64(Suppl_1):S62-S9.
Abstract
Objectives:
Early years of undergraduate medical education (especially the first 2 years) are critical for the academic success of medical students. In the traditional curricula of medical education, students learn theoretical knowledge without contact with the patient in a clinical context. Early clinical exposure (ECE) has been suggested to help medical fresh students overcome their stresses and motivate them to develop better insight and awareness to the medical profession.
Materials and Methods:
We devised a teaching-learning ECE intervention study module in endocrine physiology, which comprised traditional didactic lectures, supplemented with an ECE program in a hospital setting, a hospital visit to see patients. The study group was given the intervention of ECE, through the ECE designed module. The outcomes and effectiveness of this intervention were assessed by a multiple-choice pretest/post-test model of learning knowledge gain and effectiveness of the educational intervention by calculating learning matrices. Students feedback toward ECE was assessed by a 5 point Likert-scale responses and their views through a validated questionnaire.
Results:
Mean pre-test and post-test scores of students learning improved significantly from 9.6 ± 2.58 (48%) to 13.2 ± 2.53 (66%), (P = 0.043) in the study group. The learning gain (gi) for individual students was tabulated and average single student normalised gain Gi(avg) was calculated. For the study group, it was 29 ± 33% and control group 7 ± 14%. To assess the intervention effectiveness class average normalised gain G was found to be 34%, in the study group and 13% in the control group (P < 0.05). The study group students (96.4%) gave an overall rating of good/excellent to ECE on a five-point Likert scale. The mean score was (4.3 ± 1.4) showing that the overall rating of ECE was good to excellent.
Conclusion:
The pre-test/post-test model with a calculation of various measures of learning gain provides an objective and informative means to document learner performance and demonstrate the effectiveness of the educational intervention. The students’ satisfaction and their positive attitude toward ECE suggested that this interventional study improves the quality of basic science courses and adds substantial relevance to clinical application.
Keywords
Early clinical exposure
Learning gain
Intervention effectiveness
Student perception

INTRODUCTION
Early years of undergraduate education (especially the first 2 years) are critical for the academic success of medical students. Such success depends not only on the expanding knowledge learned during these years but also on pre-conceived attitudes toward medicine and the role of the physician.[1]
In the traditional curricula of medical education, students learn theoretical knowledge without contact with the patient in a clinical context. Moreover, when students are posted in clinical fields they cannot recall important basic scientific concepts; therefore, part of their academic education becomes impractical.[1,2] At the same time, students tend to feel slightly anxious and apprehensive when faced by real-life clinical situations for which they are psychologically unprepared. Possible contributing factors include stress due to the tremendous amount of material to be learned, perceived lack of relevance of the basic science years. The medical education community has been greatly emphasising the value of early patient contact experiences for preclinical medical students. The prime objectives of which include, getting acquainted with patients; basic clinical-skills training, promoting interest in primary care and encouraging active learning in preclinical settings. Data suggest that early clinical exposure (ECE) can make basic science curricula more relevant.[3]
ECE has been suggested to help medical fresh students overcome their stress and motivate them to develop better insight and awareness to the medical profession.[4] ECE involves active, experiential learning from patients along with practising clinicians, designed to be the ‘beginning of a lifelong learning focused on the patient.’[5] There seems to be no ‘best’ way to conduct ECE.[6] Implementing a short-term period of ECE program could influence medical students attitude toward medical education, boost their confidence in their ability to succeed in medical practice and gain social, emotional and professional satisfaction. Different teaching methods have been used to introduce an ECE program comprising mainly of a hospital round to learn about patients’ needs and health-care system. This arouses student’ interest and enhances their learning.[7]
Teaching endocrine physiology to the 1st-year medical students, in an effective manner has always been a challenge. Students are motivated and their performance improves when the instruction is adapted to their ‘Learning preferences and styles.’[8] Various methods are being used as alternative approaches to reinforce didactic instruction in endocrine physiology, such as case-stimulated learning, problem-based learning and patient-centred learning through ECE. There are studies on ECE in Indian context conducted in the previous 2 to 3 years only.[9-12] Most of the studies are based on students perception of ECE, one study has included faculty perception also.[13] The Medical Council of India in vision 2015 Document has recommended curricular reforms for undergraduate medical students and ECE is one of them for 1st-year medical students. Reviewing the literature for Indian studies on ECE reveals that ECE is implemented recently in the competency-based curriculum but it is still in infancy. None of the studies has a quantitative measurement of ECE learning outcomes. A quantitative analysis such as individual students learning gain and overall program effectiveness can be useful to study the effectiveness of teaching-learning through ECE method.[14] As per literature, only one study has detailed how the ECE program was given[12] but most of the studies have not clearly explained the designing and implementation of the ECE program in their study. With this background knowledge, we wish to introduce a short-term ECE educational intervention to 1st-year medical students. This study is based on quantitative measurement of knowledge gain by individual student, the overall effectiveness of the program and students perception of ECE.
