
Translate this page into:
Cooper’s 12 min run test: Its validity in Indian swimmers and volleyball players
*Corresponding author: Dr. Amit Bandyopadhyay, Sports and Exercise Physiology Laboratory, Department of Physiology, University of Calcutta, University Colleges of Science and Technology, 92 APC Road, Kolkata-700009 West Bengal, India. abphys@caluniv.ac.in
-
Received: ,
Accepted: ,
How to cite this article: Bandyopadhyay A. Cooper’s 12 min run test: Its validity in Indian swimmers and volleyball players. Indian J Physiol Pharmacol 2020;64(4):265-71.
Abstract
Objectives:
VO2max is globally considered as the gold standard to evaluate the cardiorespiratory fitness that is an essential component to judge one’s aerobic fitness level. The present study was aimed to enumerate the validity for application of Cooper’s 12 min run test (CRT) in predicting VO2max among Indian swimmers and volleyball players.
Materials and Methods:
Swimmers (male = 66, female = 70) and volleyball players (male = 88, female = 81) were recruited by simple random sampling from reputed clubs of Kolkata. They were segregated into study and confirmatory groups. VO2max was determined by graded incremental cycle ergometer test followed by expired gas analysis and indirect CRT method.
Results:
Predicted VO2max (PVO2max) showed significant difference with the directly measured VO2max (VO2max) in study groups of both sports. Limits of agreement between PVO2max and VO2max proved inapplicability of current CRT protocol in studied populations. Modified population specific equations were computed from significant correlation of VO2max with distance covered in Cooper run test. Application of these norms in confirmatory groups revealed insignificant difference between PVO2max and VO2max in both genders.
Conclusion:
Modified equations are validated for application of CRT in evaluating VO2max in swimmers and volleyball players of both genders of Kolkata, India.
Keywords
Cooper test
Swimmer
Volleyball
VO2max

INTRODUCTION
Maximum oxygen uptake or VO2max is one’s ability to transport maximum amount of oxygen to the exercising muscles during exhaustive work. It is globally considered as the gold standard of an individual’s cardiorespiratory fitness. It is also an important parameter to judge an athlete’s performance ability. Direct estimation of VO2max involves complicated experimental protocol that is exhaustive and time consuming.[1] It is also expensive and involves skilled personnel and several equipments. Thus, it is not possible to apply the procedure of direct estimation of VO2max outside the well-equipped laboratory infrastructure.[2] Therefore, it acts as a hindrance when large number of samples needs to be evaluated, especially in the field-based studies. Direct measurement of VO2max is also influenced by the motivation of the individual.[3] Therefore, it will be a good alternative to choose indirect simple procedure(s) for the evaluation of VO2max, especially in case of sportspersons to evaluate their cardiorespiratory fitness in the field and also in absence of favorable laboratory set up.[1,2]
The previous studies enumerated the validity of prediction of VO2max using non-exercise based models in Indian college students.[3,4] A study on Japanese adult population standardized 3 min walking distance for prediction of VO2max with respect to gender, age, and body composition.[5] Huntsman et al.[6] restricted the use of equipment by enumerating the applicability of a field test in rowers. Marsh[7] tried to assess the validity of the American College of Sports Medicine’s submaximal treadmill running test in predicting VO2max in moderately well-trained men of 18–34 years of age. Lima et al.[8] also standardized the 3200 m field test in Brazilian indoor soccer players. Klusiewicz et al.[9] have standardized another indirect protocol based on 2000 m trial that reflected the physical work capacity in terms of heart rate and that was further extrapolated with suitable regression norm in Polish rowers. All these studies emphasized that indirect protocols for VO2max prediction should be validated in the specific population before its implementation to enable the measurement of VO2max using simple methods with least instrumentation.
Cooper’s 12 min run test (CRT) is one of the popular indirect field tests for prediction of VO2max.[10] One measuring tape is required to measure the distance covered in 12 min. Application of this test in Indian sportspersons requires proper inventory of the validity of the test since it was originally enumerated in Western population.
Therefore, the present study was aimed to assess the suitability for application of the CRT to predict VO2max in male and female swimmers and volleyball players of Kolkata, West Bengal, India.
MATERIALS AND METHODS
Study population
Simple random sampling was adopted to recruit swimmers (male = 66 and female = 70) and volleyball players (male = 88 and female = 81) with similar socioeconomic background. They were selected from reputed clubs of Kolkata, West Bengal, India, and their age range was 20–25 years. The sample size was calculated by PS – Power and Sample Size Calculation version 3.0.43.[11] The confidence interval was set at 95%. The sample size thus calculated was 29 in each group. Considering 20% dropout, the adequate sample size was appeared to be 35. This study was conducted with more than this calculated number of samples in each group.
