
Translate this page into:
Testing of a self-learning, demonstration, and preceptorship model on nurses for pediatric COVID-19 preparedness
-
Received: ,
Accepted: ,
How to cite this article: Venkatesan L, Joshi P, Susaimuthu CM, Murry LL, Simak KS, Yadav S, et al. Testing of a self-learning, demonstration, and preceptorship model on nurses for pediatric COVID-19 preparedness. Indian J Physiol Pharmacol. 2023;67:321-8. doi: 10.25259/IJPP_479_2022
Abstract
Objectives:
The objectives of this study were to develop and test a teaching and learning model in clinical nursing education to integrate the key concepts of self-learning, demonstration (simulation – zone I) and preceptorship (SDP). Coronavirus disease has affected adults and a significant proportion of children globally. All nurses must know the stabilisation and management of children affected by coronavirus disease-2019 (COVID-19).
Materials and Methods:
A paediatric nursing emergency preparedness program for COVID-19 of 8 days duration was developed with the help of a team of 42 medical and nursing experts. The training program was conducted for 300 nurses using a SDP model with a blended learning approach. The effectiveness of the SDP model was evaluated using a one-group pre-test and post-test design in terms of change in knowledge and self-confidence of the participants. Feedback from the participants, experts and preceptors about the program and teaching methodology was obtained at the end of the training program.
Results:
The mean gain in knowledge (12.57 ± 2.96 vs. 16.36 ± 4.26, P < 0.001) and self-confidence scores (84.08 ± 18.20 vs. 106.65± 9.86, P < 0.001) after the training program were statistically significant. The overall mean preceptors rating of the participants in various observed skills was 55.88 ± 15.21 with the majority of observations graded as competent. All the experts, preceptors and participants were satisfied with the training program.
Conclusion:
The SDP model using a blended learning approach was effective in improving the knowledge and self-confidence of the nurses in managing children with COVID-19. It can be used to train nurses in both technical and non-technical skills in patient care areas.
Keywords
Demonstrations
Preceptorship
Paediatric COVID preparedness
Self learning-demonstration-preceptorship model
Self-learning

INTRODUCTION
Coronavirus disease-2019 (COVID-19) caused by a novel Severe Acute Respiratory Syndrome Coronavirus 2 had a devastating effect globally. The disease mainly affected adults and a proportion of children with COVID-19 illness in the first and the second wave.[1-3] The available epidemiological data from India related to COVID-19 among children suggest that individuals below 20 years constituted <12% of all confirmed cases and their mortality remained <2% in the same age group.[4-7] It was anticipated that the third wave of the pandemic would have a considerable impact on children due to their current unvaccinated status. However, there was no evidence to date to support the same. Some children became severely ill with COVID-19, while some, later on, developed multi-system inflammatory syndrome and needed hospitalisation. They were treated in the intensive care unit and required ventilatory support.[8] Children with comorbid conditions, such as obesity, diabetes and asthma, are at higher risk of serious illness with COVID-19.[9] Children with congenital heart diseases, genetic defects or conditions affecting the nervous system or metabolism might be similarly at higher risk of serious illness.[10]
The COVID care centre in our institute was set up by converting the existing trauma centre facility, during the 1st and 2nd COVID-19 waves. Nurses, being the backbone of any healthcare team as frontline workers played a crucial role in the management of patients with COVID-19. For handling the challenges of the third and the subsequent waves of COVID, a need for preparing a COVID task force was realised, that could participate in triaging, stabilisation and providing ongoing care to sick children.[8] Nurses’ role in counselling the parents can also be a great help in providing family-centred care to sick children. The nurses must be well-equipped with the essential knowledge and skills required in managing sick children. Therefore, we developed a paediatric nursing emergency preparedness program for COVID-19 (PNEPPCO) of 8-day duration. We developed an self-learning, demonstration (simulation – zone I) and preceptorship (SDP) model using a blended learning approach for imparting the PNEPPCO training. The training program was conducted for 300 nurses twice a week for 5 weeks in small groups of 30–35 nurses each. The outcome of the training was measured in terms of the change in knowledge and self-confidence of the nurses.
