
Sway detection in hypertension as a novel tool to anticipate risk and morbidity due to postural instability
 , Archana Gaur1, Nitin Ashok John1, Sai Shriya Taranikanti3, Madhusudhan Umesh1, Vidya Ganji1, Kalpana Medala1, Sakthivadivel Varatharajan4
, Archana Gaur1, Nitin Ashok John1, Sai Shriya Taranikanti3, Madhusudhan Umesh1, Vidya Ganji1, Kalpana Medala1, Sakthivadivel Varatharajan4
*Corresponding author: Madhuri Taranikanti, Department of Physiology, All India Institute of Medical Sciences Bibinagar, Hyderabad, Telangana, India. madhuri.tarani@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Taranikanti M, Mudunuru A, Gaur A, John N, Taranikanti S, Umesh M, et al. Sway detection in hypertension as a novel tool to anticipate risk and morbidity due to postural instability. Indian J Physiol Pharmacol. 2024;68:216-22. doi: 10.25259/IJPP_161_2024
Abstract
Objectives:
Hypertension contributes substantially to poor physical function and autonomic imbalance. It may cause instability in posture that limits daily activities and can lead to devastating falls. Centre of pressure (CoP) is a commonly used index of postural stability while standing and is a measure of the activity of the motor system, which may be altered in hypertension. It is also observed that the fall incidence is higher in women than men, which may be due to postural instability. The pilot study was conducted to see whether the presence of essential hypertension further contributes to postural instability in women and compared with age-matched normotensive controls.
Materials and Methods:
Sixteen hypertensive women on regular treatment for hypertension and 16 age-matched normotensive women with a mean age of 51.9 ± 9.1 years were included in the study. The WII balance board was used to measure the CoP and displacement to sway. PowerLab 8/35 (AD instruments) with LabChart software was used to measure the parameters.
Results:
Displacement of CoP in the mediolateral direction was studied in the trials. The CoP was measured in eyes closed and eyes open conditions and was displaced in both groups, with significant displacement in hypertensive women. With voluntary sway to their right and left sides, hypertensive women have shown significantly less sway displacement compared to normotensive women. In hypertensives, during right sway, the error of correction was 13%. During left sway, overcorrection was high in both hypertensive and normotensive.
Conclusion:
Postural instability is observed in hypertension, and posturography can be used as a routine screening tool to predict postural instability in hypertensives. Balance training exercise biofeedback protocols and the use of sensory augmentation devices may prove to be useful in improving postural stability.
Keywords
Hypertension
Postural instability
Centre of pressure
Biofeedback

INTRODUCTION
Independence in daily living activities, irrespective of age, can be achieved only with a controlled body posture. Orientation in space and balance needs dynamic adjustments, and sensory afferent inputs have to be well coordinated with neuromuscular performance.[1] Instability in posture can limit daily activities, resulting in psychological disturbances like depression.[2] It can lead to devastating falls, particularly in aged individuals and in those suffering from vestibular, visual, musculoskeletal, and some neurological problems.
Essential hypertension is a common and fast-growing medical condition in the community where the cause is unknown in the majority and requires in-depth studies to unmask its impact on physiological parameters like body balance. It is known that hypertension contributes substantially to poor physical function and autonomic imbalance. Several studies have evaluated postural stability in elderly and those with vestibular disorders.[3,4] One of the less explored areas is studying the association of essential hypertension with postural stability. Studies on the assessment of static and dynamic balance in hypertensive individuals are limited. Centre of Pressure (CoP) is a commonly used index of postural stability while standing and is a measure of the activity of the motor system. Decreased performance of sensory and motor systems can lead to significant sways in the body, with displacement of CoP indicating the degree of postural instability.[5]
Computerised posturography is a well-established and valid tool to determine postural stability with high test-retest reliability.[6,7] It is also observed that the fall incidence is higher in women than men, which may be due to the postural instability caused by early loss of muscle mass and bone density in women. The study was taken up to see whether the presence of essential hypertension further contributes to postural instability in women and compared with age-matched normotensive controls.