This study aims to assess the effectiveness of ECE as a teaching-learning tool for 1st-year medical students. The objectives are to calculate and compare the learning gain for an individual student and learning gain for the whole program by conventional teaching method and through ECE intervention and also to study the student’s perception regarding ECE intervention.
MATERIALS AND METHODS
Study design
It was an experimental interventional study based on the pretest/post-test intervention study design model. The study was conducted in the Department of Physiology Government Medical College, and General Hospital, Akola, Maharashtra, in collaboration with Department of Medicine, GMC, Akola.
Selection of students
Second term students of 1st-year MBBS batch comprising 150 students were selected for the study. Informed consent was obtained for participation in this study. Students were categorised into two groups of 75 each, by lottery system of selection. Group (A) was given interventional exposure to ECE whereas the other control group (B) was taught only through conventional didactic lectures.
Ethical issues
The proposed Educational Project was approved by the Institutional Ethical Committee.
Methods
The students and the faculty were briefly introduced about the study. After completion of the traditional didactic lectures by the faculty, a pre-test was given to study as well as a control group to assess the knowledge of the topics. Then, the study group (A) was given early clinical intervention through the ECE developed module. The residents from the Department of Medicine Government Medical College and Hospital Akola were informed 1 month in advance about the ECE intervention.
ECE module
The study group (A) students (n = 75) were divided into three batches A1, A2 and A3 of 25 students in each group. The duration of early clinical intervention was 10 weeks (2½ month) with 2 h/week. Three topics on endocrine physiology namely thyroid gland, adrenal cortex and endocrine pancreas were chosen for the study. ECE was given in hospital settings. The Residents from Medicine Department and the Faculty from the Physiology Department included teaching the students. On the scheduled day of ECE intervention, the study group batches (A1, A2 and A3) were taken to the medicine wards of our institute. The teachers from physiology department first taught the topic to each of their allotted respective batches. Each respective batch was further subdivided into two groups of 13 and 12 students each. The residents and faculty from medicine department taught the same topic on clinical cases to the small subdivided groups of study group batches. Three endocrine glands, namely thyroid, adrenal cortex and endocrine pancreas were taught. The cases of hyperthyroidism, hypothyroidism, diabetes and Addison’s disease were used for ECE intervention. In the first rotation, ECE intervention was given as A1- Thyroid case, A2- Adrenal cortex case and A3- Endocrine Pancreas Case. In the next rotation, A1 - Adrenal cortex case, A2 -Endocrine Pancreas case and A3 - Thyroid Case similarly in the further rotation A1 - Endocrine Pancreas, A2 - Thyroid Case and A3 - Adrenal cortex case. Cooperative patients with uncomplicated medical conditions were selected to be visited by medical students. Each batch of 25 students was given the intervention once in a week. In this way, all the three topics were taught to the study group in total 10 weeks of duration.
After giving ECE intervention to study group (A) and didactic teaching to control group (B), a post-test was given to both the groups to assess the knowledge gain in endocrine physiology. To assess the feedback of the students for the new method of teaching by ECE in learning physiology, the feedback was taken from the study group students with validated questionnaire. Simultaneously after the post-test, the control group was also given the intervention of ECE with two topics of endocrine physiology as they should not suffer from learning through a new approach. This was followed by feedback from the control group students for this new intervention with the same validated questionnaire, given to the study group.
Data collection method
This program was intended to assess the learning gain and also assess the feedback from the students for the new method of teaching in physiology by ECE for learning physiology.
For learning gain
A multiple-choice question of cognitive knowledge was developed for pre-test and post-test assessment of knowledge gain. It comprised 20 items with 20 marks. The questions were normalised for a specific topic. A pre-test before the beginning of ECE intervention and a post-test after ECE intervention were given to the students to assess the knowledge gain. The scores for pre-test and post-test for Group A and Group B were tabulated.