MATERIALS AND METHODS
Development of the training program
The PNEPPCO program along with the training methodology used for imparting the training was developed in three stages. In the first stage, a group of 42 medical and nursing experts in child health care were invited to develop the training program. Seven teams were formed, each one having 6 experts including both the medical and nursing disciplines. The broad areas were identified as (i) triaging and stabilisation of children with COVID-19 including proning and salient points of paediatric basic and advanced life support in COVID-19, (ii) maintenance of airway and oxygen administration using low-flow devices, (iii) administration of oxygen using high-flow devices including invasive ventilation, (iv) paediatric equipment such as radiant warmer, infusion pump, bubble continuous positive airway pressure used in paediatric and neonatal intensive care units, (v) drug calculation and administration, commonly used drugs in COVID-19, (vi) nutrition in children with COVID-19 and (vii) infection control in COVID-19 [Table 1].
| S. No. | Station | Skills |
|---|---|---|
| 1. | Assessment and stabilisation | Triaging the children based on priority to initiate the care appropriately |
| Assessment of a sick child, vitals monitoring and stabilisation of a sick child | ||
| Assisting in paediatric basic life support | ||
| Proning in children | ||
| 2. | Oxygenation | Assessment a sick child for airway patency and perform basic measures to restore airway patency |
| Administering oxygen in children using low-flow oxygen devices, HHHFNO | ||
| Administering oxygen using high-flow devices including the use of | ||
| 3. | Ventilation | NIV, its indication and how to provide NIV |
| Assisting in endotracheal intubation, | ||
| Nursing care of children on mechanical ventilation including monitoring | ||
| Performing closed suctioning | ||
| 4. | Medication and fluid therapy | Identification and selection of appropriate vein for intravenous cannulation |
| Fluid and drug dosage calculation in children | ||
| Administering drugs using a nebuliser | ||
| Performing care of intravascular catheters | ||
| 5. | Paediatric medical equipment | Care of a baby under radiant warmer continuous positive airway |
| Assembling CPAP machine and nursing care of baby on CPAP | ||
| Starting an IV infusion pump | ||
| Use of a defibrillator in children | ||
| 6. | Nutrition in COVID children | Breast feeding in neonates and infants and feeding in other children |
| 7. | Infection control practices | Asepsis, use of personal protective equipment |
| Disinfection and sterilisation | ||
| Biomedical waste management |
COVID: Coronavirus disease, NIV: Non-invasive ventilation, CPAP: Continuous positive airway pressure, HHHFNO: Heated, humidified, high-flow nasal oxygen
Each team was allotted one area from the decided topics to prepare the content of the e-learning module [Table 1]. The teams developed the contents of the module based on the extensive literature of the latest available evidence in the field. With an intense theoretical review method, the content of the program was finalised in eight online meetings. In the second stage, the developed program was shared with four experts for content analysis from the field of neonatology, paediatrics and nursing. Based on the suggestions of the experts, the content of the training program was finalised. In stage three, we decided on the training methodology after two brainstorming sessions. The SDP model consisting of self-learning, demonstration (Zone I simulation) and preceptorship was finalised for imparting to the nurses in managing paediatric patients with COVID-19 [Figure 1]. The SDP model provided competency-based learning to the nurses, and not just merely knowledge-based learning. The model was intended to provide a framework that can be used for professional nursing education which incorporates the core value of SDP to prepare the in-service education nurses to provide quality-based and individualised patient-centred care during the COVID-19 pandemic. The training methodology consisted of a self-learning phase (5 days), a skill demonstration and practice phase (1 day) and a preceptorship phase in the paediatric clinical area for 2 days.