They were randomly separated into study group and confirmatory group. The existing protocol of CRT was tested on the study groups (Swimmers: Male = 36 and female = 40; volleyball players: Male = 58 and female = 51). Depending on the findings of the study group, necessary modification was made in the CRT norm and the modified norm was not only validated but also confirmed in the confirmatory group (Swimmers: Male = 30 and female = 30; volleyball players: Male = 30 and female = 30). After well explanation of the entire experimental protocol to all the participants, written informed consent was obtained from them. They were asked to take light breakfast 2–3 h before the test and were instructed to refrain from any energetic physical activity for that period. The participants had no history of any major disease and were not under any medication during the study. All the subjects were involved in regular training at least for the past 5 years. Subjects reported in the laboratory at 8 am on the days of evaluation. They were tested at the same time of the day to avoid any possibility of variation in results.
The whole experiment was performed during June 2018– March 2019. The room temperature and relative humidity during the entire experimental period varied between 22 and 35°C and 55–64%, respectively. The study was approved by the Institutional Human Ethical Committee.
Experimental design
Direct and indirect methods for the estimation of maximum oxygen consumption of each subject were performed by cross-over design (direct procedure was followed by indirect one in half of the subjects, whereas the indirect one was followed by direct one in other half of the subjects to avoid any possibility of bias). At least 4 days’ gap was maintained between these two trials. Resting and exercise heart rates were measured by Polar heart rate monitor (Polar H7, Polar, Canada). Subjects took rest for 30 min before the exercise so that pulmonary ventilation and pulse rate could come down to a steady state.[1,2]
Prediction of maximum oxygen uptake capacity (PVO2max) by CRT
Indirect prediction of VO2max was performed by applying CRT method which involved running exercise on a 400 m round track for a total duration of 12 min. Details of the protocol for application of CRT in male and female populations using the following equation are available elsewhere.[12,13]
VO2max (ml.kg-1.min-1) = (22.351 × Distance covered in kilometers) - 11.288
Direct measurement of maximum oxygen uptake capacity (VO2max)
Direct measurement of VO2max was performed by a graded incremental exercise test on cycle ergometer (model of Max Plank Institute, Dortmund, Germany) by following the standard separate protocol for male and female subjects.[12,13] Expired gas was collected at the last minute of the exercise when the subject became exhausted and an aliquot of the collected gas sample was analyzed in a Scholander microgas analysis apparatus following the standard procedure.[14]
Statistical analysis
Statistical analyses were computed using the Statistical Package for the Social Sciences (SPSS) version 21.0 (SPSS Incorp., United States). Paired t-test was undertaken to compute the significance of difference between mean values of VO2max and PVO2max. Data were expressed as mean±standard deviation (S.D). Unpaired t-test, Pearson’s product moment correlation, linear regression statistic, and Bland and Altman approach for limit of agreement analysis[15] were adopted for the statistical analysis of the data. Level of significance was set at P < 0.05.
RESULTS
Both the physical and physiological parameters of the subjects belonging to the two athletic populations of swimmers and volleyball players are shown in Table 1. Significant difference was found in body height, body weight, and distance covered in CRT when compared between the groups of same genders.
| Game | Gender group | Age (years) | Body weight (kg) | Body height (cm) | Pre-exercise heart rate (beats.min-1) | Blood pressure | Distance covered in CRT (km) | |
|---|---|---|---|---|---|---|---|---|
| Systolic (mm of Hg) | Diastolic(mm of Hg) | |||||||
| Swimmers | Male (n=66) | 22.86±1.66 | 65.37±4.27 | 172.26±4.29 | 67.42±4.65 | 104.51±6.35 | 64.79±6.24 | 3.210±0.188 |
| Female (n=70) | 23.25±1.53 | 59.03±4.78 | 168.21±3.28 | 64.54±5.43 | 100.51±5.42 | 61.52±5.92 | 2.997±0.185 | |
| Volleyball Players | Male (n=88) | 22.98±1.62 | 72.25±4.02** | 178.73±4.07** | 66.81±4.63 | 103.24±5.42 | 67.41±6.47 | 3.121±0.184* |
| Female (n=81) | 23.08±1.74 | 67.76±4.09## | 173.74±4.14## | 65.74±5.84 | 10173±6.71 | 64.65±6.12 | 2.933±0.181# | |
Values are mean±SD. *P<0.01, **P<0.001 when compared between male swimmers and volleyball players. #P<0.02, ##P<0.001 when compared between female swimmers and volleyball players
For the study groups of swimmers and volleyball players of both genders, Bland and Altman approach for limit of agreement analysis is plotted in Figures 1-4, respectively.

- Plotting of difference between PVO2max and VO2max values against the average of directly and indirectly measured values of VO2max in the study group of male swimmers.