MATERIALS AND METHODS
After obtaining IEC permission (ESICMC/SNR/IEC-F0119/04/2019) and obtaining written informed consent, 40 women attending the General Medicine outpatient department were screened for hypertension, and after applying the inclusion and exclusion criteria, a total of 16 hypertensive women were included in the study. The mean age of the participants was 51.9 ± 9.1 years on regular treatment for hypertension with a similar combination of drugs. The mean duration of hypertension in the study participants was 5.06 ± 2.44 years. Those with neurological disorders with sensory-motor incoordination, secondary hypertension and any other comorbidities like diabetes which affect body balance were excluded from the study. Obese women, those with orthopaedic pathology, back pain, vestibular and other central nervous system disorders and post-stroke individuals were also excluded from the study. Sixteen age-matched normotensive women were included as controls, and all subjects were right-handed. Both pre-and post-menopausal women were included in the study.
A detailed history was obtained, and a general examination was performed. Before testing, participants were instructed to come after having a light breakfast, avoid caffeine and do strenuous exercise for 10 h. Participants were given a briefing to familiarise themselves with the test protocol. They were asked to rest for about 5 min in sitting posture and then instructed to stand on the Nintendo Wii Fit Plus balance board/force plate with dimensions of 50 cm by 30 cm and four balance sensors placed at the corners of the board that make contact with the ground. The board is placed on a stable and even horizontal ground. The surface of the board has a designated area for placement of feet. As per the protocol, participants were asked to remove their shoes and, stand on the balance board with eyes open and look straight at the wall in front at eye level. As per the instructions, participants were asked to sway to the right or left using the ankle strategy while keeping the body straight and following the trial protocol [Figure 1]. At all times, care was taken to observe whether heels and toes were in contact with the force platform. The centre of pressure coordinates were measured and recorded through the LabChart software.
