
Translate this page into:
Teaching framework of basic sciences in medical curriculum: A literature review

*Corresponding author: Dinesh Kumar Badyal, Department of Pharmacology and Medical Education, Christian Medical College, Ludhiana, Punjab, India. dineshbadyal@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Badyal DK. Teaching framework of basic sciences in medical curriculum: A literature review. Indian J Physiol Pharmacol. 2023;67:310-20. doi: 10.25259/IJPP_266_2023
Abstract
Objectives:
The quantity, quantity, and timing of basic sciences teaching in the context of clinical learning have been a debatable issue for a long time. Therefore, this study was planned to evaluate the teaching framework of basic sciences in undergraduate medical education.
Materials and Methods:
The publications were collected through online searches according to predefined inclusion and exclusion criteria. Three reviewers analysed the data and arrived at a conclusion to select 90 publications. These publications were analysed thoroughly to classify them into ten categories of basic sciences teaching frameworks. Content analysis of these publications was done for comparison across publications.
Results:
The reviewer’s rate of agreement for their conclusions varied between 89 and 94% for different phases of analysis. The most common category was ‘Integration’ (29%), followed by ‘Problem-based/Case base learning’ (18%) and ‘Mixed-methods approach’ (14%). The strategies being used in basic sciences teaching were mostly learner centred (68.9%).
Conclusion:
The review of basic sciences teaching frameworks in our study indicates that various frameworks of basic sciences teaching are being used in various medical schools throughout the world. The pattern of these frameworks can contribute to effective policy-making for improving basic sciences teaching.
Keywords
Basic science teaching
Clinical sciences teaching
Medical education

INTRODUCTION
Basic sciences have long formed the major part of the first 2 years of the undergraduate (UG) medical curriculum and have been taught predominantly by basic sciences faculty in some countries and clinical sciences faculty in other countries.[1,2] The Flexner report paved the way for the formulation of this traditional approach for teaching basic sciences in the initial 1–2 years followed by clinical science teaching.[2] This concept might have been relevant at that time as explained by the cognitivism theory of learning where the learner adds knowledge to their existing knowledge.[3]
However, there is renewed interest in optimizing basic science teaching to maximise its utility for learning clinical science.[1] This led to modifications of basic sciences teaching frameworks in UG medical curriculum in various countries at different times.
Several investigators have tried various interventions in basic sciences teaching based on various principles and theories. These experimentations include problem-based learning (PBL), integration of basic and clinical sciences, simulations/e-learning, computer-assisted learning (CAL), trimming or cutting down of content, and decreasing the time allocated for basic sciences in the first 2 years of a course.[2,4-8]
These changes in the quality and/or quantity of basic sciences teaching have been variable and debatable, especially from the point of view of basic sciences and clinical sciences faculty.[9-12] However, it is accepted by all that a foundation in basic sciences is important for applying scientific concepts to clinical situations.[10]
The information about the framework of basic sciences teaching, how it is being taught, methods used and innovations tried will help other countries like India, where there are further modifications of basic sciences.[13]
The research questions framed were as follows:
What are the most effective frameworks of basic sciences teaching to optimise clinical sciences teaching? and
Can a research agenda be set by analysing these frameworks of basic sciences teaching to optimise clinical science teaching in the UG medical curriculum?
Therefore, this study was designed to review the current literature and its categorisation as per the nature of frameworks of basic sciences teaching in the UG medical curriculum.
MATERIALS AND METHODS
In our study, we included basic sciences according to the world federation of medical education (WFME) definition, that is, ‘anatomy, biochemistry, biophysics, cell biology, genetics, immunology, microbiology (including bacteriology, parasitology, and virology), molecular biology, pathology, pharmacology and physiology depending on local needs, interests, and traditions.’[14] We looked at those articles that included any of the above topics.
The free-text search was used to capture all potentially relevant articles. There were online searches using various sources based on the literature review. Keywords were used to add uniformity [Table 1]. Initial screening was based on titles/abstracts and was done as per our research questions and the study design. The full-length articles were obtained. The year of publication of articles ranged from 1994 up to 2017. During the second reading of articles, the relevant cross-references were searched using manual search and these publications were screened by applying inclusion and exclusion criteria.
| Basic science | AND teaching | AND modifications | OR integration |
|---|---|---|---|
| OR preclinical | OR methods OR education OR learning OR retention |
OR reforms OR innovations OR trends OR changes OR modernisation OR downsizing OR impact |
OR early clinical exposure OR e-learning OR simulations OR problem-based OR case-based OR computer-assisted OR mixed methods OR clinical reasoning OR diagnosis |
Inclusion and exclusion criteria
Research, review, and/or innovative articles on various forms of basic sciences teaching frameworks in the context of clinical science teaching; research articles or review articles on potential/reported impact of basic sciences teaching frameworks on clinical sciences teaching and publications available as full-length articles were included in the search.
Articles in languages other than English and articles that reported only a minimal detail of their underlying basic sciences teaching framework were excluded from the study.
Data analysis
A qualitative analysis of data was done and consisted of three stages as described below:
Stage 1
The articles were thoroughly studied and analysed as per inclusion and exclusion criteria. The selection of articles was subjected to a second scrutiny by two independent researchers in medical education. The conclusions agreement rate of the three reviewers was 93% in their accepted list of key publications, which is within acceptable reliability agreement limits.[15] The process is depicted in [Figure 1].