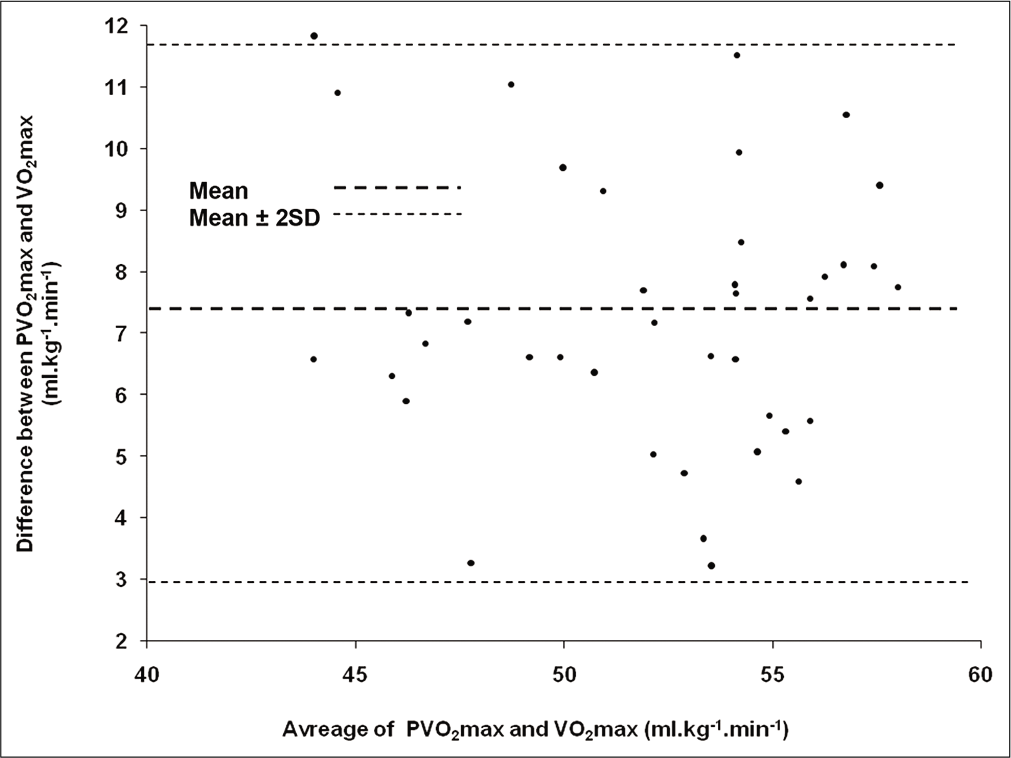
- Plotting of difference between PVO2max and VO2max values against the average of directly and indirectly measured values of VO2max in the study group of female swimmers.
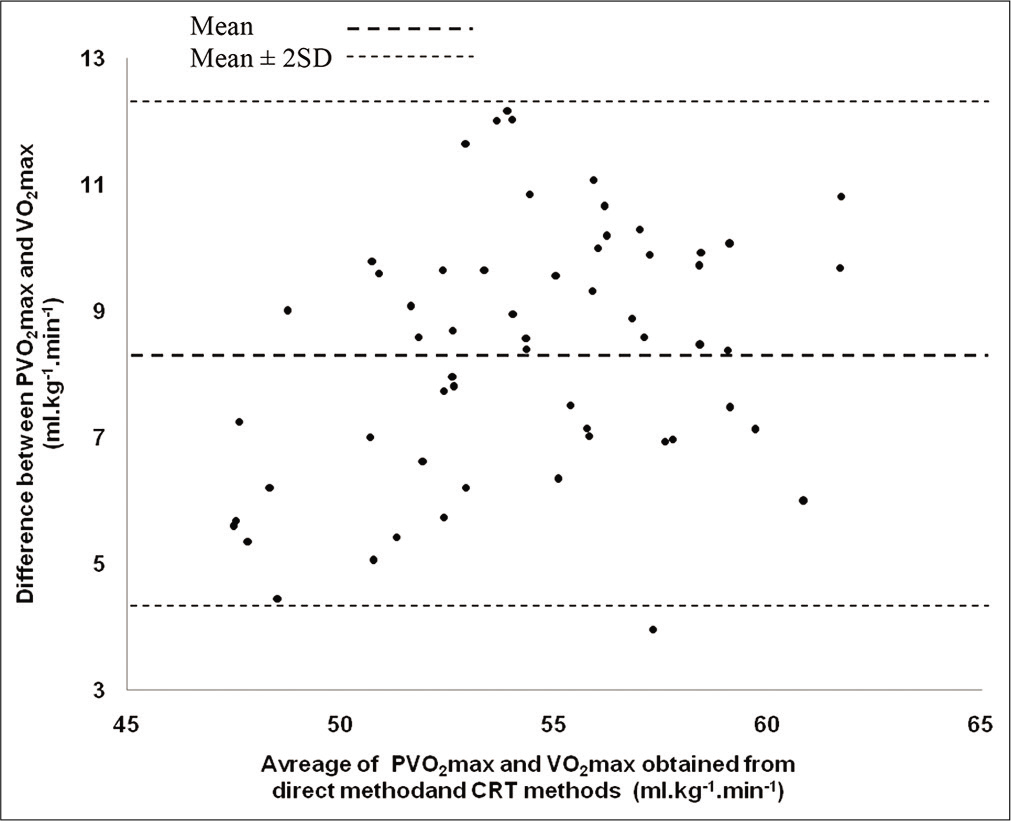
- Plotting of difference between PVO2max and VO2max values against the average of directly and indirectly measured values of VO2max in the study group of male volleyball players.