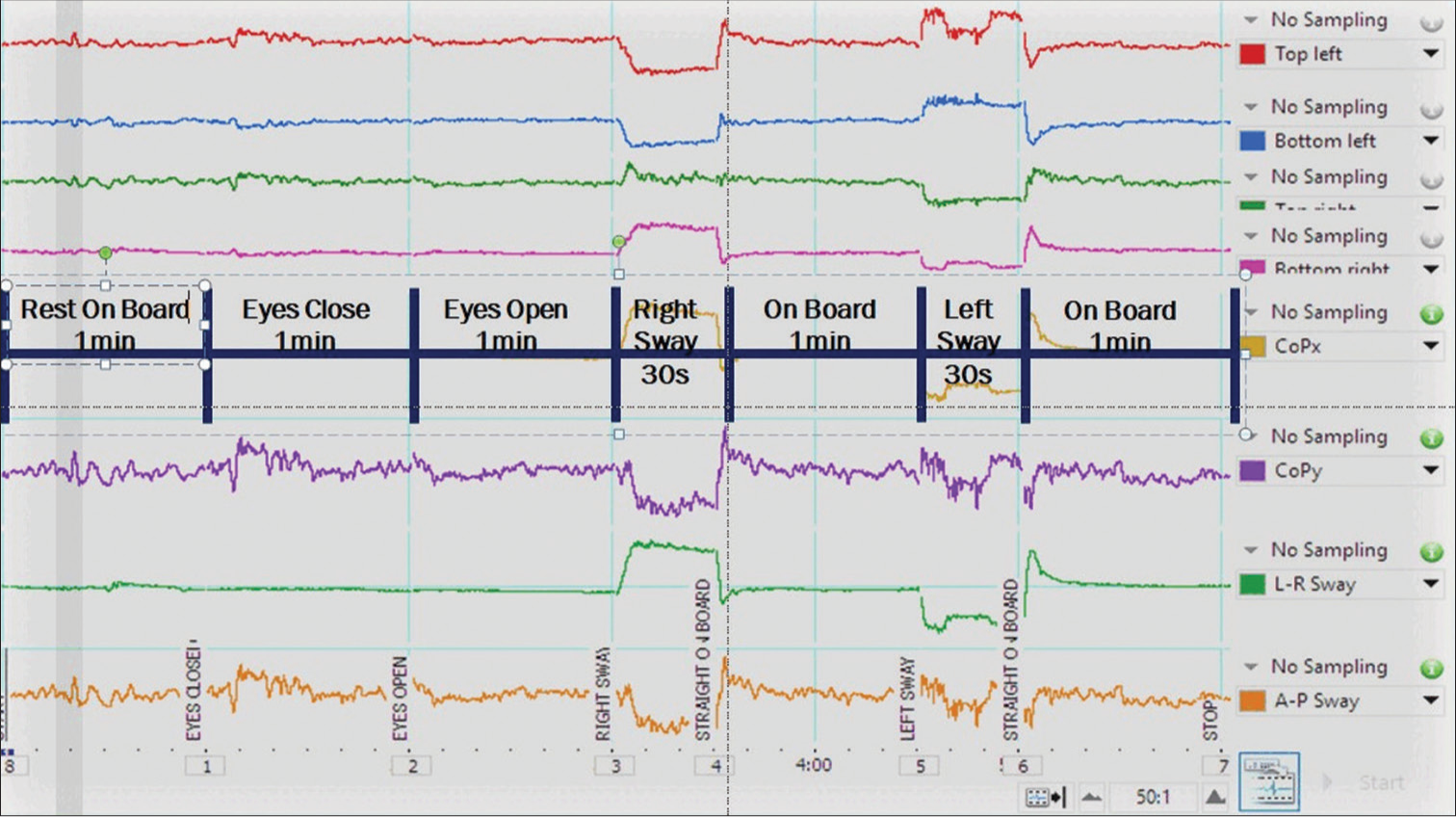
- Trial protocol.
Trial protocol
Rest on the board, standing, with eyes open for 1 min
Close eyes for 1 min
Open eyes for 1 min
Right sway (RS) with eyes open (with body straight using ankle strategy) for 30 s
Rest on the board standing with eyes open for 1 min
Left sway (LS) with eyes open (with body straight using ankle strategy) for 30 s
Rest on the board standing with eyes open for 1 min.
Displacement of CoP in the mediolateral (ML) direction was studied as per the trial. The displacement was measured in centimetres in ML direction with eyes open and eyes closed conditions. The WII balance board was wirelessly connected to PowerLab 8/35 (AD instruments) with LabChart software that was used to measure the parameters.
Statistical analysis
All parameters were subjected to the Shapiro–Wilcoxon test to check for normality. Continuous data were represented as mean ± standard deviation, and categorical variables were represented as percentages. The chi-square test and student “t” test were used to compare the groups. P < 0.05 was considered significant.
RESULTS
The mean duration of hypertension in the subjects was 5.06 ± 2.44 years. The mean value of blood pressure in the hypertensive group was 146.06 mm of Hg systolic and 88.81 mm of Hg diastolic. The mean blood pressure of the non-hypertensive group was 123.44 ± 5.65 mm of Hg systolic and 80.56 ± 5.9 diastolic [Table 1]. Displacement of CoP in the ML direction was studied in the trials and expressed in centimetres. The CoP was measured in eyes closed and eyes open conditions. After initial resting for 1 min, in eyes closed position, the CoP was found to be displaced in both groups, with significant displacement in hypertensive women [Table 2].