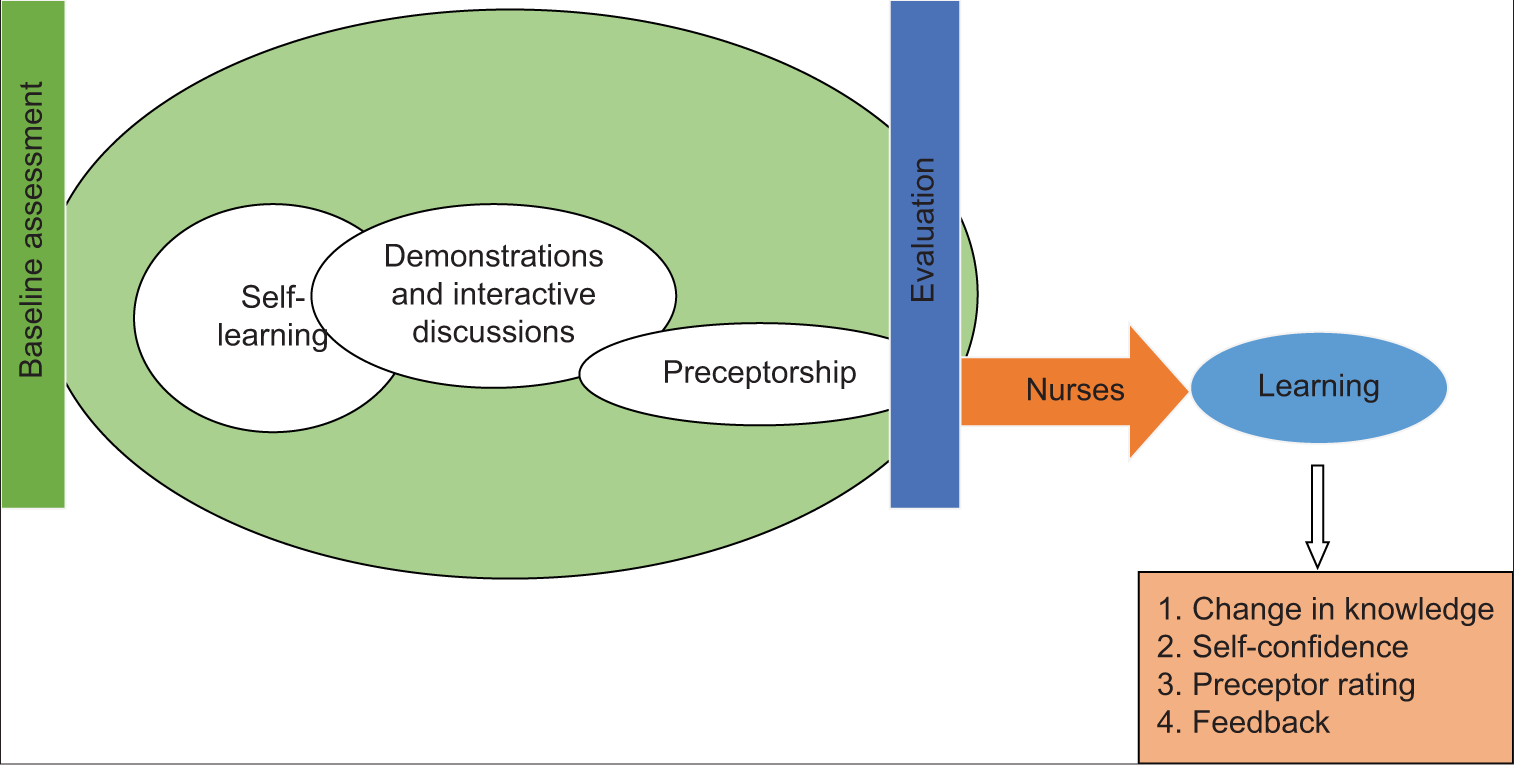
- An self-learning, demonstration and preceptorship model.
Setting
The training program adopted a blended teaching methodology and utilised both web-based and face-to-face teaching-learning activities. A total of 300 nurses working at the trauma centre (COVID unit) were invited to participate in the training programs. Ethical permission was obtained from the Institute Ethics Committee (IEC letter no. IEC-550/06.08.2021, RP-23/2021). The written informed consent was obtained through a Google form after informing the participants about the purpose of the study. Confidentiality and anonymity were ensured to all the participants. The entire training program was spread over 5 weeks and was conducted twice a week by enrolling 30 nurses in each group in the simulation e-learning telemedicine (SET) facility of the institute. The preceptorship program was carried out in the paediatric and neonatal wards/intensive care units of the hospital by 16 nurses specialised in paediatric and neonatal care.
Tools and techniques
The tools developed for the procedure of data collection were the demographic profile, knowledge questionnaire and self-confidence tool. The demographic profile has items related to age, gender and years of experience and undergone any training program related to COVID-19. The knowledge questionnaire had 25 multiple-choice questions (MCQs) items. The MCQs were developed from a standardised and validated resource material on paediatric critical care prepared for the course. A score of ‘1’ was given for every correct response and ‘0’ for the incorrect response, with a maximum possible score of 25. The participants rated their confidence in performing paediatric nursing procedures on a 5-point Likert scale ranging from ‘highly confident-5’ to ‘not confident at all 1’ for each procedure. The feedback proforma had 6 items related to the quality of the resource material, relevance of the skills taught, hands-on training, overall benefit of the course, confidence in performing skills and the likelihood of recommending the training to the colleagues rated on a 5-point Likert scale. The reliability and validity of the tools were established before administration. The preceptor’s evaluation pro forma had 26 activities, which included all the skills imparted to them during self-learning and demonstrations. The observed skills of the participants were graded as competent (3), less competent (2) and needing improvement (1) with the scores ranging from 1 to 3 for each activity. The proforma had maximum and minimum possible scores of 78 and 26, respectively. Feedback from the experts and preceptors was also taken using a 5-item questionnaire on a 4-point Likert scale.