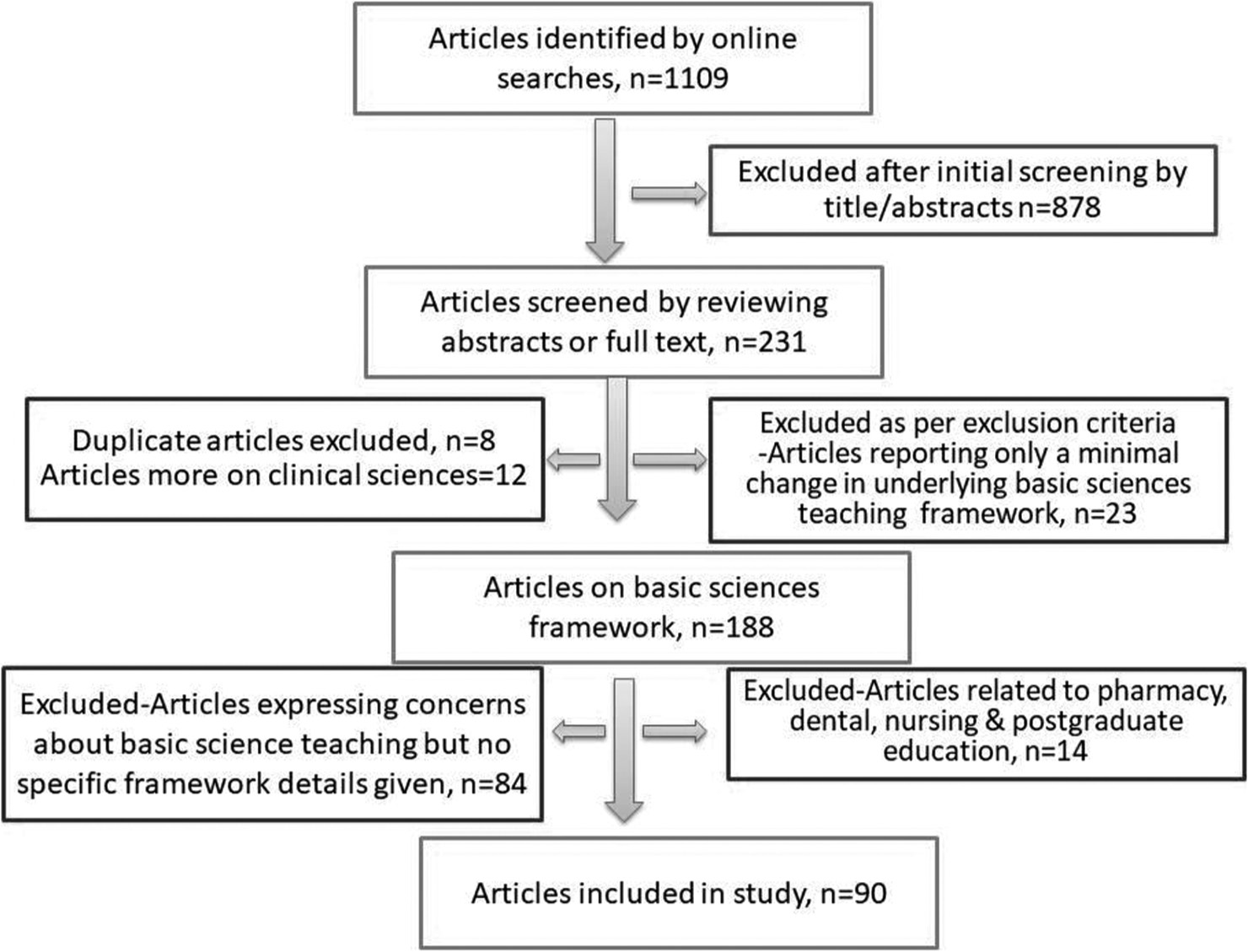
- The process of selecting publications. (n=90), n: number
Stage 2
The refined list of publications was categorised according to the underlying framework by which the basic sciences were taught. This process was carried out by two independent researchers and the principal author. Subsequent discussion of points of difference enabled an agreed list of ten educational frameworks to be identified [Table 2]. The validation of the selection of categories was done by reading the same publications by the principal author and two independent reviewers. The three reviewer’s agreement rate of conclusions was 89%, which is considered to provide adequate reliability for the process.[15]
| Category (%) | Teaching framework |
|---|---|
| ECE (5%) | Use of SPs, meeting patients on day 1 of course |
| Integrated (29%) | Vertical integration/reinforcement in the final year, integration of e-learning, integration of cognitive skills, intellectual skills, and PBL, integration of social sciences, multidisciplinary, 18-month integrated module, concept mapping, short home works |
| CBME (3%) | Competencies developed, integration at all levels |
| PBL/CBL (18%) | The pairing of basic science and clinical science faculty, shared teaching strategy, use of IT, transfer of learning |
| Simulation-based (6%) | High-fidelity mannequins, full-body mannequins, anaesthesia use in pharmacology, care of asthmatic |
| eLearning/CAL (6%) | Dissection and computer-aided teaching; cases with digital images, movies |
| TBL/Active learning (1%) | Presentations, lectures, posters, and blogs by students |
| Contextual/clinical reasoning (8%) | Deep learning, analysis of prescription, 5-step evidence-based, causal relationships added, reduction in year 1 duration, clinical duration increased |
| Traditional (10%) | Didactic lectures, practical/clinical classes |
| Mixed (14%) | Overview lecture followed by PBL, Didactic lectures topped up with PBL/CBL |
SP: Standardised patients, PBL: Problem-based learning, CBME: Competency-based medical education, CAL: Computer-assisted learning, IT: Information technology, TBL: Team-based learning, CBL: Case-based learning, ECE: Early clinical experience
Stage 3
Content analysis was done to arrive at a set of factors that could further characterise the framework for basic sciences teaching and provide some parameters to help define the context of each publication and provide a means of comparison across the whole list of 90 publications.[15] After many iterations, a stable set of factors emerged. To ensure reliability, a sample of 20% of the publications was independently coded with a reliability of 94, which was well within acceptable levels.[15] A further sample of 20% was recoded by the researcher to ensure internal consistency. The underlying teaching frameworks are listed in [Table 2].
Statistical analysis
The data in our study are depicted in percentages and numbers. We used the agreement formula to evaluate the agreement of conclusions between reviewers.[15] Student’s t-test was used to compare pre-and post-intervention test scores. statistical package for the social sciences (SPSS) version 21.0 was used for descriptive frequency analysis and t-test.
RESULTS
Several articles were excluded after the initial screening of titles, as shown in [Figure 1]. The selected articles were from 23 countries [Figure 2]. Most of the studies were from the USA (30%), followed by India (13%) and the UK (8%). The maximum number of studies are from the years 2007 and 2016 (11.1% each). The year of publication of articles ranged from 1994 up to 2017 [Figure 3].