| Parameter | Hypertensive women (n=16) | Normotensive women (n=16) | P-value |
|---|---|---|---|
| Systolic blood pressure | 146.06±14.9 | 123.44±5.65 | <0.0001 |
| Diastolic blood pressure | 88.81±8.3 | 80.56±5.9 | 0.0029 |
| Mean arterial pressure | 107.9±9.8 | 94.85±5.3 | 0.0001 |
| Trial | Hypertensive women (n=16) | Normotensive women (n=16) | P-value |
|---|---|---|---|
| dCoP EC (cms) | 0.189±0.58 | 0.051±0.37 | 0.9340 |
| dCoP EO (cms) | 0.063±0.44 | 0.004±0.61 | 0.3863 |
EC: Displacement from the resting state to eyes closed for 1 min, EO: Displacement from the resting state to eyes open for 1 min, dCoP: Desired centre of pressure
When the subjects were instructed to sway voluntarily to their right and left sides, hypertensive women showed significantly less sway displacement compared to normotensive women [Table 3]. On swaying in ML direction to either right or left sides and in the process of returning to the initial position, it was observed that some subjects exhibited either over-correction or under-correction. In hypertensives, during RS, under-correction and error of correction were more compared to normotensives with 13% error [Figure 2]. Although the percentage of subjects showing overcorrection during RS was less compared to normotensives, the degree of overcorrection was higher in them (35%). During LS, only hypertensive subjects have shown under-correction with an error of 7.9% [Figure 3]. Overcorrection during LS was high in both hypertensive and normotensive, showing a significant difference [Tables 4 and 5]. Another interesting observation was the significant (P = 0.009) difference in the error of correction between right and LSs within the hypertensive group with more over-correction during LS [Table 5].
| Trial | Hypertensive women (n=16) | Normotensive women (n=16) | P-value |
|---|---|---|---|
| RS (cms) | 7.53±3.6 | 10.95±1.6 | 0.0015* |
| LS (cms) | 7.44±4.5 | 10.12±1.2 | 0.0284* |
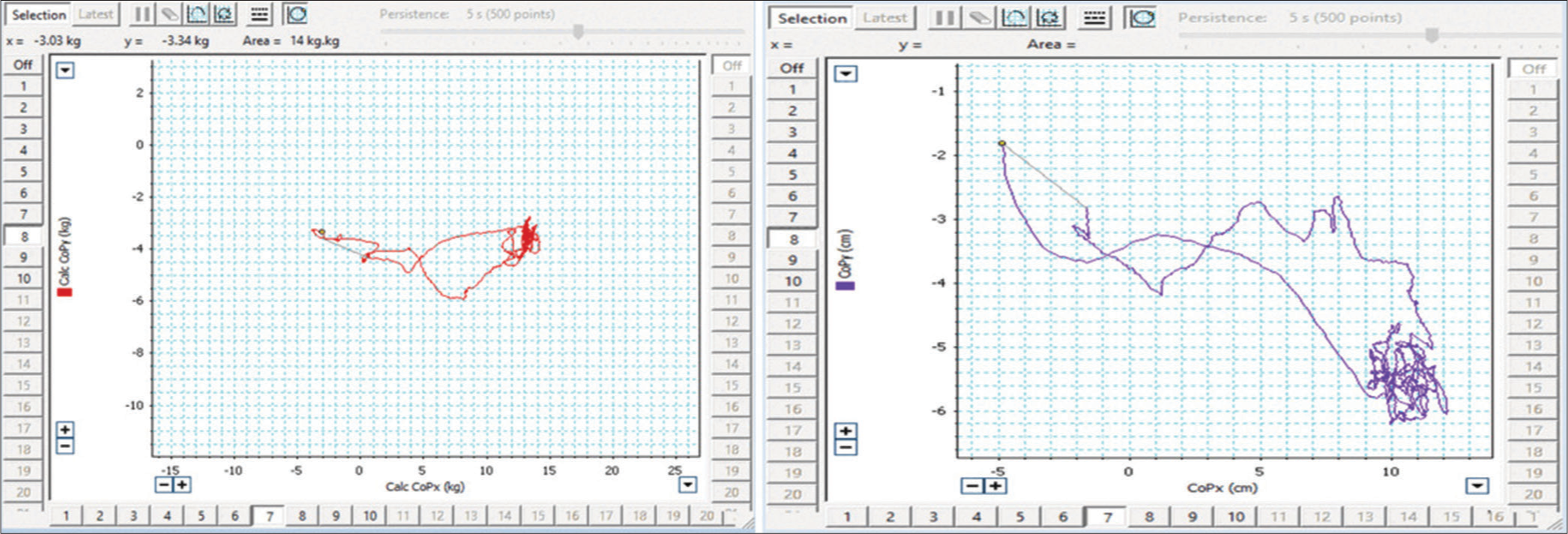
- Comparison of XY plot of Anteroposterior – mediolateral sway between normotensive (left) and hypertensive (right) during right sway.