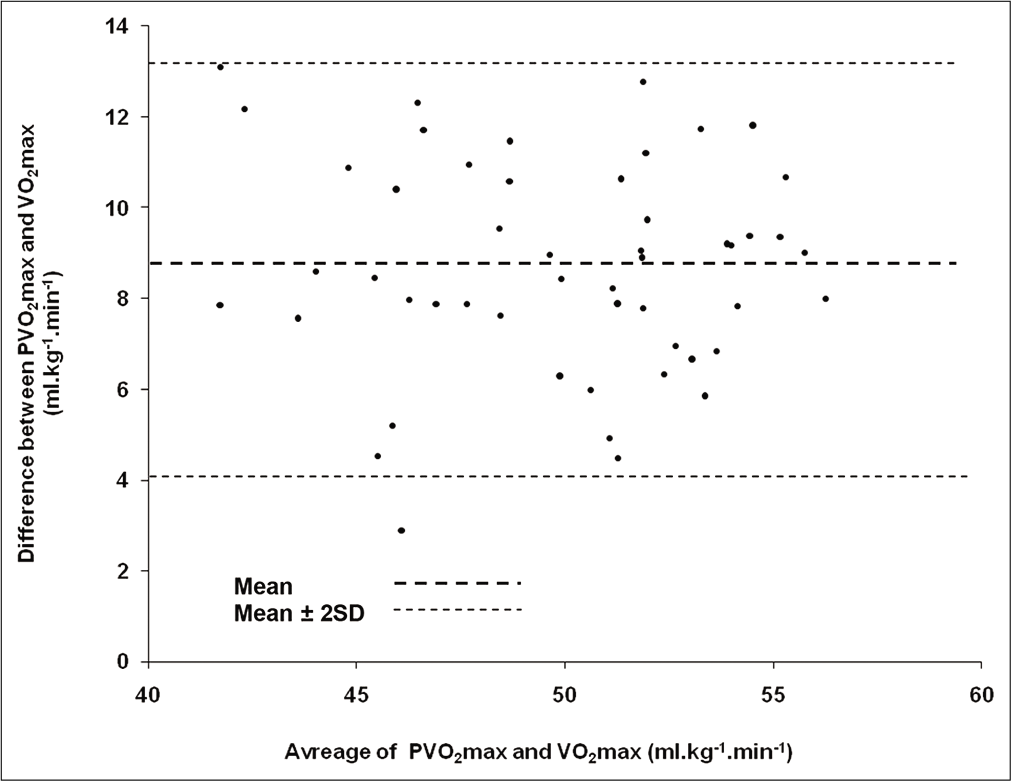
- Plotting of difference between PVO2max and VO2max values against the average of directly and indirectly measured values of VO2max in the study group of female volleyball players.
Based on the existence of significant correlation between VO2max and distance covered in CRT for the study groups of swimmers and volleyball players of both genders, regression equations have been computed and plotted in [Figures 5-8], respectively.