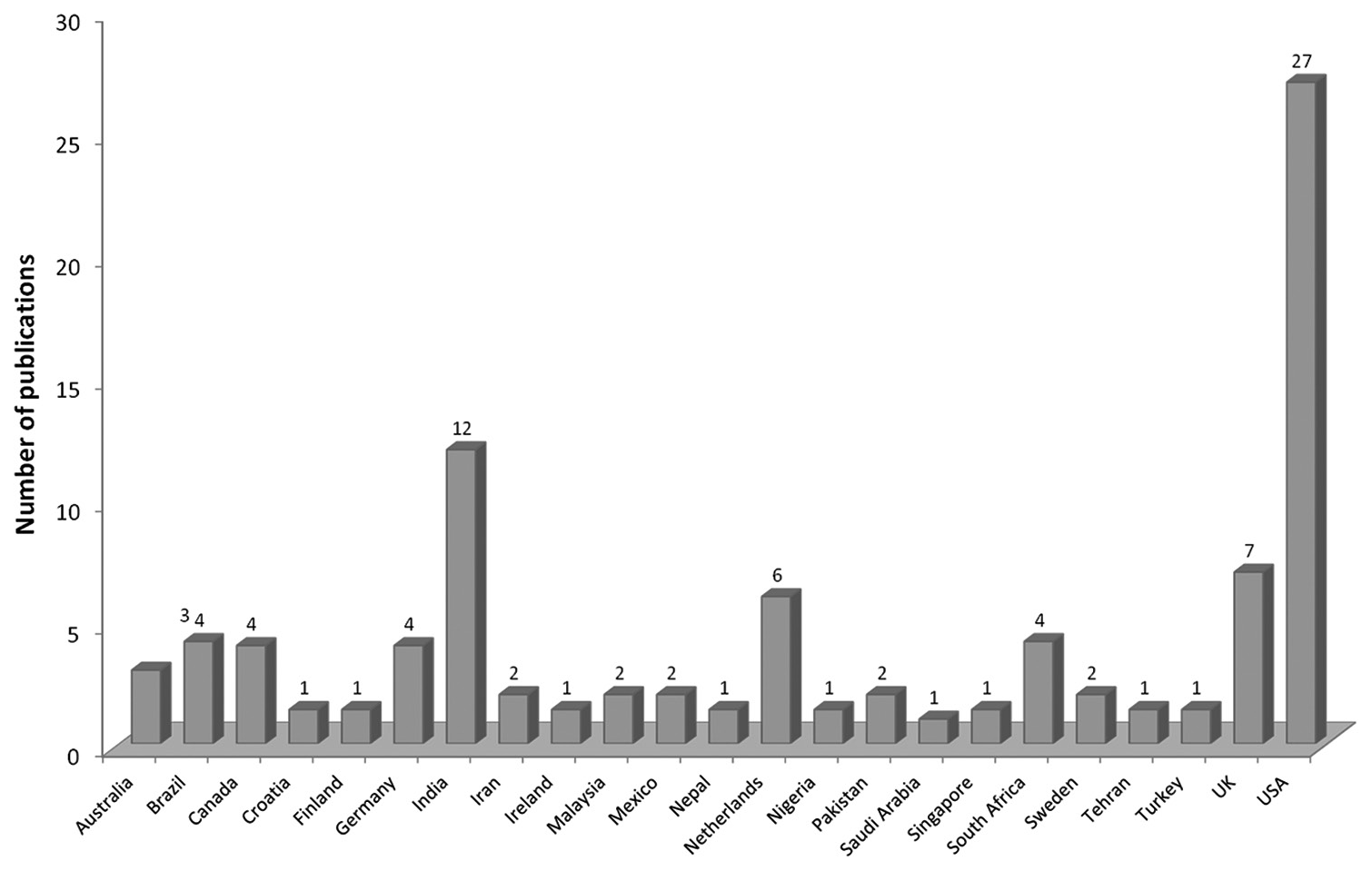
- Country-wise distribution of publications (n=90), UK: United Kingdom, USA: United States of America
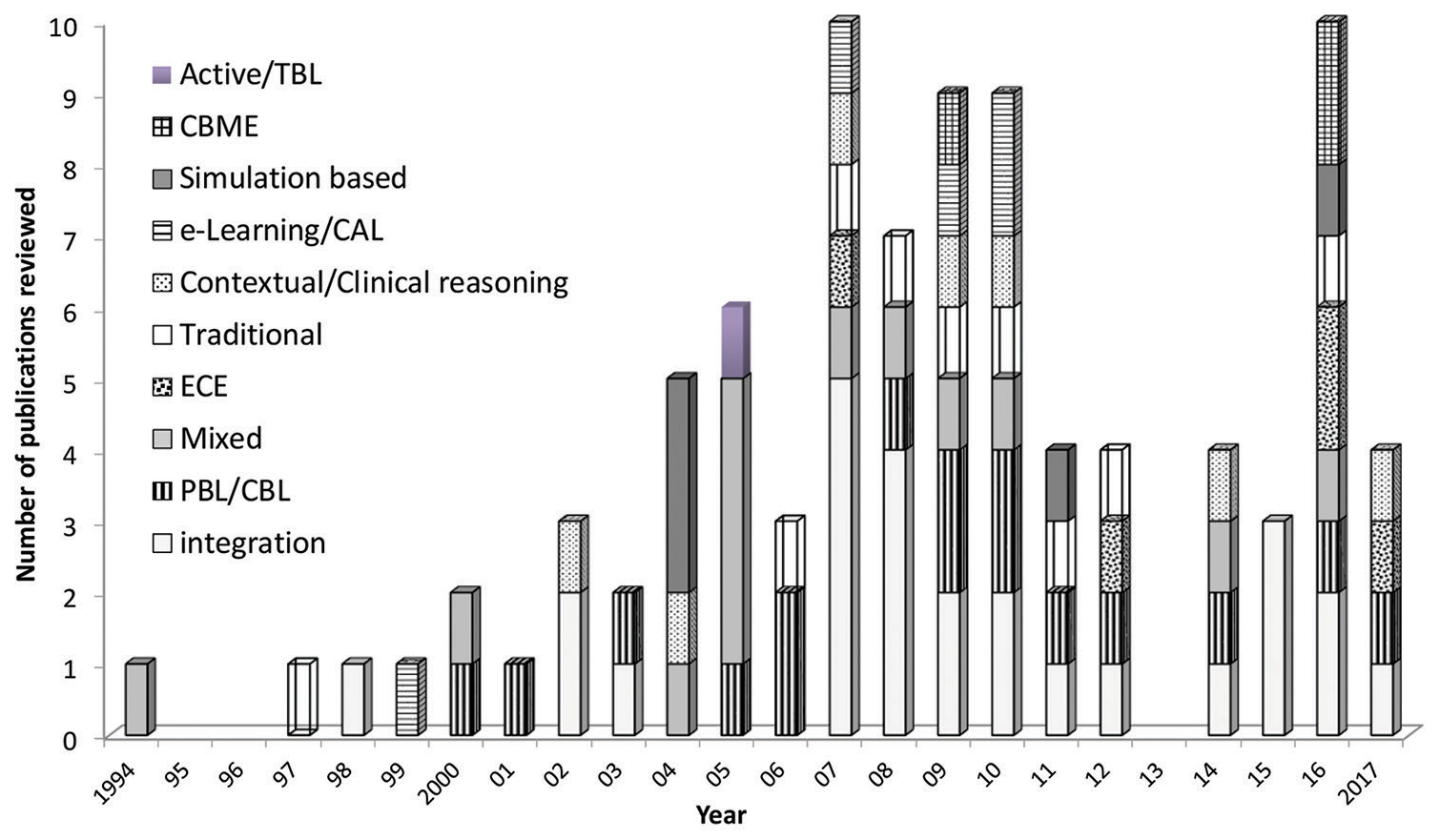
- Year-wise distribution of publications (n=90). PBL: Problem based learning, CBL: Case based learning, ECE: Early clinical exposure, CBME: Competency based medical education, CAL: Computer assisted learning, TBL: Team based learning
Most of the articles reviewed were original research articles (85.6%), followed by innovative articles (7.8%), invited articles (4.4%), and reviews (2.2%). Most of the studies (95.6%) were single centres and a few (12.2%) were multicentric involving 3–5 centres.[3,4,6,8,9,16-99] Most of the studies were conducted in schools and universities (82.3%) where a particular basic sciences teaching framework was being used.