For students feedback
A set of the questionnaire (15 items) was given at the end of the entire intervention program to study group to assess the attitude of the students toward ECE. The same validated questionnaire was given to Group B for their feedback regarding ECE intervention. The questionnaire had both open-ended questions, which yielded narrative comments and structured questions, which yielded semi-quantitative data. Each item was scored on a five-point Likert scale, with a score of 1 = poor, 2 = not adequate, 3 = satisfactory, 4 = good and 5 = excellent to determine the overall rating of the program by the students. The validity of the questionnaire was assessed by three experts in medical education Unit of the Institute and its reliability was confirmed via the test-retest method. Cronbach’s alpha coefficient was 0.7. Alpha coefficient of 0.7–0.79 is the acceptable levels for educational research.[14,15] The theme of the questions was based on the understanding of physiology, acquiring knowledge, development of interest, motivation to read, awareness about patients problem and needs and what students liked. They were asked to read each item carefully and then answer using a 5 point Likert-type scale from strongly agree to strongly disagree. The data were collected by the students’ representative.
Data analysis
We hypothesised that participation in this educational intervention for 2½ months would result in improved class and individual student learning gains in cognitive knowledge. For this study, the learning effectiveness was defined as the extent to which the intervention study produced learning gains for the group and for individual students as demonstrated by several metrics of student performance.
Pre-test and post-test scores of both the groups were compared and the effectiveness of the educational intervention for the group as a whole was determined using a predefined target objective of at least 0.3 (30%) for class average normalised gain (G).[16] Assessment and analysis of qualitative evaluations and Likert-scale survey measurements from each participant by reviewing results from post-course student questionnaires was done. The data were analysed using SPSS-PC Base 15 for windows. The quantitative data are reported in frequency distributions. In the qualitative data analysis, the themes were identified for each open-ended question for the students ‘views regarding ECE intervention.’
Statistical methods
Learning knowledge gain
This was a pre-test/post-test study designed to assess learning gain and effectiveness of the educational Intervention of ECE in learning physiology. Mean of cases for pre-test and post-test scores were tabulated to calculate the learning gains.
The paired-sample t-test with an α = 0.05 was used to compare pre- and post-test scores.
The following learning gain matrices were studied.
Individual single-student normalised gains (Gi) were calculated for all students. Gi=Post-test score – Pre-test score
Average single students normalised gain G(avg) G(avg) = [Σ(Gi)]/N
Individual single-student Gi values to identify the learning gain variability among students and the average single student normalised gain were calculated.
Intervention effectiveness
As a measure of learning intervention effectiveness, the class average normalised gain (G) was calculated.
(G) = [(%post-test) − (%pre-test)]/[100% − (%pre-test)]
A predefined target (G) of 30% was taken as defining the minimum value at which the educational intervention could be regarded as effective.[9]
RESULTS
Learning gain
Seventy students out of 75 completed the complete sessions and gave both the pre-test and the post-test and program feedback evaluation. The response rate was 93.33% (70/75). Mean test scores of pre-test and post-test in study group improved significantly from 48% (9.6/20 ± 2.58) to 66% (13.2/20 ± 2.53) (P = 0.043). Individual single students normalised gain (Gi) values were also increased in the study group. The average single student normalised gain (Gavg) for the control group (7% ± 14%) with significantly increased (P < 0.05) in the study group (29% ± 33%), as shown in [Table 1 and Figure 1].