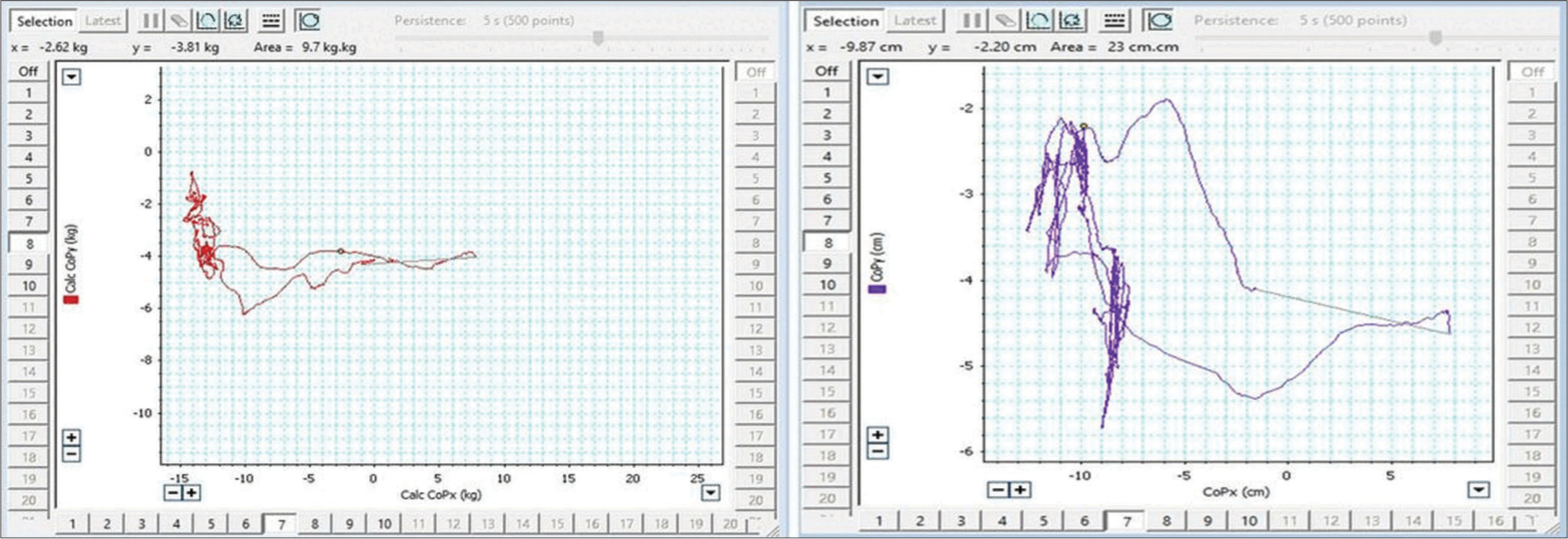
- Comparison of XY plot of Anteroposterior – mediolateral sway between normotensive (left) and hypertensive (right) during left sway.