[Table 2] depicts various categories of basic science teaching. The category of ‘integration of basic sciences teaching’ is being practiced approximately in one-third of studies (29%). This category included all studies involving vertical or horizontal integration or both. The level of integration was higher on Harden’s Ladder that’s why these studies were included.[100] This is followed by PBL/Case based learning (CBL) (18%) and the mixed-methods category (14%).
The traditional category (10%) included studies that were mainly based on traditional methods such as didactic lectures and practical classes. The contextual/clinical reasoning (8%) included studies that explored reasoning skills. Simulation-based and e-learning/CAL categories were equally represented (6%).
The year-wise category distribution of publication depicts that early clinical experience, traditional, and contextual/clinical reasoning studies are more in the latter half of the collection period, that is, the recent period [Figure 3]. The top three categories, that is integration, PBL/CBL, and mixed-methods studies are fairly distributed over the years. Simulation, competency-based medical education (CBME), and e-learning studies are not showing any consistent pattern and are sporadic.
Apart from the category of integration, integration was part of the basic sciences teaching framework in most (91.1%) of the articles.[17,18,21,34,74] Most of the studies involving integration used both horizontal and vertical integration (73.3%). About one-fifth of studies reported vertical integration (17.8%) and 1.4% of studies reported horizontal integration only. Integration started in year 1 in 62.2% of studies and after year 1 in other studies (18.9%).
Three-fourths of the studies (75.5%) used either a real patient or paper-based case in the basic sciences teaching framework. ECE was reported in a number of studies (62.5%). Information technology was used in approximately one-third (32.2%) of studies in various forms such as digitalisation of teaching materials, the use of videos, animations, computer simulations, high-fidelity simulations, and full-body mannequins. Most of the methods used in teaching-learning of basic sciences were innovative (80%). Some of these methods are given in detail in [Table 2].
Almost half of the studies (55.6%) included articles on multiple disciplines of basic sciences [Figure 4]. There were other articles where only one discipline of basic sciences was reviewed. Anatomy as an individual discipline was the concern of studies in basic sciences in one-fifth of studies (20%). In a study, team-based learning (TBL) was used in anatomy.[68]

- Subject-wise distribution of publications in the top three categories, PBL: Problem based learning, CBL: Case based learning
Since three main categories of basic sciences teaching framework came out to be integration, PBL/CBL, and mixed-methods approach, we also analysed the discipline-wise distribution of articles in these three categories. The integration category mainly involved articles with multiple disciplines (81%), PBL/CBL category included articles related to individual disciplines, especially anatomy and physiology (37.5%) as well as multi-discipline articles (48.8%). The mixed-method category included articles on individual disciplines, that is, anatomy (38.5), physiology (23.1), and multi-subjects (23.1).
The assessment was updated and modified in harmony with the implemented basic sciences teaching framework in approximately half (48.9%) of the studies [Table 3]. The updates in the assessment were slightly more prevalent in the integrated category (57.7% each) than in the PBL/CBL category (50%). The basic sciences were taught in the first 1–2 years in various frameworks (92.2%). There was no change in the overall duration of the course in most of the studies (94.4%). There was no change in the content of the overall course in half of the studies (48.9%). The contents of the overall course increased in some studies (16.7%) and decreased in other studies (13.3%), as shown in [Table 4].
| Updated | Not updated | Partially updated | |
|---|---|---|---|
| Overall course | 48.9 | 43.3 | 7.8 |
| Integrated | 57.7 | 38.5 | 3.8 |
| PBL/CBL | 50.0 | 50.0 | 0 |
| Mixed methods | 53.8 | 46.2 | 0 |
Values represent percentages. PBL: Problem-based learning, CBL: Case-based learning
| Increased | Decreased | Both | No change | |
|---|---|---|---|---|
| Overall | ||||
| Overall course | 16.7 | 13.3 | 21.1 | 48.9 |
| Basic sciences | 16.7 | 53.3 | 1.1 | 28.9 |
| Clinical sciences | 56.7 | 7.8 | 1.1 | 34.4 |
| Integrated | ||||
| Overall | 15.4 | 19.2 | 15.4 | 50.0 |
| Basic sciences | 0 | 61.5 | 3.8 | 34.6 |
| Clinical sciences | 53.8 | 0 | 3.8 | 42.3 |
| PBL/CBL | ||||
| Overall | 6.2 | 6.2 | 18.8 | 68.8 |
| Basic sciences | 12.5 | 62.5 | 0 | 25.0 |
| Clinical sciences | 62.5 | 12.5 | 0 | 25.0 |
| Mixed | ||||
| Overall | 23.1 | 7.7 | 7.7 | 61.5 |
| Basic sciences | 38.8 | 38.5 | 0 | 23.1 |
| Clinical sciences | 23.1 | 30.8 | 0 | 46.2 |
Values represent percentages. PBL: Problem-based learning, CBL: Case-based learning
The constructivism theory can help to explain the intervention in half of the studies (46.7%). This theory was more useful to explain learning in integration and PBL/CBL categories. The cognitivism theory seems to be involved in one-fifth of the studies (19%) and is more related to the traditional intervention studies. The behaviourism theory is more related to contextual learning and is found to be associated with 4.4% of studies. The sociocultural theory is related to few studies (7.8%) and the rest of the studies had mixed interventions; hence, there was a mix of theories contributing.
DISCUSSION
The quality of publications was ensured by following the pre-decided inclusion and exclusion criteria. The subjective bias was minimised by the involvement of two independent reviewers apart from the principal investigator. The agreement of conclusions among reviewers was well within acceptable limits.
The year-wise distribution indicates the increased need to try and identify the best strategies as the number of publications increased after 2004. The country-wise distribution over 23 countries shows the need for optimisation of basic sciences teaching at international levels. The maximum number of studies were from the United States of America (USA) which might be because the reforms started in a major way in the USA after Flexner’s report.[35] India and United Kingdom (UK) are next in the number of studies. India has a maximum number of medical schools in the country and implemented a new competency-based curriculum in 2019; hence, innovations are going on at various places.[13,78] In the UK, reforms in basic sciences are being tried at various medical schools.[101] In fact, WFME is trying for uniform accreditation as per defined standards in all institutes at the international level.[102] This has huge international implications as upcoming United States Medical Licensing Examination (USMLE) criteria to take students from accredited institutes will come into force in 2023.[103] Most of the experimentations involved single institutes indicating a lack of collaborative efforts which are needed.