Procedure for data collection
A group of 30 nurses was enrolled in each training program. An official chat group was made for communication and dissemination of the resource material using the Telegram App. The nurses completed a need assessment survey 2–3 days before the training program. In the needs assessment, nurses rated their level of confidence in performing common paediatric nursing skills on a 5-point Likert scale ranging from ‘highly confident-5’ to ‘not confident at all 1.’ A brief demographic proforma was also filled by the nurses that included their educational background and professional experience. The baseline knowledge assessment of the participants was done using 25-item MCQs. The questionnaires were shared as a Google form link on the Telegram app and the nurses were requested to click on the link and complete them.
In the self-learning phase, the training resource material was shared with the nurses through the Telegram app. The participants were instructed to read the materials and clear their doubts if any on the chat group. The nurses were requested to go through the study material at their own pace. The material consisted of webinars, videos and pdf material. The self-learning phase was followed by guided skills and interactive practice sessions in small groups of 5–6 nurses per station. Five stations were made, manned by 3–4 experts [Table1]. Each station had 3–4 skills to learn. The participants were rotated through the five skills stations, namely, assessment and stabilisation of a sick child including proning, oxygenation, ventilation, medication, fluid therapy and paediatric medical equipment. Each station was facilitated by a team of medical faculty, nursing faculty and clinical nurse expert. The participants spent approximately 40–45 min in each skill station. Two sessions on nutrition and infection control practices were conducted in the form of an open house session. The participants were encouraged to participate in interactive case-based discussions. The facilitators helped the participants to enhance their knowledge and refresh their skills. Following the skills training, the nurses were posted in the paediatric units of the hospital for 2 days for clinical practice. Sixteen senior nurses working in paediatric areas for at least 5 years were approached to act as preceptors to the trainee nurse [Figure 2]. They were oriented to their role and expectation as a preceptor in a meeting. Each subject was assigned a preceptor to guide practice. The preceptors supervised the participants in the clinical area for 2 days and rated their performance randomly on the competency of skills on a 3-point rating scale (3 – competent, 2 – less competent and 1 – needs improvement) at the end of the 2-day preceptor-ship program. The entire training program was conducted in a mutually respectful environment.
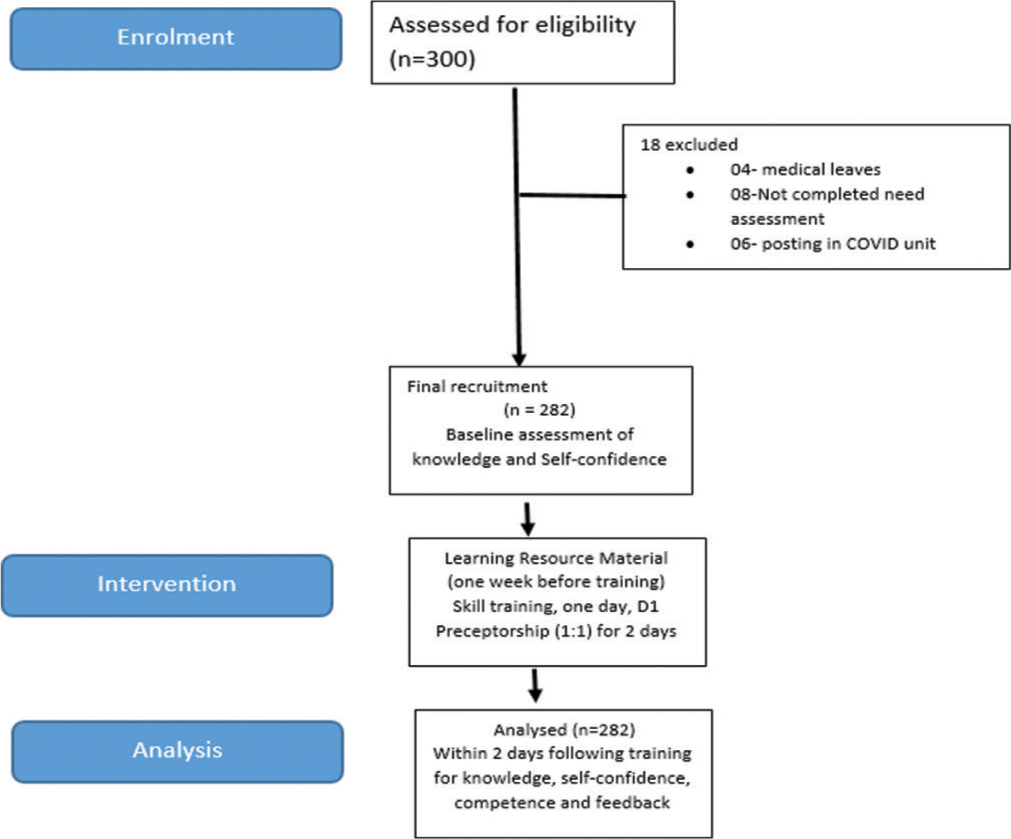
- Consort diagram. n: Number of nurses.