| Trial | Correction in hypertensive women (n=16) | Correction in normotensive women (n=16) | P-value | ||
|---|---|---|---|---|---|
| RS | Over correction n=7 | Under correction n=9 | Over correction n=12 | Under correction n=4 | 0.1489 |
| LS | Over correction n=11 | Under correction n=5 | Over correction n=16 | Under correction n=0 | 0.04* |
| Trial | % error in correction in hypertensive women (n=16) |
% error in correction in normotensive women (n=16) |
P-value | ||
|---|---|---|---|---|---|
| Over correction | Under correction | Over correction | Under correction | ||
| RS % correction | 35 | 13 | 16 | 4.7 | 0.999 |
| LS % correction | 74 | 7.9 | 20 | 0 | 0.332 |
| 0.009* | 0.066 | ||||
DISCUSSION
Postural control mechanisms operate in a regulated manner with inputs from muscle afferents, vestibular apparatus, and peripheral somatosensory and visual receptors.[8,9] In general, the signals from the proprioceptive receptors get weaker with ageing, and hence, the elderly are prone to frequent falls.[10] The excursions in CoP in these individuals can be attributed to several factors, such as neurological, orthostatic hypotension or pain associated with the musculoskeletal system.[11,12] While parameters such as height, weight and resting heart rate may affect stability, the present study was taken up as a pilot study and was limited to seeing the effect of blood pressure alone on postural stability.
Postural sways are small micro-movements that happen around the CoP and often go unnoticed. Normally, the body and the brain try to correct these sways with the help of inputs from visual and proprioceptive pathways. Further, these sways are sometimes corrected even without the visual inputs. Instability in posture may not be expected if a person is congenitally blind, as the other proprioceptive mechanisms are strengthened in them. In people who become blind later in life, such instability may be expected if there is hypertension. The present study measured the displacement in a neutral position by eliminating the visual inputs to the body by asking the subjects to stand on the Wii board with their eyes closed. It was observed in the study that there was an increased CoP displacement in hypertensive subjects as compared to normotensives in eyes closed condition, probably due to the weakening proprioceptive inputs caused by hypertension per se. Animal studies on hypertensive rats have shown evidence of axonal atrophy along with slowing of nerve conduction suggestive of neuropathy.[13] During voluntary sways in the ML direction, normotensives somewhat regained their initial CoP position, but hypertensives have shown exaggerated displacement in the opposite direction. This could probably be because hypertensive individuals are anxious about falls due to adrenergic overdrive, and in anticipation, they possibly tend to overcorrect. Tinetti et al. have reported an increased incidence of falls in hypertensives who are on antihypertensive medications.[14] Falls in hypertensives are more common with polypharmacy treatment and in those on diuretics but are not associated with the number of antihypertensive medications.[15] Another study reported that increased blood pressure reduced the risk of falls in women, and reduced blood pressure increased the risk in men, which was due to postural hypotension.[16] The study attributes displacement of CoP and corrections during sways to neural involvement in hypertension, as evidenced by previous studies. In this study, it is observed that hypertensive women had a significant amount of overcorrection to bring their CoP back to resting state from the sway position. Anteroposterior sways are common in normal, healthy individuals, and inherent postural control mechanisms alter ankle stability. Lateral sways, in contrast, are not ‘natural’ and require more of anticipatory postural correction mechanisms.[17] In the present study, the degree of overcorrection was found to be much more than the degree of under correction and the overcorrection is by far even greater in LS. The greater degree of overcorrection in LSs is a normal phenomenon for a right-footed person, and this is further exaggerated in hypertensive subjects. This overcorrection might be a response to postural anxiety as they have increased apprehension of falling. In the context of elevated postural anxiety and postural danger induced by standing at the edge of a raised platform, healthy volunteers have shown diminished spinal reflex excitability.[18]
Reduced pain perception and sensitivity have been linked to hypertension.[19,20] Pain causes increased presynaptic inhibition of muscle afferents with prolonged latencies, causing decreased muscle control and increased postural sway.[21] This has been further proved by Ruhe et al. as there is a decreased postural sway in pain relief of chronic back pain patients.[22] On the other hand, Ruhe et al. have also observed that pain intensity is directly related to the amount of sway.[23]
One can attribute dysautonomia as a cause for postural instability in hypertensives and is associated with reduced heart rate variability.[24] Furthermore, postural instability in Parkinson’s disease is associated with parasympathetic autonomic dysfunction.[25] It has been observed that cardiac dysautonomia and adrenergic overdrive have a greater role in the development and progression of essential hypertension. [26,27] This can also be ascribed to overall increased vigilance and, hence excitable state of neural networks involved in postural control. Hyperactive postural control mechanisms may be operating in hypertensives, which by far go unnoticed and become explicit by doing such trials. Together, it can be said that the postural control mechanisms, reflexes and anticipatory signals from the cortex are more pronounced in hypertensives, along with the element of dysautonomia to produce postural instability.