The identification of ten categories of the framework in our study highlights the extent of experimentation in basic sciences teaching as well as uncertainty about the right recipe for optimal basic sciences teaching. Most of these studies were original research articles indicating that the investigator is trying to prove the utility of these interventions using scientific research methods. In educational research, we do not have gold standard designs like ‘randomised clinical trials’ to prove the efficacy of a drug.
The integration category was the most frequently tried intervention in the basic sciences teaching framework. Apart from the integration category, integration was involved to some extent in most of the other approaches used, for example, integration was part of PBL, CBL, early clinical experience, and contextual learning. The year-wise distribution highlights the increasing role of integration in recent years. Hence, our results depict a trend toward integration. The role and greater involvement of integration have been highlighted by various councils and associations.[16,104-106] Vertical integration is reported to stimulate students to have deep learning, a better understanding of basic sciences, and better retention of basic sciences.[30,76,79] Harden’s Ladder of Integration is a good guide to look at the level of integration. There is still a gap in understanding the right amount of integration of basic and clinical sciences. A rule of 20:80 can be used. In basic sciences, years use 80% basic sciences and 20% clinical sciences and reverse it in clinical years.[2]
The second category of PBL/CBL studies spread over various years in our study indicates the preference for this student-centred approach. PBL is reported to be the mainstay of innovations in basic sciences for a long time followed by the introduction of CBL.[107,108] The flexibility and utility of the mixed methods approach have been reported earlier.[83] The top three categories had good representation over the years indicating consistent experimentation with these methods.
The fourth category of traditional methods indicates the usefulness of conventional methods even now. In one study, students were concerned about not getting a solid foundation in some core content knowledge.[104] In another study, students asked for some lectures in essential core areas even in integrated frameworks.[42] This indicates that the methods, even if traditional, need to be optimised for learning and can be useful if used appropriately.[37] In the contextual/clinical reasoning category, the application of basic scientific knowledge was highlighted.[96]
Simulation and e-learning/CAL studies were not consistent over the years. The reason could be that these interventions depend a lot on technological advancements, the high cost of simulations such as mannequins, trained workforce, and other infrastructure support for simulations. Sometimes, high-fidelity simulations can be disruptive in the teaching-learning process.[47,94,109,110] The use of information technology was limited to one-third of the studies only. Although it was reported that technological advancement will be used more in the innovations, it was more of the concept of integration and use of cases in small groups which led the way in our review.[111]
The last three categories were represented with few studies only, that is, early clinical exposure (ECE), competency based medical education (CBME) and TBL. However, the low representation can be due to various reasons. The views of experts on CBME are debatable, and hence, this method has seen major ups and downs.[112,113] CBME studies were not consistent on time series and it shows that the competency-based or outcome-based approach is not evenly tried. On the other side, ECE studies are more in the later half of the time series indicating the picking up of this method. TBL is the least represented category. The earlier studies too reported limited use of TBL in medical education.[51,68]
The results of our study show that in most of the interventions, real patients or paper-based cases were used. This led to early clinical experience too. ECE was reported to be enjoyable and contributed to the learning.[71,78,80] This way the interventions were learner cantered in three-fourths of the studies. This shows a preference for the learner-centred approaches which have been postulated to be pivotal in learning.[114]
In our study, more than half of the studies involved multiple disciplines and were not limited to one or two disciplines only. The integration category studies and other studies with integration involved multiple disciplines indicating the importance of multiple disciplines for higher integration in both directions. Otherwise in other approaches, interventions involving a single discipline are also leading. This trend shows a shift toward the role of basic sciences collectively rather than individual discipline. In fact, the recent WFME guidelines define basic sciences as multiple disciplines.[102]
Assessment is one of the important pillars of any educational course. In our study, the assessment was not updated in approximately 40% of studies, especially in the integrated and PBL/CBL category. In the mixed methods approach, the assessment was updated. This is a very familiar situation where most of the time curriculum is changed without updating the assessment. Assessment is the most neglected part of curriculum planning and is left to universities to decide later on.[115]
The reduction in duration and contents in basic sciences needs to be carefully examined in light of the relevance in the overall teaching. In fact, a number of individual studies reported that the utility of basic sciences teaching improved when the relevant part was taught in the context of clinical application.[65,116]
Our review shows that basic sciences are being taught as ‘relevant parts’ only rather than traditional ways of learning full subjects before going to clinical sciences. One common theme of all interventions was to increase clinical sciences content and decrease basic sciences content or in other words to teach relevant basic sciences in the context of clinical sciences. This goes well with a renewed understanding of evolution in learning theories. The theories involved in learning in basic sciences are postulated to be varying based on the type of approaches used.
In our analysis, we found that constructivism theory played a significant role in integration approaches in basic sciences teaching. In the PBL/CBL category, learning can also be explained on the basis of constructivism.[117] A mixed-method approach involved more than a single theory, but the conglomeration of stories was not very scientific. However, it is difficult to associate one single theory with learning. When these theories are viewed in the ascending stages of learning these theories complement each other and are more like a part of evolutionary sequences in learning.
This is depicted in various interventions used in the publications that we reviewed in this study. There is ascendency in categories from cognitivism (traditional) to constructivism (integration, PBL/CBL) to sociocultural and behaviourism (learning in context, in the community) to critical (societal changes) and to humanism (own growth). In this era of information explosion and easy availability of knowledge, we need to look at theories that remain relevant.[117]
CONCLUSION
The review of basic sciences teaching frameworks in our study indicates that certain gaps do exist in our understanding. The gaps or issues of concern that can lead to the formulation of a research agenda to optimise clinical science teaching can be viewed as opportunities for improvement. The results can help in effective policy-making for improvising the basic sciences in terms of contents, context, duration, and the way it is being taught. However, this needs to be interpreted in light of clinical experience and expertise. This will help to optimise the utility of basic sciences teaching to improve clinical sciences teaching in UG medical education.
Ethical approval
Institutional review board approval is not required.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of Artificial Intelligence (AI)-Assisted Technology for assisting in the writing or editing of the manuscript and no images were manipulated using the AI.
Financial support and sponsorship
Nil.
References
- American medical education 100 years after the Flexner report. N Engl J Med. 2006;355:1339-44.
- [CrossRef] [PubMed] [Google Scholar]
- Teaching of the basic sciences in medicine: Changing trends. Natl Med J India. 2015;28:137-40.
- [Google Scholar]
- Learning experiences and assessment in the first 2 years of the medical course at King's College London School of Medicine. Keio J Med. 2010;59:140-5.