Outcome assessment
The impact of the training program was assessed in terms of the knowledge and confidence of the participants within 2 days of completion of the training. Post-test assessment of the participants was also done through online mode. The participants also filled out a feedback form on the quality of the training. Preceptors randomly evaluated the skills of the participants for various paediatric procedures. At the end of the training, program participants were given credit hours equivalent to the number of hours spent in the training.
Analysis
Data were coded and entered in an Excel sheet and then imported to STATA software version 13.1, Stata Corp, College Station, Texas 77845 USA. Descriptive statistics such as frequency, percentage, mean, median, standard deviation and interquartile deviation were used to analyse data. Paired t-test was used to compute the difference in knowledge and confidence scores between pre-test and post-test values. The set level of significance for inferential statistics was taken as <0.05.
RESULTS
A total of 282 nurses from a given list of 300 completed the needs assessment survey. There were 18 dropouts in the study due to various reasons such as being on medical leave,[4] not completing the need assessment survey[8] and being on night duty.[6] The final sample size was 282 [Figure 2]. The mean age of the participants was 32.1 ± 6.5 years. A majority (68.1%) of them were female and had a bachelor’s degree in nursing (68.1%) with median years of professional experience of 8 years. Most of them (85.1%) did not have prior experience working in paediatric areas and only a small proportion of the nurses (18%) had undergone online training related to COVID-19 during the past 6 months. A majority of them (89.4%) had worked in COVID-19 units having a median work experience of 1 year. Most of them preferred resource materials in the form of videos (70%), while only 25% wanted reading materials.
There was a significant improvement in the level of knowledge (12.57 ± 2.96 and 16.34 ± 4.26, P = 0.001) and the self-reported confidence (84.08 ± 18.20 vs. 106.65 ± 9.86, P < 0.001) of the participants in performing paediatric nursing skills after the training program [Table 2]. A mean rating score of 4.4 or more, out of five, was given by the participants on the quality of the resource material shared on the Telegram app, the relevance of the skills taught, the quality of the hands-on training and the likelihood of recommending the course to a colleague [Table 2]. Self-reported level of confidence towards performing the paediatric skills is given in [Table 3]. No association could be established between knowledge level and the qualification and total professional experience of the participants (P > 0.05). Preceptors rated the majority of participants competent for the observed skills [Table 4]. All the experts (42) and the preceptors (16) enjoyed interacting with nurses and giving demonstrations to the participants in small groups. All experts opined that the hybrid model of teaching saved their time in training the nurses in paediatric COVID-19 preparedness. They all recommended the use of the SDP model in the future training of healthcare workers of various levels. The preceptors did not feel any increase in the workload while supervising the participants during the training program.