| Parameters | Student group | Pvalue | Result | ||||
|---|---|---|---|---|---|---|---|
| Study group A n=75 |
Control group B n=75 |
||||||
| Pre-test scores (MCQ) | 9.6/20±2.5 48% | 9.48/20±2.71 47.4% | >0.05 | NS | |||
| Post-test scores (MCQ) | 13.2/20±2.5 66% | 9.8/20±2.21 49% | <0.05 | S | |||
| Gi(avg) | 29%±33 | 7%±14 | <0.05 | S | |||
| G | 34% | 3.02% | <0.05 | S | |||
P<0.05 was considered significant. S: Significant, NS: Not significant. Gi(ave) is the average single-student normalised gain: Gi(ave) = [Σ from 1 to N (Gi)]/N, Where gi = post-test score – pre-test score for individual students. G is the class average normalised gain: G = [(% post-test) − (% pre-test)]/[100% − (% pre-test)]. Hake criterion for educational intervention is effective if G is >30%. MCQ: Multiple-choice question
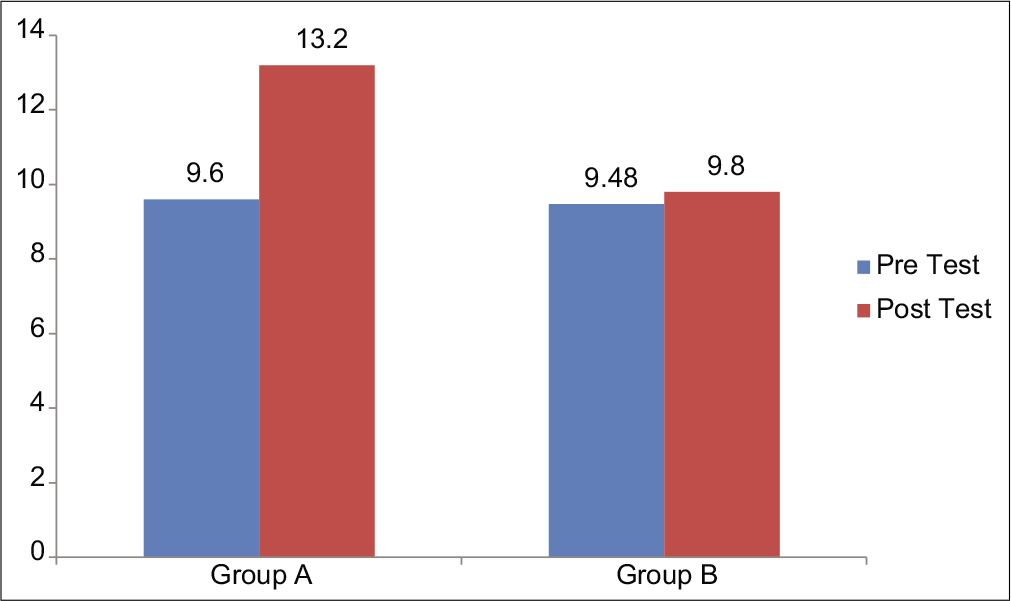
- Comparison of Pre test & post test scores in Group A , Study group & Group B Control group.
Intervention effectiveness
The class average normalised gain (G) was 34%, in the study group as compared to 13% in the control group with (P < 0.05), as shown in [Table 1 and Figure 2].
![Learning gain and learning effectiveness. Gi(ave) is the average single-student normalised gain: G(ave) = [Σ (Gi)]/N, Where Gi = post test score – pre test score for individual students. G is the class average normalised gain: G=[(% post-test) − (% pre-test)]/ [100% − (% pre-test)]. Hake criterion for educational intervention is effective if G is >30%.](/content/114/2020/64/Suppl 1/img/IJPP-64-S62-g002.png)
- Learning gain and learning effectiveness. Gi(ave) is the average single-student normalised gain: G(ave) = [Σ (Gi)]/N, Where Gi = post test score – pre test score for individual students. G is the class average normalised gain: G=[(% post-test) − (% pre-test)]/ [100% − (% pre-test)]. Hake criterion for educational intervention is effective if G is >30%.
Feedback assessment
The study group students (96.4%) gave an overall rating of good/excellent to ECE on a five-point Likert scale; the mean score being 4.3 ± 1.4, as shown in [Figure 3]. Overall, 98% of the students were satisfied with the intervention and believed that ECE helped them to become more familiar with the clinical environment and reduce their fear. About 80% felt that clinical contact and interaction was the best feature of the program and increased the student’s interest in the learning of basic sciences and their application. Their motivation to study basic sciences had increased their understanding (92%). About 83% of students reported it helped them in integrating the knowledge they learned through ECE. These visits to wards and patients gave a favourable insight toward medical education (21%).

- Likert scale rating for overall rating of the module.
More familiar with work environment (36%), learn how to behave towards patients (3%), professional’s development (46%) and received a new insight enabled them to see the patient as a person within a family (5%). About 67% of the students expressed a desire and a need for ECE to be implemented in teaching basic sciences for each system. About 32% of students expressed a new attitude toward medical ethics and professionalism shown in [Figure 4]. Clinical contact enhanced their sensitivity toward the patient’s problems and needs. Students showed a very positive perception for ECE intervention, as shown in [Table 2]. As far as drawbacks are concerned, they said that the number of students per group while seeing the patient was large and there was significant waiting time between two group classes.