- [CrossRef] [PubMed] [Google Scholar]
- Teaching and evaluating first and second year medical students' practice of evidence-based medicine. Med Educ. 2004;38:868-78.
- [CrossRef] [PubMed] [Google Scholar]
- Problem-based learning and the medical school: Another case of the emperor's new clothes? Adv Physiol Educ. 2005;29:194-6.
- [CrossRef] [PubMed] [Google Scholar]
- Case method teaching: An effective approach to integrate the basic and clinical sciences in the preclinical medical curriculum. Med Teach. 2009;31:834-41.
- [CrossRef] [PubMed] [Google Scholar]
- The effectiveness of the problem-based learning teaching model for use in introductory Chinese undergraduate medical courses: A systematic review and meta-analysis. PLoS One. 2015;10:e0120884.
- [CrossRef] [PubMed] [Google Scholar]
- Developing a competency-based medical education curriculum for the core basic medical sciences in an African Medical School. Adv Med Educ Pract. 2016;7:389-98.
- [CrossRef] [PubMed] [Google Scholar]
- Attitudes among students and teachers on vertical integration between clinical medicine and basic science within a problem-based undergraduate medical curriculum. Med Teach. 2002;24:286-8.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical and basic science teachers' opinions about the required depth of biomedical knowledge for medical students. Med Teach. 2006;28:234-8.
- [CrossRef] [PubMed] [Google Scholar]
- Integration and timing of basic and clinical sciences education. Med Teach. 2013;35:381-7.
- [CrossRef] [PubMed] [Google Scholar]
- Integrated teaching : A less trodden path. Indian J Physiol Pharmacol. 2015;58:189-91.
- [Google Scholar]
- Undergraduate medical education curriculum in India : Is a change needed. ? Sub-Himalayan J Health Res. 2016;3:36-40.
- [Google Scholar]
- WFME standards for educational programmes: Tutors' perceptions in Pakistan. Educ Med J. 2013;5:43-54.
- [CrossRef] [Google Scholar]
- Social studies in improving students' map skills: Teachers' opinions. Educational sci: Theo pract. 2015;15:1345-62.
- [Google Scholar]
- Validating the effectiveness of Clinically Oriented Physiology Teaching (COPT) in undergraduate physiology curriculum. BMC Med Educ 2008:204-8.
- [CrossRef] [PubMed] [Google Scholar]
- Key steps for integrating a basic science throughout a medical school curriculum using an e-learning approach. Med Teach. 2009;31:822-8.
- [CrossRef] [PubMed] [Google Scholar]
- Do we need dissection in an integrated problem-based learning medical course? Perceptions of first-and second-year students. Surg Radiol Anat. 2007;29:173-80.
- [CrossRef] [PubMed] [Google Scholar]
- Integration of basic sciences in health's courses. Biochem Mol Biol Educ. 2012;40:204-8.
- [CrossRef] [PubMed] [Google Scholar]
- Computer simulation models are implementable as replacements for animal experiments. Altern Lab Anim. 2009;37:191-5.
- [CrossRef] [PubMed] [Google Scholar]
- Blended learning-integrating E learning with traditional learning methods in teaching basic medical science. Al Ameen J Med Sci. 2014;7:265-9.
- [Google Scholar]
- Clinical rotation in pathology: Description of a case based approach. J Clin Pathol. 2006;59:355-9.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of clinical relevance of problem-oriented teaching in undergraduate anatomy at the University of Pretoria. Surg Radiol Anat. 2001;23:57-60.
- [CrossRef] [PubMed] [Google Scholar]
- Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. 2006;355:2217-25.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of the foundations of clinical medicine course on USMLE scores. J Gen Intern Med. 2008;23:1002-5.
- [CrossRef] [PubMed] [Google Scholar]
- Enhancing learning through optimal sequencing of web-based and manikin simulators to teach shock physiology in the medical curriculum. Adv Physiol Educ. 2011;35:402-7.
- [CrossRef] [PubMed] [Google Scholar]
- Integrating basic science into clinical teaching initiative (IBS-CTI): Preliminary report. J Pediatr. 2008;153:683-7.
- [CrossRef] [PubMed] [Google Scholar]
- Design, implementation, and evaluation of a simulation-based clinical correlation curriculum as an adjunctive pedagogy in an anatomy course. Acad Med. 2017;92:494-500.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge loss of medical students on first year basic science courses at the University of Saskatchewan. BMC Med Educ. 2006;6:5.
- [CrossRef] [PubMed] [Google Scholar]
- Pros and cons of vertical integration between clinical medicine and basic science within a problem-based undergraduate medical curriculum: Examples and experiences from Linköping, Sweden. Med Teach. 2002;24:280-5.
- [CrossRef] [PubMed] [Google Scholar]
- Computer-aided learning: An overvalued educational resource? Med Educ. 1999;33:136-9.
- [CrossRef] [PubMed] [Google Scholar]
- The impact of pre-clinical pharmacology and pharmacotherapy training on students' abilities and perceptions during clinical rotations. Med Teach. 2007;29:981-3.
- [CrossRef] [PubMed] [Google Scholar]
- Early clinical experience : A way for preparing. Galn Med J. 2012;1:42-7.
- [CrossRef] [Google Scholar]
- Exploring the value and role of integrated supportive science courses in the reformed medical curriculum iMED: A mixed methods study. BMC Med Educ. 2016;16:132.
- [CrossRef] [PubMed] [Google Scholar]
- Dissection as a teaching tool: Past, present, and future. Anat Rec B New Anat. 2005;285:11-5.
- [CrossRef] [PubMed] [Google Scholar]
- Teaching skills to promote clinical reasoning in early basic science courses. Anat Sci Educ. 2010;3:267-71.
- [CrossRef] [PubMed] [Google Scholar]
- Provision of anatomical teaching in a new British medical school: Getting the right mix. Anat Rec B New Anat. 2005;284:22-7.
- [CrossRef] [PubMed] [Google Scholar]
- Physician perceptions of the role and value of basic science knowledge in daily clinical practice. Med Teach. 2012;34:744-7.
- [CrossRef] [PubMed] [Google Scholar]
- Are we teaching sufficient anatomy at medical school? The opinions of newly qualified doctors. Clin Anat. 2008;21:718-24.
- [CrossRef] [PubMed] [Google Scholar]
- Development of visual pharmacology education across an integrated medical school curriculum. J Vis Commun Med. 2007;30:156-61.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical integration of biochemistry and clinical medicine using a near-peer learning model. Biochem Mol Biol Educ. 2016;44:507-16.
- [CrossRef] [PubMed] [Google Scholar]
- Development of basic medical sciences in a new medical school with an integrated curriculum: The ANU experience. Med Teach. 2009;31:829-33.