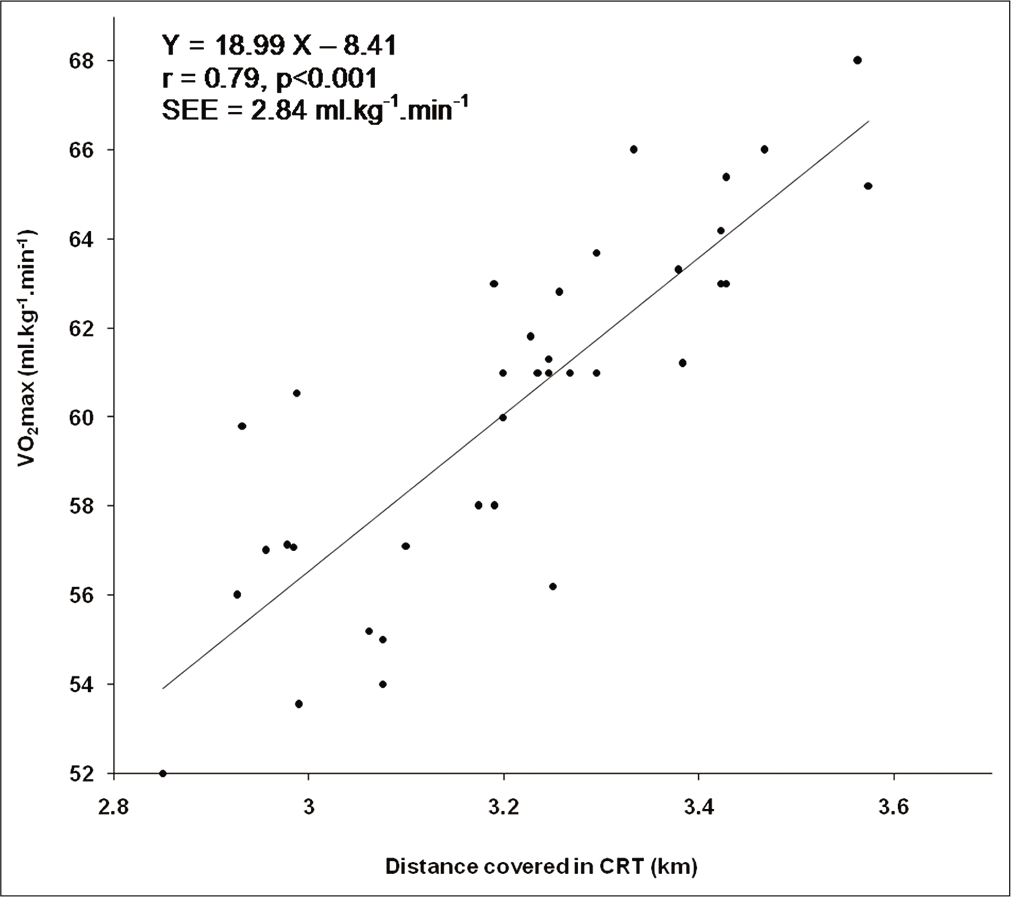
- Relationship between VO2max and distance covered in CRT in the study group of male swimmers.
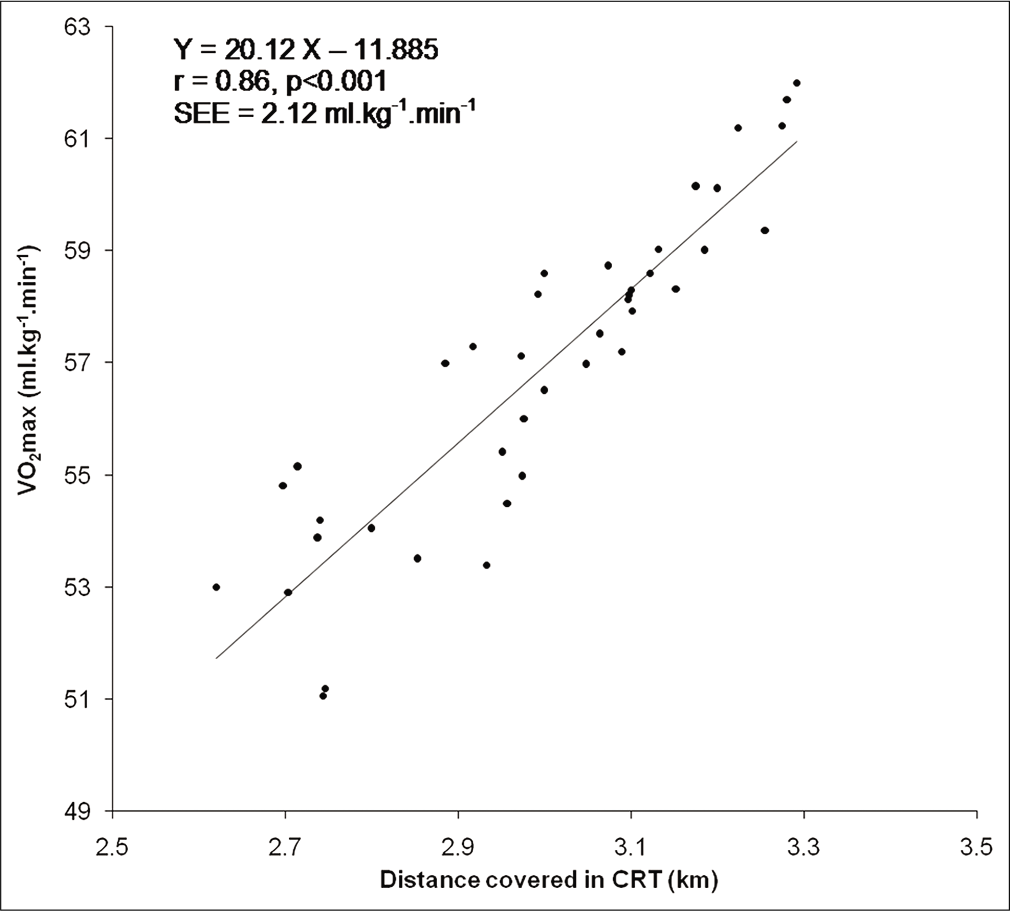
- Relationship between VO2max and distance covered in CRT in the study group of female swimmers.

- Relationship between VO2max and distance covered in CRT in the study group of male volleyball players.