- Students’ feedback responses about ECE intervention.
| Understanding of endocrine physiology: | ‘helped us develop a better understanding of the topics’ ‘the classical features in patients helped in understanding the subject deeper’ ‘We could understand well instead of just memorising causes and symptoms of disease’ ‘made the concepts clear’ |
|---|---|
| Acquiring knowledge: | ‘Many things which we would have overlooked were brought to our notice, normal values and especially treatment’ ‘helped for the test’ ‘re-enforced our knowledge’ ‘seeing the patients make things stay much longer in your memory’ |
| Integration of Knowledge: | ‘We were able to relate what we saw with what we had read’ ‘it was a nice class where we could integrate our knowledge’ ‘clinical cases helped us to relate to the subject’ ‘I understood how to apply physiology’ |
| Development of interest: | ‘made theory come alive literally’ ‘was interesting because it broke the monotony of ‘by-hearting learning’ ‘It is interesting to see the things we read in textbooks’ ‘it did.. made me feel like a doc’ |
| Motivation to read | ‘practical exposure to patients gave us more interest to go and read up that day’ ‘seeing the patients motivated us to read more about what we didn’t know’ ‘I had a great interest in my textbook after the visit’ ‘learning was motivating and informative’ |
| Development of sensitivity towards patient problem and needs: | ‘made us more sensitive toward them as we saw their plight’ ‘helped me realise how much trouble each disease causes and be sensitive to the patient’ ‘yes, the hospital visit helped…especially the patient with Cushing’s syndrome’ ‘helped to see how difficult these diseases are for the patient’ |
| What they liked: | ‘It was something like a play-way-method of learning’ ‘We learnt more about clinical applications than we otherwise would have’ ‘seeing cases about which we can only read’ ‘made learning interesting’ ‘why we are studying physiology was clear’ |
Suggestions for improvement of the program included having smaller student groups for the hospital visit. Some students said, ‘can probably have more patients.’ A few students felt that the waiting time could have been utilised in some other learning activity. Some students advocated an increase in the frequency of hospital visits.
DISCUSSION
In this study, we used a pre-test/post-test assessment model, several measures of learning gain, students feedback and Likert-scale analysis, to study the learning effectiveness and perceived educational values by the students for educational intervention in learning physiology.
The effectiveness of this learning intervention, independent of the student’s pre-test level of knowledge, was established using measures of class-average normalised gain (G) and related metrics. This practice is followed in physics education research where it has been shown that (G) for course with widely varying average pre-test scores (%pre) is nearly independent of the pre-test score, being dependent primarily on the effectiveness of the instruction.[16] Weiman and Perkins[17] described the (G) metric as the fraction of concepts that students master, on average, which they did not already know at the start of the class. The class average normalised gain has been described by McGowan and Davis[18] as ‘telling us what the student achieved in tests, given what was possible for her (him) to achieve.’ The use of the single student Gi and its related calculations has received empirical justification as an easy-to-use gauge of learning effectiveness.[19] Furthermore, individualised learning needs can potentially be determined by single student normalised gain assessments. In our study, this performance measure allowed us to document changes in individual scores in addition to explore the overall effectiveness of educational intervention study of ECE in learning endocrine physiology.
As medical education moves to new curricular models, including competency-based education with defined objectives, benchmarks and outcomes and more standardised approaches, it is important to understand and set objectives for each phase of education.[20] While earlier work has defined the preclinical phase,[21] there has been limited attention to the relative values of these experiences for medical students or the objectives, competencies and outcomes associated with early patient experiences. Hence, understanding the benefits of ECE will help shape the best experiences following a curriculum’s objectives. Early clinical experience is a key ingredient to reinforce the integrated base curriculum and increase the value of it. Early clinical experience provides medical students with an experiential context for learning basic science content and opportunities to experience the relevance between basic science knowledge and its clinical application. This enables medical students to obtain a better and deeper understanding of medicinal theory and practice through the application of their knowledge in real hospital situations.[22] The students’ satisfaction and their positive attitude toward ECE suggested that this interventional study improves the quality of basic science courses. It also helps students in getting acclimatised to the hospital environment. As was reported by the previous studies and based on the information supplied by the students, it seems that the application of early contact with patients can increase medical students; enthusiasm and motivation in their education and strengthen their positive attitude towards the medical profession. The early clinical experience helped the students learn about professional roles and responsibilities, healthcare systems and health needs of a population. Early clinical experiences enhance student’s empathic attitudes toward ill people.[6] Our study showed that early clinical experiences called for more attention to the importance of basic sciences and increased the students’ interest in studying basic sciences.
Limitations
This study has several limitations. The study was conducted at a single medical institute and therefore the findings may not be generalised to other medical institutions. Very few topics of a single system were intervened. However, few medical institutes provide multiple types of early patient experiences and this comparison, even if at a single site, provides valuable information.