- [CrossRef] [PubMed] [Google Scholar]
- Combination of didactic lectures and case-oriented problem-solving tutorials toward better learning: Perceptions of students from a conventional medical curriculum. Adv Physiol Educ. 2007;31:193-7.
- [CrossRef] [PubMed] [Google Scholar]
- Combination of didactic lecture with problem-based learning sessions in physiology teaching in a developing medical college in Nepal. Adv Physiol Educ. 2000;24:8-12.
- [CrossRef] [PubMed] [Google Scholar]
- Undergraduate anatomy teaching in the UK. Bull Royal Coll Surg England. 2009;91:102-6.
- [CrossRef] [Google Scholar]
- Bringing good teaching cases “to life”: A simulator-based medical education service. Acad Med. 2004;79:23-7.
- [CrossRef] [PubMed] [Google Scholar]
- A study of the competency of third year medical students to interpret biochemically based clinical scenarios using knowledge and skills gained in year 1 and 2. Biochem Mole Biol Educ. 2016;44:202-7.
- [CrossRef] [PubMed] [Google Scholar]
- Restructuring a basic science course for core competencies: An example from anatomy teaching. Med Teach. 2009;31:855-61.
- [CrossRef] [PubMed] [Google Scholar]
- Integrated and contextual basic science instruction in preclinical education: Problem-based learning experience enriched with brain/mind learning principles. Educ sci: Theo pract. 2015;15:1215-28.
- [Google Scholar]
- Teaching of medical pharmacology: the need to nurture the early development of desired attitudes for safe and rational drug prescribing. Med Teach. 2009;31:847-54.
- [CrossRef] [PubMed] [Google Scholar]
- An initial experience with “team learning” in medical education. Acad Med. 2002;77:40-4.
- [CrossRef] [PubMed] [Google Scholar]
- Student perceptions of the use of presentations as a method of learning endocrine and gastrointestinal pathophysiology. Adv Physiol Educ. 2010;34:75-85.
- [CrossRef] [PubMed] [Google Scholar]
- Medical students preference of problem-based learning or traditional lectures in King Abdulaziz University, Jeddah, Saudi Arabia. Ann Saudi Med. 2014;34:128-33.
- [CrossRef] [PubMed] [Google Scholar]
- Integrated cases section: A course designed to promote clinical reasoning in year 2 medical students. Teach Learn Med. 2010;22:312-6.
- [CrossRef] [PubMed] [Google Scholar]
- The use of self-learning modules to facilitate learning of basic science concepts in an integrated medical curriculum. Anat Sci Educ. 2010;3:219-26.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomy as the backbone of an integrated first year medical curriculum: Design and implementation. Anat Sci Educ. 2011;4:157-69.
- [CrossRef] [PubMed] [Google Scholar]
- Contexts, concepts and cognition: Principles for the transfer of basic science knowledge. Med Educ. 2017;51:184-95.
- [CrossRef] [PubMed] [Google Scholar]
- Acceptance and impact of integrated teaching in undergraduate medical student: An observational cross-sectional study. Natl J Integr Res Med. 2016;7:93-8.
- [Google Scholar]
- Appraisal and improvisation of undergraduate practical curriculum in physiology. South East Asia J Med Educ. 2010;4:55-8.
- [CrossRef] [Google Scholar]
- The influence of the new pathway curriculum on Harvard medical students. Acad Med. 1994;69:983-9.
- [CrossRef] [PubMed] [Google Scholar]
- A multimedia approach for teaching human embryology: Development and evaluation of a methodology. Ann Anat. 2010;192:388-95.
- [CrossRef] [PubMed] [Google Scholar]
- Lessons learned about integrating a medical school curriculum: Perceptions of students, faculty and curriculum leaders. Med Educ. 2008;42:778-85.
- [CrossRef] [PubMed] [Google Scholar]
- Medical student knowledge regarding radiology before and after a radiological anatomy module: Implications for vertical integration and self-directed learning. Insights Imaging. 2014;5:629-34.
- [CrossRef] [PubMed] [Google Scholar]
- Preparing medical students for future learning using basic science instruction. Med Educ. 2014;48:667-73.
- [CrossRef] [PubMed] [Google Scholar]
- Medical clerks' attitudes towards the basic sciences: A longitudinal and a cross-sectional comparison between students in a conventional and an innovative curriculum. Med Teach. 2007;29:772-7.
- [CrossRef] [PubMed] [Google Scholar]
- Expanding course goals beyond disciplinary boundaries: Physiology education in an undergraduate course on psychoactive drugs. Adv Physiol Educ. 2007;31:161-6.
- [CrossRef] [PubMed] [Google Scholar]
- Team-based learning in a medical gross anatomy and embryology course. Clin Anat. 2005;18:56-63.
- [CrossRef] [PubMed] [Google Scholar]
- Development of knowledge in basic sciences: A comparison of two medical curricula. Med Educ. 2012;46:1206-14.
- [CrossRef] [PubMed] [Google Scholar]
- The role of basic sciences in a problem-based learning clinical curriculum. Med Educ. 2000;34:608-13.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of early clinical exposure in learning respiratory physiology among the newly entrant MBBS students. J Adv Med Educ Prof. 2017;5:6-10.
- [Google Scholar]
- Anatomy curriculum for medical students: what can be learned for future curricula from evaluations and questionnaires completed by students, anatomists and clinicians in different countries? Ann Anat. 2009;191:541-6.
- [CrossRef] [PubMed] [Google Scholar]
- Satisfaction of the pre-clinical students regarding current anatomy curriculum and anatomy teachers of Kust Institute of Medical Sciences (KIMS), Kohat. KUST Med J. 2011;3:45-51.
- [Google Scholar]
- A case based-shared teaching approach in undergraduate medical curriculum: A way for integration in basic and clinical sciences. Acta Med Iran. 2017;55:259-64.
- [Google Scholar]
- Does problem-based learning lead to deficiencies in basic science knowledge? An empirical case on anatomy. Med Educ. 2003;37:15-21.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical integration of basic science in final year of medical education. Int J Appl Basic Med Res. 2016;6:182.
- [CrossRef] [PubMed] [Google Scholar]
- Perspectives in medical education 5. Implementing a more integrated, interactive and interesting curriculum to improve Japanese medical education. Keio J Med. 2007;56:75-84.
- [CrossRef] [PubMed] [Google Scholar]
- Skill learning through early clinical exposure: An experience of Indian Medical School. J Clin Diagn Res. 2016;10:C01-4.
- [CrossRef] [PubMed] [Google Scholar]
- Motivating medical students to learn basic science concepts using chronic myeloid leukemia as an integration theme. Rev Bras Hematol Hemoter. 2015;37:63-6.
- [CrossRef] [PubMed] [Google Scholar]
- Attitude of medical students towards early clinical exposure in learning endocrine physiology. BMC Med Edu. 2007;7:30.