| Pre-intervention scores mean±SD | Post-intervention scores mean±SD | P-value | |
|---|---|---|---|
| Knowledge | 12.57±2.96 | 16.36±4.26 | 0.001 |
| Confidence | 84.08±18.20 | 106.65±9.86 | 0.001 |
| Feedback of the participants | Mean | ||
| Quality of resource materials shared in telegram | 4.5 | ||
| Relevance of skills taught | 4.5 | ||
| Rating of hands-on training | 4.5 | ||
| Overall benefit from the course | 4.6 | ||
| Likelihood of recommending the course to colleagues | 4.8 | ||
Scores range=1–5. SD: Standard deviation, n: Number of nurses
| Paediatric nursing skills | Pre-test (n=282) Median(Q1, Q3) |
Post-test (n=282) Median(Q1, Q3) |
P-value |
|---|---|---|---|
| Triaging of children | 3 (3, 4) | 5 (4.5) | 0.001 |
| Checking blood glucose in children | 4 (4, 5) | 5 (5.5) | 0.001 |
| Monitoring of a sick child-vitals, CFT and SpO2 | 4 (4, 5) | 5 (5.5) | 0.001 |
| Oro-pharyngeal suctioning | 4 (3, 5) | 5 (5,5) | 0.001 |
| Positioning a child for open airway | 4 (3, 4) | 5 (4.5) | 0.001 |
| Endotracheal suctioning | 4 (3, 5) | 5 (5.5) | 0.001 |
| Use of low-flow oxygen delivery devices-nasal prong, face mask | 4 (4, 5) | 5 (5.5) | 0.001 |
| Use of high-flow oxygen delivery devices-NRM, HFNO | 4 (3, 4) | 5 (4, 5) | 0.001 |
| Taking care of a child on non-invasive mechanical ventilation | 3 (3, 4) | 5 (4, 5) | 0.001 |
| Taking care of a child on invasive mechanical ventilation | 3 (3, 4) | 5 (4, 5) | 0.001 |
| Assisting in ET intubation | 4 (3, 4) | 5 (4, 5) | 0.001 |
| OG/NG tube insertion and feeding | 4 (3, 4) | 5 (4, 5) | 0.001 |
| Drug dosage calculation, drop factor in paediatrics | 4 (3, 4) | 5 (5, 5) | 0.001 |
| Insertion of IV line | 3 (3, 4) | 5 (4, 5) | 0.001 |
| Nebulisation | 4 (4, 5) | 5 (5, 5) | 0.001 |
| Fluid therapy | 4 (3, 4) | 5 (5, 5) | 0.001 |
| Blood and component therapy | 4 (3, 4) | 5 (4, 5) | 0.001 |
| Paediatric basic life support | 3 (3, 4) | 5 (4, 5) | 0.001 |
| Assisting in CPR | 4 (3, 4) | 5 (4, 5) | 0.001 |
| Proning of a paediatric COVID patient | 4 (3, 4) | 5 (4, 5) | 0.001 |
| Using radiant warmer | 4 (3, 4) | 5 (5, 5) | 0.001 |
| Using syringe pump | 4 (4, 5) | 5 (5, 5) | 0.001 |
| Handling CPAP/BIPAP/Ventilator | 3 (3, 4) | 5 (4, 5) | 0.001 |
Mann–Whitney U-test, P<0.05 (Level of significance ). COVID: Coronavirus disease, PNEPPCO: Paediatric nursing emergency preparedness program for COVID-19, SpO2: Oxygen saturation, NRM: Non-rebreather mask, HFNO: High-flow nasal oxygen, ET: Endotracheal tube, OG/NG: Orogastric/Nasogastric, CPR: Cardiopulmonary resuscitation, CPAP: Continuous positive airway pressure, BIPAP: Bi-level positive airway pressure, CFT: Capillary filling time, IV: Intravenous, n: Number of nurses
| Skills | Competent (f) | Less competent (f) | Needs improvement (f) |
|---|---|---|---|
| Checking vital signs (n=90) | 90 | - | - |
| Checking oxygen saturation (n=90) | 89 | 1 | - |
| Checking blood glucose (n=90) | 81 | 9 | - |
| Sample collection (n=81) | 81 | - | - |
| Proning of a sick child (n=42) | 33 | 6 | 3 |
| Assisting in resuscitation (n=57) | 53 | 1 | 3 |
| Oral and oropharyngeal suctioning (n=48) | 40 | 3 | 5 |
| Insertion of guedel airway (n=70) | 68 | 1 | 1 |
| Administering oxygen using nasal prongs (n=35) | 30 | 1 | 4 |
| Administering oxygen using simple face mask (n=81) | 80 | 1 | 0 |
| Administering oxygen using NRM (n=76) | 75 | - | 1 |
| Administering oxygen using Venturi mask (n=42) | 40 | 1 | 1 |
| Administering oxygen using HFNO (n=38) | 37 | 1 | 0 |
| Assisting in endotracheal intubation (n=58) | 54 | 3 | 1 |
| Inline endotracheal suctioning (n=46) | 35 | 4 | 7 |
| Care of a child on non-invasive ventilation (Nasal CPAP/NIV) (n=46) | 44 | 1 | 1 |
| Care of a child on invasive ventilation (n=60) | 52 | 6 | 2 |
| NG/OG tube insertion (n=61) | 56 | 2 | 3 |
| NG/OG tube feeding (n=48) | 38 | 4 | 6 |
n: Number of observations. NIV: Non-invasive ventilation, NRM: Non-rebreather mask, HFNO: High-flow nasal oxygen, CPAP: Continuous positive airway pressure, NG/OG: Nasogastric/Orogastric, f: Frequency
DISCUSSION