Balance measures to study postural stability in hypertensives can keep the individual, the caretaker and the attending physician informed and identify those at risk of falling so as to take necessary and timely corrective steps. Balance training exercises for such individuals can improve their stability.[6] Real-time measurements will serve as a biofeedback module to acquaint the individual with the changing postural stability patterns, and regular use as an intervention can help in training the body to maintain balance. The availability of low-power and wearable sensor devices can characterise lateral sway and gait metrics and provide corrective feedback in real-time through vibratory feedback modules.[28] A variety of non-invasive self-motion signals are provided by unimodal and multimodal feedback displays, such as vibrotactile electric tongue currents, audio and combinations of visual, vibrotactile and auditory cues.[29] There is also evidence of training sessions using a sensory augmentation device producing substantial gain in balance performance.[30] Hence, the treating physician may investigate these possibilities while treating postural instability in hypertensives.
Limitations
The sample size was small as the authors performed a pilot study to see the effect of hypertension on balance. A larger sample with more variables, including measurement of autonomic activity, might provide more information for similar studies in future.
CONCLUSION
Postural instability is present in hypertensive individuals. Posturography can be used as a routine screening test to predict postural instability in hypertensives. Balance training exercise feedback protocols and use of sensory augmentation devices may prove to be useful in improving postural stability.
Ethical approval
The research/study was approved by the Institutional Ethics Committee at ESIC Medical College, Sanathnagar, Hyderabad, number ESICMC/SNR/IEC-F0119/04/2019, dated 15 April 2019.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Sensorimotor manipulations of the balance control loop-beyond imposed external perturbations. Front Neurol. 2018;9:899.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of a multifactorial intervention for dizziness in older people in primary care: A cluster randomised controlled trial. PLOS One. 2018;13:e0204876.
- [CrossRef] [PubMed] [Google Scholar]
- Disorders of balance and vestibular function in US adults: Data from the National Health and Nutrition Examination Survey, 2001-2004. Arch Intern Med. 2009;169:938-44.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of dizziness on everyday life in older primary care patients: A cross-sectional study. Health Qual Life Outcomes. 2011;9:44.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative posturography in altered sensory conditions: A way to assess balance instability in patients with chronic whiplash injury. Arch Phys Med Rehabil. 2004;85:432-8.
- [CrossRef] [PubMed] [Google Scholar]
- Results of a 10 week community based strength and balance training programme to reduce fall risk factors: A randomised controlled trial in 65-75 year old women with osteoporosis. Br J Sports Med. 2001;35:348-51.
- [CrossRef] [PubMed] [Google Scholar]
- Validity and reliability of limits-of-stability testing: A comparison of 2 postural stability evaluation devices. J Athl Train. 2011;46:600-6.
- [CrossRef] [PubMed] [Google Scholar]
- Human upright posture control models based on multisensory inputs; in fast and slow dynamics. Neurosci Res. 2016;104:96-104.
- [CrossRef] [PubMed] [Google Scholar]
- The proprioceptive senses: Their roles in signaling body shape, body position and movement, and muscle force. Physiol Rev. 2012;92:1651-97.
