
Translate this page into:
Alignment and integration in competency-based medical education curriculum: An overview
*Corresponding author: Minal Patel, Department of Physiology, Pramukhswami Medical College, Karamsad, Anand -388 325, Gujarat, India. drminalpatel78@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Patel M, Shah HD. Alignment and integration in competency-based medical education curriculum: An overview. Indian J Physiol Pharmacol 2020;64(Suppl_1):S13-S5.
INTRODUCTION
Alignment is the components of same organ system or a disease when taught concurrently at the same phase but under different subjects. Integration means blending various components of a single topic/organ system that is similar, overlapping or redundant which is otherwise taught under different subjects in same, or different phases, thus, subject based demarcation is lost.[1] In medical education, integration plays very important role as learning of basic science is in context to clinical education so that it becomes more relevant and meaningful to the students. Subject-based teaching gives broad and deep knowledge of each subject to the students. The unique needs of medical education necessitate both an understanding of interconnectedness between subjects and their application to the patient. For optimum patient care contribution of various departments is essential, a sort of integrated care toward patient. Unless we train our students that way right from the beginning, it may be difficult for them to accept it later on. Therefore, to remove repetitions and help students to see and understand interconnectedness among various disciplines of medicine, alignment and integration is required in competency-based medical education (CBME) curriculum.[1] It provides the students with a holistic rather than a fragmented learning perspective by de-emphasising compartmentalisation of the disciplines. Integration promotes students comprehensive understanding, rationalize redundancy and reinforcement materials, student involvement and motivation skyrockets as they can see interconnectedness and inter-relationships among disciplines, provide context and relevance when introduced in early stage of MBBS course and reinforce biomedical basis of clinical concepts when practiced in later stage.
DIFFERENT LEVELS OF INTEGRATION RECOGNISED GLOBALLY
Based on the work of Jacobs, Fogarty and Drake, integration ladder was created by Harden[2] which has 11 steps from subject-based to integrated teaching and learning. The steps on ladder from below upward are isolation, awareness, harmonisation, nesting, temporal coordination, sharing, correlation, complementary, multi-disciplinary, inter-disciplinary and trans-disciplinary. Harden describe integration ladder as, subject-based teaching (isolation) at the bottom of the ladder and full integration (trans-disciplinary teaching) at the top. The emphasis is on the subjects or disciplines in the first four steps on the ladder, the following six steps emphasize integration across several disciplines. The student takes more responsibility for the integration and is given tools to do so in the last step of the ladder.
As per GMER 2019 MCI recommends Temporal Coordination (as much as possible) and Nesting, Sharing and Correlation: up to 20% of subject contents[1] [Figure 1].
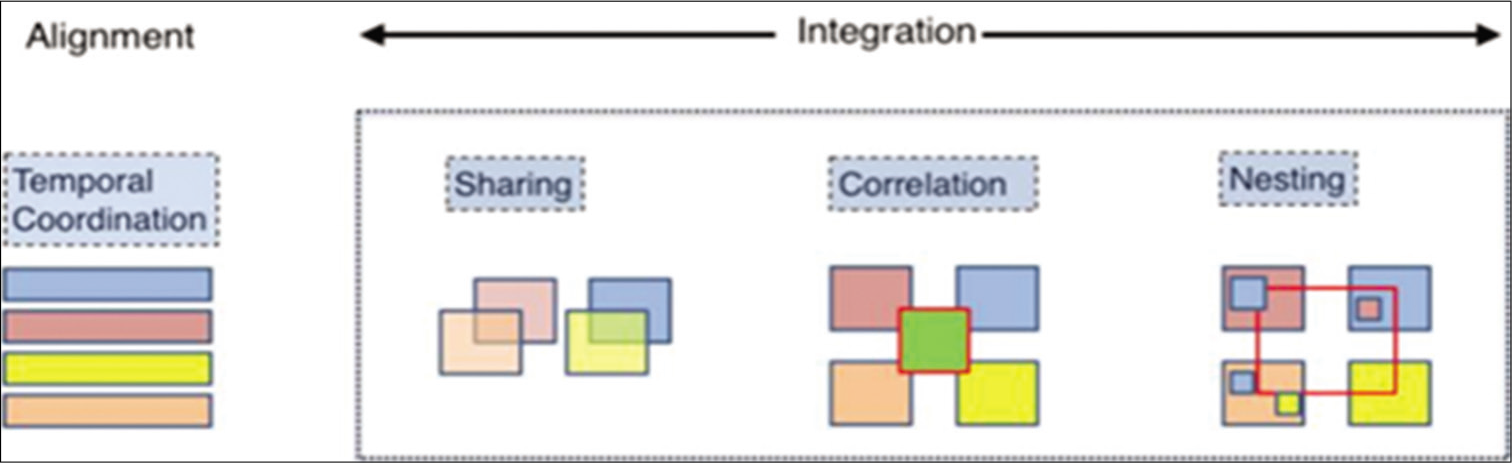
- Represents the concept of alignment and integration.