Nurses are the frontline COVID warriors, the first ones to respond in repeated surges of the COVID pandemic affecting a larger proportion of children.[11] Nursing care of children is entirely different from adults. Children affected by COVID-19 need specialised care by nurses trained in paediatric care. Most of the nurses who were then working in the COVID centre did not have any previous experience in caring for sick children other than their pre-service training. The SDP model can be effective in resource-constrained countries like India during the on-going COVID pandemic. The model encouraged the use of self-study, demonstration and preceptorship used in small groups. The role of nurse preceptor is well established in many countries,[12,13] but is relatively a newer concept in India. In a multicentric survey, the majority of healthcare workers reported having low awareness, confidence and preparedness in handling patients with COVID-19.[14] We also had a similar finding in our study before the training program in the pre-intervention phase. The nurses felt anxious, not prepared well and expressed their concerns when faced with high-consequence infectious diseases like COVID-19.[14,15] The healthcare workers (HCWs) have expectations for training from the authorities to prepare themselves for dealing with COVID-19.[15] Therefore, it is of utmost importance that need-based training is arranged for the HCW on a regular basis.[16] In the present study, we made use of an SDP model having the amalgamation of SDP. The participants were highly satisfied with the quality of the resource material, relevance of the skills taught, hands-on training and overall benefit of the course. They were confident in performing skills and recommended the training to their colleagues. The results of the present study are in congruence with the findings of some studies in which the blended learning approach was used;[17,18] however, these studies did not have the concept of preceptorship. The present study is the first of its kind, in which we introduced the concept of preceptorship in a training program. The preceptors were experienced senior nursing officers, having expertise in managing paediatric and neonatal cases. All the participants worked under the guidance of preceptors before being evaluated for the learned skills. Evaluation of the skills of the nurses was done by preceptors, who did not have any involvement in the training program. Our SDP training model was based on adult learning principles such as need-based learning, self-paced learning, mutual respect and autonomy for the learner. The multidisciplinary team of trainers also ensured that the doubts and queries of the participants were addressed holistically. The involvement of all stakeholders in the training projected a deep sense of investment in the training and appropriately influenced the learning environment. The majority of our participants preferred to watch videos for self-learning followed by reading materials, with only a few of them opting for the recorded webinars in the need assessment phase. Keeping this in mind, we prepared the resource materials. An association between skill-based training and level of confidence has been reported in some studies.[19,20] Similarly, in our study, we observed an improvement in confidence in performing paediatric skills after the training. We received positive feedback about the training program from the participants. We took a 360° evaluation of the training program from all those who were involved in the training program. The entire course was paperless; the pre-test and post-test assessments and the feedback were taken online. In view of the enhancement of knowledge and self-confidence level of the participants, the SDP model can be used to bridge the gap between knowledge and gaining the technical skills required for the management of children with COVID-19.
The major limitation of our study was the short duration of the training program. Informal feedback obtained from our participants showed that they wanted more time, at least 2 days for supervised practice in the lab. Unfortunately, this was not possible for us due to an urgent need to prepare a large number of nurses in managing paediatric COVID-19 cases. We also could not assess the impact of our training in attaining the skills of all the participants in the actual place of work, where the COVID patients were admitted. The study needs to be replicated in other settings to prove generalizability.
CONCLUSION
The SDP model with a blended learning approach and multidisciplinary team involvement led to improvement and knowledge and confidence among nurses working in a COVID-19 centre. Building the nursing staff ’s capacity to face the new challenges of COVID-19 in children would boost their knowledge and self-confidence and ensure the highest possible quality of patient care.
Acknowledgment
The authors would like to acknowledge the support of the entire medical team, secretarial staff and the simulation e-learning telemedicine (SET) facility and the preceptors for their contribution to the completion of the study.