- [CrossRef] [PubMed] [Google Scholar]
- Integrating the teaching of basic sciences, clinical sciences, and biopsychosocial issues. Acad Med. 1998;73(9 Suppl):S24-31.
- [CrossRef] [Google Scholar]
- The use of multiple tools for teaching medical biochemistry. Adv Physiol Educ. 2008;32:38-46.
- [CrossRef] [PubMed] [Google Scholar]
- Blended learning in medical education: Use of an integrated approach with web-based small group modules and didactic instruction for teaching radiologic anatomy1. Acad Radiol. 2004;11:1059-70.
- [CrossRef] [PubMed] [Google Scholar]
- Experience with a theme-based integrated renal module for a second-year MBBS class. Adv Physiol Educ. 2010;34:15-9.
- [CrossRef] [PubMed] [Google Scholar]
- Standardized patient's views about their role in the teaching-learning process of undergraduate basic science medical students. J Clin Diagn Res. 2016;10:JC01-5.
- [CrossRef] [PubMed] [Google Scholar]
- Integration of cognitive skills as a cross-cutting theme into the undergraduate medical curriculum at Tehran university of medical sciences. Acta Med Iran. 2017;55:68-73.
- [Google Scholar]
- Commentary: IDSA guidelines for improving the teaching of preclinical medical microbiology and infectious diseases. Acad Med. 2010;85:19-22.
- [CrossRef] [PubMed] [Google Scholar]
- The Minnesota virtual clinic: Using a simulated EMR to teach medical students basic science and clinical concepts. AMIA Annu Symp Proc. 2003;2003:1013.
- [Google Scholar]
- Paired basic science and clinical problem-based learning faculty teaching side by side: Do students evaluate them differently? Med Educ. 2005;39:194-201.
- [CrossRef] [PubMed] [Google Scholar]
- Introduction of real patients into problem-based learning in preclinical first-year anatomy curriculum. Med Teach. 2011;33:854-6.
- [CrossRef] [PubMed] [Google Scholar]
- Blending problem-based learning with Web technology positively impacts student learning outcomes in acid-base physiology. Adv Physiol Educ. 2005;29:35-9.
- [CrossRef] [PubMed] [Google Scholar]
- What makes the learning of physiology in a PBL medical curriculum challenging? Student perceptions. Adv Physiol Educ. 2009;33:187-95.
- [CrossRef] [PubMed] [Google Scholar]
- The perception of MBBS interns towards biochemistry curriculum in a south Indian medical college. Natl J Integr Res Med. 2016;7:82-7.
- [Google Scholar]
- Using high-fidelity patient simulation and an advanced distance education network to teach pharmacology to second-year medical students. J Clin Anesth. 2004;16:144-51.
- [CrossRef] [PubMed] [Google Scholar]
- An effective integrated learning programme in the first year of the medical course. Natl Med J India. 2008;21:21-6.
- [Google Scholar]
- No content without context: Integrating basic, clinical, and social sciences in a pre-clerkship curriculum. Med Teach. 2009;31:812-21.
- [CrossRef] [PubMed] [Google Scholar]
- Two perspectives on the effects of a curriculum change: Student experience and the United States medical licensing examination, step 1. Acad Med. 2007;82:S117-20.
- [CrossRef] [PubMed] [Google Scholar]
- The role of biomedical knowledge in diagnosis of difficult clinical cases. Adv Health Sci Educ Theory Pract. 2007;12:417-26.
- [CrossRef] [PubMed] [Google Scholar]
- The value of basic science in clinical diagnosis: Creating coherence among signs and symptoms. Med Educ. 2005;39:107-12.
- [CrossRef] [PubMed] [Google Scholar]
- The integration ladder: A tool for curriculum planning and evaluation. Med Educ. 2000;34:551-7.
- [CrossRef] [PubMed] [Google Scholar]
- A BEME systematic review of UK undergraduate medical education in the general practice setting: BEME Guide No. 32. Med Teach. 2015;37:611-30.
- [CrossRef] [PubMed] [Google Scholar]
- Basic medical education: WFME global standards for quality improvement. World Fed Med Educ. 2007;36 Available from: https://wfme.org/wp-content/uploads/2020/12/WFME-BME-Standards-2020-1.pdf [Last accessed on 2023 Aug 06]
- [Google Scholar]
- The association between medical education accreditation and examination performance of internationally educated physicians seeking certification in the United States. Qual High Educ. 2013;19:283-99.
- [CrossRef] [Google Scholar]
- Physicians for the twenty-first century. Report of the project panel on the general professional education of the physician and college preparation for medicine. J Med Educ. 1984;59:1-208.
- [CrossRef] [Google Scholar]
- Tomorrow's doctors-outcomes and standards for undergraduate medical education. 2009. London: General Medical Council; :1-108. Available from: https://www.kcl.ac.uk/lsm/study/outreach/downloads/tomorrows-doctors.pdf [Last accessed on 2023 Aug 06]
- [Google Scholar]
- Revival of the case method: A way to retain student-centred learning in a post-PBL era. Med Teach. 2007;29:e32-6.
- [CrossRef] [PubMed] [Google Scholar]
- PBL in the undergraduate MD program at McMaster University: Three iterations in three decades. Acad Med. 2007;82:370-4.
- [CrossRef] [PubMed] [Google Scholar]
- Teaching basic science to optimize transfer. Med Teach. 2009;31:807-11.
- [CrossRef] [PubMed] [Google Scholar]
- Simulation and technology-enhanced learning In: FAIMER-Keele Master's in health professions education: Accreditation and assessment, Module 6, Unit 7 (2nd ed). London: FAIMER Cent Distance Learn CenMEDIC; 2015. p. :1-65.
- [Google Scholar]
- Is learning anatomy facilitated by computer-aided learning? A review of the literature. Med Teach. 2009;31:e393-6.
- [CrossRef] [PubMed] [Google Scholar]
- Competency-based training: Who benefits? Postgrad Med J. 2013;89:107-10.
- [CrossRef] [PubMed] [Google Scholar]
- Competency-based medical education: An overview and application in pharmacology. Indian J Pharmacol. 2016;48:S5-9.
- [CrossRef] [PubMed] [Google Scholar]
- Educational strategies in curriculum development: The SPICES model. Med Educ. 1984;18:284-97.
- [CrossRef] [PubMed] [Google Scholar]
- Student assessment: Moving over to programmatic assessment. Int J Appl Basic Med Res. 2016;6:149-50.
- [CrossRef] [PubMed] [Google Scholar]
- Persistent reservations against the premedical and medical curriculum. Perspect Med Educ. 2013;2:335-9.
- [CrossRef] [PubMed] [Google Scholar]