Integration in practice would be at two planes:[1] Horizontal and vertical. Horizontal integration (within a phase) brings together the disciplines, topic and subject, removes redundancy and provides interconnectedness in the disciplines of the same phase. Vertical integration (across phases) brings together basic and clinical sciences. In the earlier phase, it shows importance of basic science in relation to clinical aspects while in latter phase purpose of vertical integration is to use prior knowledge of basic science for clinical practice. Thus, horizontal integration is across the subjects in a given phase and vertical integration is across different phases of the course. This means, the learning become more meaningful and relevant to the students by learning the basic science in context of clinical and professional practice [Figure 2].[1]
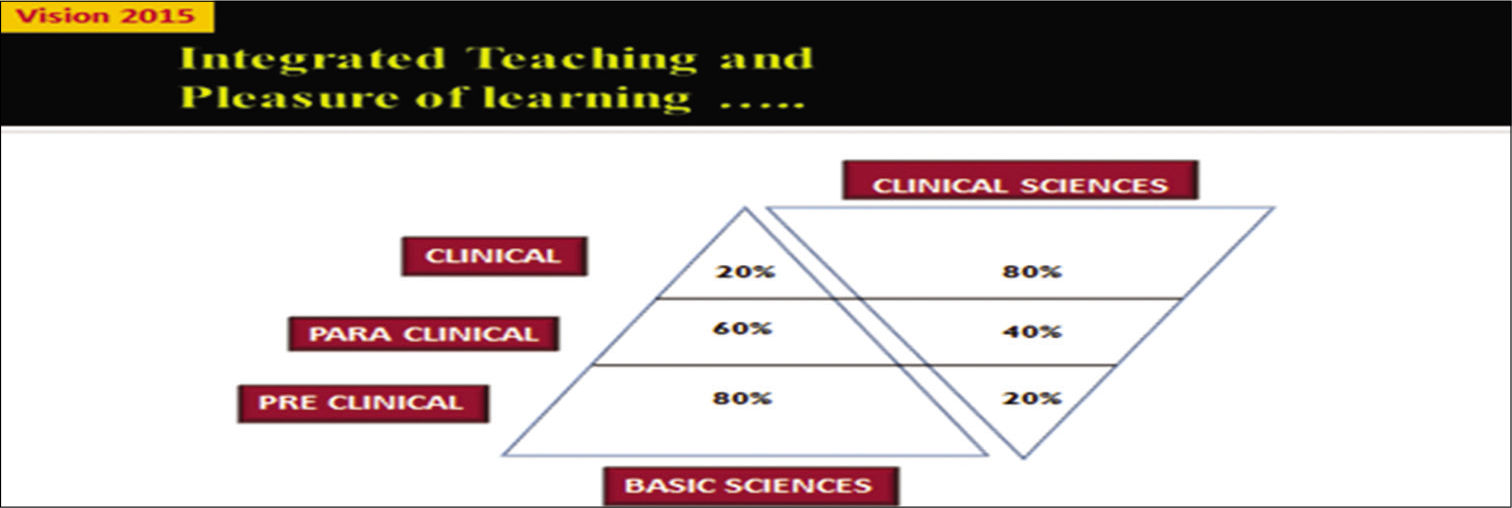
- Represents the importance of integration.