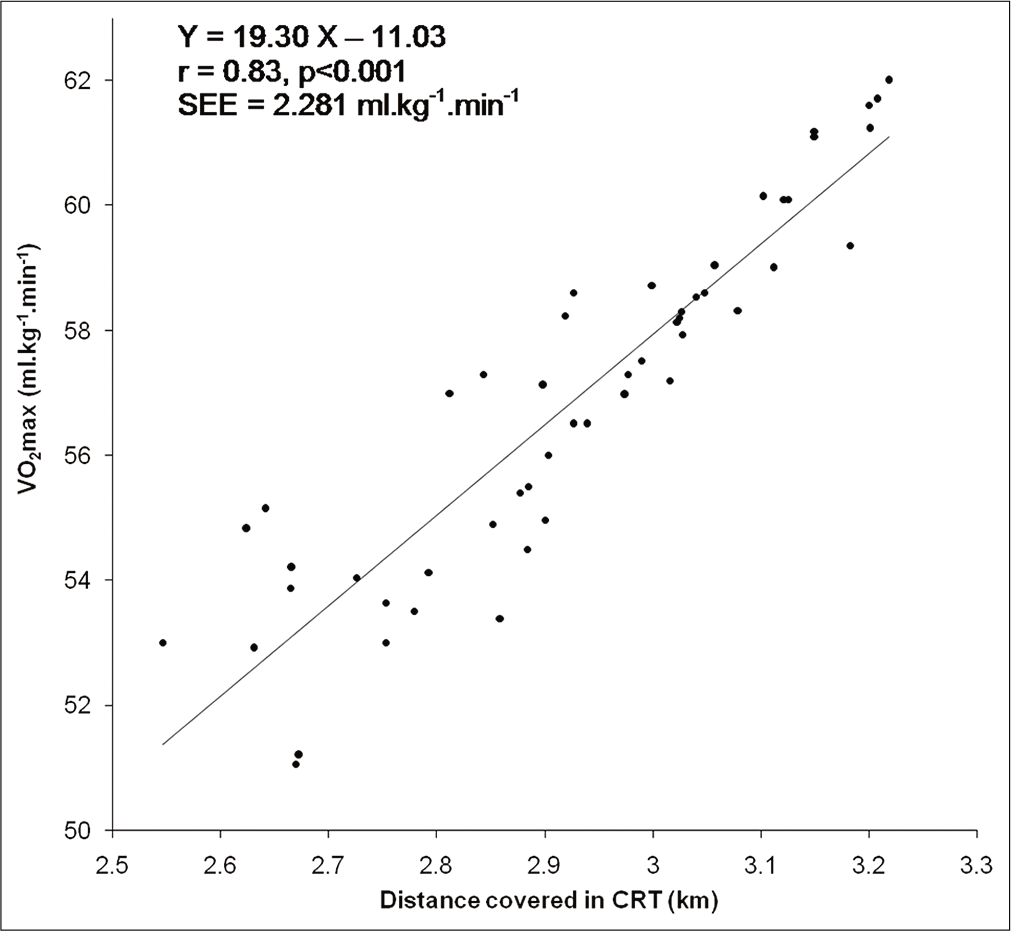
- Relationship between VO2max and distance covered in CRT in the study group of female volleyball players.
DISCUSSION
PVO2max (60.47 ± 4.20 ml.kg-1.min-1 in males and 55.70 ± 4.13 ml.kg-1.min-1 in females) of swimmers showed significant difference with VO2max (52.57 ± 4.53 ml.kg-1.min-1 in males and 48.40 ± 4.30 ml.kg-1.min-1 in females) in the study group. Bland and Altman[15] analysis revealed that the limits of agreement between PVO2max and VO2max were large enough (2.17–13.61 ml.kg-1.min-1 in males and 2.91–11.67 ml.kg-1.min-1 in females) with poor confidence intervals [Figures 1 and 2]. This finding indicated the inapplicability of current protocol of CRT for indirect prediction of VO2max in swimmers of Kolkata, India. Moreover, significant (P < 0.001) difference between PVO2max and VO2max indicated that application of the Cooper’s protocol[10] does not accurately predict maximum oxygen uptake in the studied population. However, the distance covered in CRT exhibited significant correlation (r = 0.79 in males and r = 0.86 in females, P < 0.001) with directly measured VO2max. Accordingly, prediction equations were computed in male (Y = 18.99 X – 8.41 [SEE = 2.84 ml.kg-1.min-1]) and female (Y = 20.16 X – 11.88 [SEE = 2.12 ml.kg-1.min-1]) swimmers from the data obtained in the study groups for precise assessment of VO2max in the studied population [Figures 5 and 6].