- [CrossRef] [PubMed] [Google Scholar]
- The importance and role of proprioception in the elderly: A short review. Mater Sociomed. 2019;31:219-21.
- [CrossRef] [PubMed] [Google Scholar]
- Mechanisms underlying center of pressure displacements in obese subjects during quiet stance. J Neuroeng Rehabil. 2011;8:20.
- [CrossRef] [PubMed] [Google Scholar]
- Center of pressure excursion as a measure of balance performance in patients with non-specific low back pain compared to healthy controls: A systematic review of the literature. Eur Spine J. 2011;20:358-68.
- [CrossRef] [PubMed] [Google Scholar]
- Hypertension-induced peripheral neuropathy and the combined effects of hypertension and diabetes on nerve structure and function in rats. Acta Neuropathol. 2012;124:561-73.
- [CrossRef] [PubMed] [Google Scholar]
- Antihypertensive medications and serious fall injuries in a nationally representative sample of older adults. JAMA Intern Med. 2014;174:588-95.
- [CrossRef] [PubMed] [Google Scholar]
- Older adults with hypertension: Prevalence of falls and their associated factors. Int J Environ Res Public Health. 2021;18:8257.
- [CrossRef] [PubMed] [Google Scholar]
- Blood pressure and falls in community-dwelling people aged 60 years and older in the VHM and PP cohort. BMC Geriatr. 2013;13:50.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in postural sway and its fractions in conditions of postural instability. J Appl Biomech. 2006;22:51-60.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of postural anxiety on the soleus H-reflex. Hum Mov Sci. 2007;26:103-12.
- [CrossRef] [PubMed] [Google Scholar]
- Hypoalgesia associated with elevated resting blood pressure: evidence for endogenous opioid involvement. J Behav Med. 2010;33:168-16.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between resting blood pressure and acute pain sensitivity in healthy normotensives and chronic back pain sufferers: The effects of opioid blockade. Pain. 2002;100:191-201.
- [CrossRef] [PubMed] [Google Scholar]
- Experimental muscle pain produces central modulation of proprioceptive signals arising from jaw muscle spindles. Pain. 2000;86:151-62.
- [CrossRef] [PubMed] [Google Scholar]
- Pain relief is associated with decreasing postural sway in patients with non-specific low back pain. BMC Musculoskelet Disord. 2012;13:39.
- [CrossRef] [PubMed] [Google Scholar]
- Is there a relationship between pain intensity and postural sway in patients with non-specific low back pain? BMC Musculoskelet Disord. 2011;12:162.
- [CrossRef] [PubMed] [Google Scholar]
- Reduced heart rate variability and new-onset hypertension: Insights into pathogenesis of hypertension: The Framingham Heart Study. Hypertension. 1998;32:293-7.
- [CrossRef] [PubMed] [Google Scholar]
- Association of postural instability with autonomic dysfunction in early Parkinson's disease. J Clin Med. 2020;9:3786.
- [CrossRef] [PubMed] [Google Scholar]
- Autonomic dysfunction in essential hypertension: A systematic review. Ann Med Surg (Lond). 2013;3:2-7.
- [CrossRef] [PubMed] [Google Scholar]
- The autonomic nervous system and hypertension. Circ Res. 2014;114:1804-14.
- [CrossRef] [PubMed] [Google Scholar]
- The impact of vibrotactile biofeedback on the excessive walking sway and the postural control in elderly. Proc Wirel Health. 2013;2013:3.
- [CrossRef] [PubMed] [Google Scholar]
- Channeling of brain towards engaging sensorimotor tasks for inducing hedonic pleasure to alleviate blood pressure in hypertension. Ann Neurosci. 2023;30:109-18.
- [CrossRef] [PubMed] [Google Scholar]
- The role of sensory augmentation for people with vestibular deficits: Real-time balance aid and/or rehabilitation device? J Vestib Res. 2017;27:63-76.
- [CrossRef] [PubMed] [Google Scholar]