ADVANTAGES AND BENEFITS OF INTEGRATED TEACHING
Curriculum integration provides students to understand a whole view of the curriculum to broaden the context of their learning beyond single subject areas. Learning the connections among subject areas help students to build on their diverse prior knowledge and experiences, supports their holistic view and ensures deep and meaningful learning. It helps students to perceive the interconnectedness and inter-relationships among disciplines. The integration not only provides a deeper understanding of content but also encourages active participation in relevant real-life experiences and finally provides connections among various curricular disciplines. It reduces overlap, repetition and redundancy, thus making effective use of the academic calendar. It is not only beneficial to the students but also for various disciplines, as by planning integrated session interdisciplinary working coordination and communication can be improved.[1,3]
ANTICIPATED CHALLENGES IN ADOPTING AND IMPLEMENTATION OF INTEGRATED TEACHING IN CBME CURRICULUM
Like any other technique and process, the concept of integration is bound to meet several challenges and impediments in its acceptance and implementation. One of the challenges is lack of trained faculty. Teaching-learning and assessment methods proposed under CBME will require training of the faculty across the India. Motivation of the faculty is also important challenge, as many of the faculty are not interested and even, they do not bother to learn the ideal conventional TL methods. It is very difficult to change the mind-set of faculty to accept intrusion of another department into their domain. Even tendency of many faculty to resist change and lack of confidence in moving out of the comfort zone of their traditional teaching methodology. Although, alignment and integration are ideal on paper, are difficult to implement due to different weightage, time allotments of various subjects. Lack of proper interdisciplinary coordination leads to difficulty in framing a time-table for integrated teaching sessions. There is a need of coordination between various regulatory stakeholders to facilitate faculty development programs and to create learning environments for smooth implementation of CBME. Emphasis on formative assessment is given in CBME curriculum, so arranging frequent formative and internal assessment are another major challenge. In CBME, curriculum passive learning is replaced by active learning where more emphasis is given on self-directed learning and skill trainings. To engage the students in all these activities resources are required. Hence, there may be certain hurdles in setting up an appropriate infrastructure for its implementation. Therefore, in CBME curriculum for a better implementation of integrated teaching all leaders, medical educators and decision makers need collaborative approaches to common challenges.[4]
ASSESSMENT IN CBME CURRICULUM
In CBME, assessment is an important component of curriculum at par with learning objectives and learning process. Assessment should be planned after framing learning objective but, precede designing of teaching-learning method. Planning assessment before the session will help to design learning sessions and not only that but it also help to modify the leaning objectives.[5] The assessment will be subject based but to test whether the learner has internalised and integrated the concept phase appropriate clinical relevance will be assessed during examination.[1] It is blended assessment which assesses knowledge, skills and soft skills mostly embedded within competency, so assessing integrative aspects of multiple modules. It is longitudinal that is formative/assessment for learning as well as summative assessment in contrast to traditional assessment which mainly focuses on summative assessment. Feedback is an important component of formative assessment in integrated assessment in CBME curriculum.[1] Hence, integrated assessment in CBME curriculum is clinically relevant and health-care scenario centric. There are different integrated assessment techniques[6] such as performance assessment, systematic observations, portfolios, criterion referenced assessment for students pursuing integrated curriculum and authentic assessment is based on combination of all these techniques.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Alignment and Integration Module for Undergraduate Medical Education Program New Delhi: Medical Council of India; 2019.
- [Google Scholar]
- The integration ladder: A tool for curriculum planning and evaluation. Med Educ. 2000;34:551-7.
- [CrossRef] [PubMed] [Google Scholar]
- Integrated medical curriculum: Advantages and disadvantages. J Med Educ Curric Dev. 2016;3:S18920.
- [CrossRef] [PubMed] [Google Scholar]
- Moving toward competency-based education: Challenges and the way forward. Arch Med Heal Sci. 2014;2:247-53.
- [CrossRef] [Google Scholar]