In case of the volleyball players, PVO2max (58.55 ±4.09 ml.kg-1.min-1 in males and 54.19 ± 4.01 ml.kg-1.min-1 in females) revealed significant difference with VO2max (50.19 ± 3.47 ml.kg-1.min-1 in males and 45.49 ± 4.12 ml.kg-1.min-1 in females) in the study group. Bland and Altman (1986) method of limit of agreement analysis revealed that the limits of agreement between PVO2max and VO2max were large enough (4.34–12.36 ml.kg-1.min-1 in males and 4.04–13.36 ml.kg-1.min-1 in females) with poor confidence intervals [Figures 3 and 4], indicative of unsuitability of current protocol of CRT in this particular population. Moreover, significant (P < 0.001) difference between PVO2max and VO2max marked that it would not be justified in accepting the prediction of maximum oxygen uptake in the studied population through CRT application as suggested by Cooper.[10] However, the distance covered in CRT depicted significant correlation (r = 0.87 in males and r = 0.83 in females, P < 0.001) with directly measured VO2max in the study group of both genders, and accordingly, regression norms were computed in male (Y = 16.55 X – 1.49 [SEE = 1.724 ml.kg-1.min-1]) and female (Y = 19.30 X – 11.03 [SEE = 2.281 ml.kg-1.min-1]) volleyball players depending on the data obtained in the study groups for precise prediction of VO2max in the studied population [Figures 7 and 8].
The newly derived equations were applied in the confirmatory group of both the genders of swimmers. This revealed insignificant difference between PVO2max (53.12 ± 3.48 ml.kg-1. min-1 in males and 49.73 ± 3.73 ml.kg-1.min-1 in females) and VO2max (52.71 ± 3.34 ml.kg-1.min-1 in males and 48.87 ± 3.87 ml.kg-1.min-1 in females). Moreover, the standard errors of estimate of these norms were substantially small (SEE = 2.84 ml.kg-1.min-1 and 2.12 ml.kg-1.min-1 in male and female groups, respectively). Prediction of VO2max from this new equation showed a variation of <5% in 52 male and 55 female participants, 5–9% in 8 male and 11 female participants, 10–14% in 4 male and 3 female participants, and 15–19% in 2 male and 1 female participants from their respective directly measured value of VO2max. Application of Bland and Altman’s analysis between directly measured VO2max and indirectly predicted VO2max from the newly derived equation revealed substantially small limits of agreement in male (–0.19–1.51 ml.kg-1.min-1) and female (–0.05–1.85 ml.kg-1. min-1) groups. The percentage of variation between VO2max and PVO2max reduced from 15.03% to 0.77% in male swimmers and from 15.08% to 1.76% in female swimmers following application of the revised population-specific equations.
Further, in case of the volleyball players, application of these newly derived equations in the confirmatory group indicated insignificant difference between PVO2max (49.68 ± 3.73 ml.kg-1.min-1 in males and 47.72 ± 3.64 ml.kg-1.min-1 in females) and VO2max (50.29 ± 4.03 ml.kg-1.min-1 in males and 46.57 ± 3.75 ml.kg-1.min-1 in females). Moreover, the standard errors of estimate of these norms were substantially small (SEE = 1.724 ml.kg-1.min-1 and 2.281 ml.kg-1.min-1 in male and female groups, respectively). Prediction of VO2max from this new equation showed a variation of <5% in 62 male and 59 female participants, 5–9% in 18 male and 15 female participants, 10–14% in 5 male and 5 female participants, and 15–19% in 3 male and 2 female participants from their respective directly measured value of VO2max. Application of Bland and Altman’s analysis between directly measured VO2max and indirectly predicted VO2max from the newly derived equation revealed substantially small limits of agreement in male (0.16–1.76 ml.kg-1.min-1) and female (0.06–1.06 ml.kg-1.min-1) groups. The percentage of variation between VO2max and PVO2max reduced from 16.65% to 1.21% in male volleyball players and from 19.12% to 0.24% in female volleyball players following application of the revised population-specific equations. This variation should be within a range of 7% for the acceptability of the modified norm.[16] The criterion has been satisfied in the present investigation.
The exercise protocol of the modified method remains the same, but the regression equation has been modified in different genders of swimmers and volleyball players on the basis of proper statistical analyses. These are the population-specific corrections of the regression norm as also reported in the earlier studies dealing with standardization of indirect protocols for the valid prediction of VO2max.[1,2,12,13]
Variation of results between the original equation and presently modified equation was perhaps due to the fact that the original equation was proposed in sedentary Western population while the present study involved swimmers and volleyball players from Kolkata, West Bengal, India. There is a variation in the ethnicity as well as physical fitness level which might be potential reasons for the inapplicability of the existing protocol in the currently studied sportspersons of both genders.
Bland and Altman’s guideline[15] was adopted to test the repeatability of the modified equations in the studied population. It has been observed that the mean difference between repeated measures of VO2max (determined by both direct method and indirect modified method) was insignificantly different from zero in both the genders of swimmers. As per the definition of “Repeatability Coefficient,”[17] it is expected that 95% of differences would be less than two SDs (±2SDs) which has been met in the present investigation. The SDs between repeated measures of each method separately were computed and the SDs of differences between the means for each method were also computed to determine the repeatability coefficients in both the genders for direct method and indirectly modified method. The mean differences of repeated measures were 0.0052 ml.kg-1.min-1 and 0.0061 ml.kg-1.min-1 for modified equations in males and females, respectively, whereas 0.0043 ml.kg-1.min-1 and 0.0049 ml.kg-1.min-1 for direct method in males and females, respectively. The corresponding values of repeatability coefficients were ±0.42 ml.kg-1.min-1, ±0.46 ml.kg-1.min-1, ±0.48 ml.kg-1.min-1, and ±0.43 ml.kg-1.min-1, respectively.