CONCLUSION
The pre-test/post-test model with the calculation of various measures of learning gain, including class-average and single-student normalised gain, provides an objective and informative means to document learner performance and demonstrate the effectiveness of educational intervention through ECE. The apparent benefits of ECE include exposure to the health-care system, instilling the qualities of a patient-centred humanistic approach and increasing motivation for classroom learning. ECE forms a crucial part in the gradual introduction for students to medicine. Depending on the student’s perception, it would appear that early clinical experience, in tandem with theoretical courses, can provide a framework for the beneficial and successful integration of the teaching and learning of basic sciences in a traditional program.
Acknowledgment
The authors would like to thank Professor and Head, and Faculty from Department of Medicine, Government Medical College, Akola (M.S.)
Future direction
An objective analysis of the effectiveness of this approach could be made by comparing students’ performance with and without the ECE program. In teaching hospitals, where many patients with endocrine disorders may not be admitted in the ward, video clipping of patients is a good option for similar teaching.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Early practical experience and the social responsiveness of clinical education: A systematic review. BMJ. 2005;331:387-91.
- [CrossRef] [PubMed] [Google Scholar]
- Pros and cons of vertical integration between clinical medicine and basic science within a problem-based undergraduate medical curriculum: Examples and experiences from Linkoping, Sweden. Med Teach. 2002;24:280-5.
- [CrossRef] [PubMed] [Google Scholar]
- Educational and career outcomes of an internal medicine preceptorship for first-year medical students. J Gen Intern Med. 1999;14:341-6.
- [CrossRef] [PubMed] [Google Scholar]
- How can experience in clinical and community settings contribute to early medical education? A BEME systematic review. Med Teach. 2006;28:3-18.
- [CrossRef] [PubMed] [Google Scholar]
- Curricular change: Recommendations from a national perspective. Acad Med. 2001;76:S140-5.
- [CrossRef] [PubMed] [Google Scholar]
- A tale of two exposures: A comparison of two approaches to early clinical exposure. Educ Health (Abingdon). 2002;15:386-90.
- [CrossRef] [PubMed] [Google Scholar]
- The American college of chest physician evidence-based educational guidelines for continuing medical education interventions: A critical review of evidence-based educational guidelines. Chest. 2009;135:834-7.
- [CrossRef] [PubMed] [Google Scholar]
- How can physicians' learning styles drive educational planning? Acad Med. 2005;80:680-4.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of comprehensive early clinical exposure program for pre clinical year medical students. Health Prof Educ. 2018;4:133-8.
- [CrossRef] [Google Scholar]
- Effect of early clinical exposure on 1st MBBS student. Int J Curr Med Appl Sci. 2015;8:56-8.
- [Google Scholar]
- Effectiveness of early clinical exposure in learning respiratory physiology among the newly entrant MBBS students. J Adv Med Educ Prof. 2017;5:6-10.
- [Google Scholar]
- Recent trends in teaching and learning in physiology education early clinical exposure and integration. Int J Basic Appl Physiol. 2012;1:175-82.
- [Google Scholar]
- The impact of early clinical exposure on first M.B.B.S. students. Int J Healthc Biomed Res. 2014;2:176-81.
- [Google Scholar]
- Reliability: On the reproducibility of assessment data. Med Educ. 2004;38:1006-12.
- [CrossRef] [PubMed] [Google Scholar]
- Interactive-engagement vs traditional methods: A six-thousand-student survey of mechanics test data for introductory physics courses. Am J Phys. 1998;66:64.
- [CrossRef] [Google Scholar]
- Individual Gain and Engagement with teaching goals.Proceedings of 26th annual conference of the International Group for the Psychology of Mathematics Education. North American Chapter Toronto: OISE.
- The Calculus Concept Inventory-new Data Correlation with Teaching Methodology. Washington, DC: Joint Mathematics Meeting; 2009. p. :5-10.
- [Google Scholar]
- The assessment of clinical skills/competence/ performance. Acad Med. 1990;65:S63-7.
- [CrossRef] [PubMed] [Google Scholar]
- A Taxonomy for Learning, Teaching and Assessing a Revision of Blooms Taxonomy of Educational Objectives Boston: Addison Wesley Longman;
- [Google Scholar]
- Using actual patients in the classroom to develop positive student attitudes toward pharmaceutical education. American Journal of Pharmaceutical Education. 1999;63:296-9.
- [Google Scholar]