What is already known?
Nurses are the frontline workers in the management of COVID-19 COVID-19 is a new highly infectious disease of the century The nurses need to be prepared in terms of enhancement of their knowledge and skills related to the management of COVID-19.
What does this paper add?
The SDP model intended to provide a framework, to be used for professional nursing education incorporated the core value of adult learning principles, and prepares nurses to learn the skills using demonstration and preceptorship to provide quality-based and individualised patient-centred care during the COVID-19 pandemic in a resource constraint country.
Ethical approval
Ethical permission was obtained from the Institute Ethics Committee (IEC letter no. IEC-550/06.08.2021, RP-23/2021).
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Healthcare Workers. 2020. Centers for Disease Control and Prevention. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/pediatric-hcp.html [Last accessed on 2021 Jul 13]
- [Google Scholar]
- COVID-19 in childhood: Transmission, clinical presentation, complications and risk factors. Pediatr Pulmonol. 2021;56:1342-56.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19 in children across three Asian cosmopolitan regions. Emerg Microbes Infect. 2020;9:2588-96.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://ncdc.gov.in/dashboard.php [Last accessed on 2021 Oct 01]
- 90% of those Killed by Covid in India are Older than 40 and 69% are Men. 2020. Hindustan Times. Available from: https://www.hindustantimes.com/india-news/90-of-those-killed-by-covid-in-india-are-older-than-40-69-are-men/story-glg0Ct4rHQ1YVvZgnckUcM.html [Last accessed on 2021 Oct 01]
- [Google Scholar]
- SARS-CoV-2 Infection in Children. N Engl J Med. 2020;382:1663-5.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19 and Your Health. 2020. Centers for Disease Control and Prevention. Available from: https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/children/symptoms.html [Last accessed on 2021 Jul 03]
- [Google Scholar]
- COVID-19: How it is Affecting Children and What Nurses can do to Help. 2020. RCNi. Available from: https://rcni.com/nursing-children-and-young-people/opinion/comment/covid-19-how-it-affecting-children-and-what-nurses-can-do-to-help-159566 [Last accessed on 2021 Jul 03]
- [Google Scholar]
- Clinical profile and risk factors for severe disease in 402 children hospitalized with SARS-CoV-2 from India: Collaborative Indian pediatric COVID study group. J Trop Pediatr. 2021;67:fmab048.
- [CrossRef] [PubMed] [Google Scholar]
- Hospital preparedness and management of pediatric population during COVID-19 outbreak. Ann Thorac Med. 2020;15:107-17.
- [CrossRef] [PubMed] [Google Scholar]
- Nurses on the frontline against the COVID-19 pandemic: An integrative review. Dubai Med J. 2020;3:87-92.
- [CrossRef] [Google Scholar]
- Nursing Management. Available from: https://journals.lww.com/nursingmanagement/fulltext/2020/03000/nurse_preceptors__a_valuable_resource_for_adapting.9.aspx [Last accessed on 2021 Jul 04]
- [Google Scholar]
- Clinical nurse preceptor teaching competencies: Relationship to locus of control and self-directed learning. J Nurs Res. 2012;20:142-51.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of healthcare workers' levels of preparedness and awareness regarding COVID-19 infection in low-resource settings. Am J Trop Med Hyg. 2020;103:828-33.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge, attitudes and practices of healthcare workers within an Australian tertiary hospital to managing high-consequence infectious diseases. Infect Dis Health. 2021;26:95-103.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19: The need for continuous medical education and training. Lancet Respir Med. 2020;8:e23.
- [CrossRef] [PubMed] [Google Scholar]
- E-learning in newborn health-a paradigm shift for continuing professional development for doctors and nurses. Indian J Pediatr. 2014;81:1376-80.
- [CrossRef] [PubMed] [Google Scholar]
- Online Neonatal Training and Orientation Programme in India (ONTOP-IN)--the way forward for distance education in developing countries. J Trop Pediatr. 2012;58:486-90.
- [CrossRef] [PubMed] [Google Scholar]
- Determinants of confidence in overall knowledge about COVID-19 among healthcare workers in South Africa: Results from an online survey. Front Public Health. 2021;9:614858.
- [CrossRef] [PubMed] [Google Scholar]
- Student self-confidence with clinical nursing competencies in a high-dose simulation clinical teaching model. J Nurs Educ Pract. 2016;6:52.
- [CrossRef] [Google Scholar]