Further, for volleyball players, repeatability of the modified equations has also been tested according to the guideline of Bland and Altman.[11] It has been observed that the mean difference between repeated measures of VO2max (determined by both direct method and indirect modified method) was insignificantly different from zero in both the genders of volleyball players. According to the definition of “Repeatability Coefficient.”[12] It is expected that 95% of differences would be ±2SDs which has been met in the present investigation. The SDs between repeated measures of each method separately were computed and the SDs of differences between the means for each method were also computed to determine the repeatability coefficients in both the genders for direct method and indirectly modified method. The mean differences of repeated measures were 0.0058 ml.kg-1.min-1 and 0.0065 ml.kg-1.min-1 for modified equations in males and females, respectively, whereas 0.0049 ml.kg-1.min-1 and 0.0054 ml.kg-1.min-1 for direct method in males and females, respectively. The corresponding values of repeatability coefficients were ±0.53 ml.kg-1.min-1, ±0.56 ml.kg-1.min-1, ±0.52 ml.kg-1.min-1, and ±0.58 ml.kg-1.min-1, respectively.
CONCLUSION
From the present observation, it may be concluded that the presently derived or modified equations will predict VO2max in the studied populations more accurately. Therefore, these newly derived norms, validated against direct measurement of VO2max using incremental cycle ergometer test, are recommended for the application of Cooper’s 12 min run test as a valid method for correct and precise evaluation of cardiorespiratory fitness in terms of VO2max in swimmers and volleyball players of both genders of Kolkata, West Bengal, India.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Validity of Queen's College step test for use with young Indian men. Br J Sports Med. 2004;38:289-91.
- [CrossRef] [PubMed] [Google Scholar]
- Validity of Queen's College step test for estimation of maximum oxygen uptake in female students. Indian J Med Res. 2005;121:32-5.
- [Google Scholar]
- Concurrent validity of the non-exercise based VO2max prediction equation using percentage body fat as a variable in Asian Indian adults. Sports Med Arthrosc Rehabil Ther Technol. 2012;4:34.
- [CrossRef] [PubMed] [Google Scholar]
- Development of non-exercise based VO2max prediction equation in college-aged participants in India. J Sports Med Phys Fitness. 2012;52:465-73.
- [Google Scholar]
- Prediction of maximal oxygen uptake from a 3-minute walk based on gender, age, and body composition. J Phys Act Health. 2013;10:280-7.
- [CrossRef] [PubMed] [Google Scholar]
- Development of a rowing-specific VO2max field test. J Strength Cond Res. 2011;25:1774-9.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the American College of sports medicine submaximal treadmill running test for predicting VO2max. J Strength Cond Res. 2012;26:548-54.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation between direct and indirect VO2max measurements in indoor soccer players. Rev Bras Med Esporte. 2005;11:159-61.
- [CrossRef] [Google Scholar]
- Indirect methods of assessing maximal oxygen uptake in rowers: Practical implications for evaluating physical fitness in a training cycle. J Hum Kinet. 2016;50:187-94.
- [CrossRef] [PubMed] [Google Scholar]
- A means of assessing maximal oxygen intake. Correlation between field and treadmill testing. J Am Med Assoc. 1968;203:201-4.
- [CrossRef] [PubMed] [Google Scholar]
- Power and sample size calculation for studies involving linear regression. Control Clin Trials. 1998;19:589-601.
- [CrossRef] [Google Scholar]
- Validity of Cooper's 12-minute run test for estimation of maximum oxygen uptake in male university students. Biol Sport. 2015;32:59-63.
- [CrossRef] [PubMed] [Google Scholar]
- Validity of Cooper's 12-min run test for estimation of maximum oxygen uptake in female university students. Indian J Physiol Pharmacol. 2014;58:184-6.
- [Google Scholar]
- Analysis of gas samples In: Samuel J, Hansfield S, eds. Physiological Measurements of Metabolic Functions in Man (2nd ed). New York: McGraw-Hill Book Company; 1963. p. :507-10.
- [Google Scholar]
- Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307-10.
- [CrossRef] [Google Scholar]
- Guidelines for Exercise Testing and Prescription (7th ed). Baltimore, MD: Lippincott Williams and Wilkins Company; 2006.
- [Google Scholar]
- Precision of Test Methods-Part 1: Guide for the Determination and Reproducibility for a Standard Test Method by Inter-Laboratory Tests (BS 5497) 1975
- [Google Scholar]




