
Translate this page into:
Correlation between clinical outcome and nerve conduction studies before and after surgery in patients with carpal tunnel syndrome
*Corresponding author: Debanjana Chowdhury, Department of Physiology, Calcutta National Medical College, Kolkata, West Bengal, India. debanjanachowdhury87@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Chowdhury D, Sen S. Correlation between clinical outcome and nerve conduction studies before and after surgery in patients with carpal tunnel syndrome. Indian J Physiol Pharmacol. 2024;68:325-34. doi: 10.25259/IJPP_403_2023
Abstract
Objectives:
In this study, we aimed to establish the correlation between clinical outcomes using a self-administered Boston carpal tunnel questionnaire (BCTQ) and nerve conduction studies (NCSs) before and after carpal tunnel release (CTR) operation in moderate, severe and extreme groups of patients. In prevalent literature, we found conflicting reports regarding the correlation, so we undertook this study to get a clear concept of the correlation between BCTQ and NCS.
Materials and Methods:
Thirty-two patients (39 hands) of carpal tunnel syndrome (CTS) were subdivided into three categories: Group I is moderate CTS (n = 9 hands), Group II is severe CTS (n = 14 hands) and Group III is extreme CTS (n = 16 hands). We evaluated electrophysiological parameters using both conventional motor parameters such as distal motor latency (DML), forearm conduction velocity (FMCV) and short-segment NCS parameter – transcarpal motor conduction velocity (TMCV) in pre-surgical and 6- and 9-month’s post-operative patients. The correlation between BCTQ consisting of symptom severity scale (SSS), functional status scale (FSS), and NCSs before and after CTR was assessed using Spearman rank correlation coefficients to establish the importance of CTR as the most effective treatment modality for CTS patients.
Results:
We found a significant correlation between BCTQ parameters – SSS and FSS and motor NCS parameters – DML, FMCV and TMCV in all three groups of CTS patients preoperatively, but the Spearman correlation coefficient value decreased and became statistically non-significant after 6 and 9 months of CTR operation. The BCTQ parameters SSS and FSS are influenced by the subjective information provided by the patients, whereas NCS is the objective and quantitative method to evaluate the condition of the median nerve. Moreover, NCS should be included in the post-operative follow-up to eliminate the possibility of recurrence, inadequate release of transverse ligament compressing the median nerve, and presence of other similar pathology or post-CTR complications.
Conclusion:
We can, therefore, conclude that clinicians should use BCTQ and NCS together to ascertain the success of CTR operation.
Keywords
Carpal tunnel syndrome
Nerve conduction study
Correlation
Boston carpal tunnel questionnaire

INTRODUCTION
Carpal tunnel syndrome (CTS), first described by Paget in 1854, is the most prevalent focal peripheral neuropathy caused by excessive pressure on the median nerve at the wrist.[1] Although clinical manifestations (paresthesia, numbness, tingling, wrist pain, thenar muscle atrophy and weakness along the median nerve distribution of hand) and physical findings (positive Phalen’s test and Tinel’s sign) are used to diagnose CTS, nerve conduction study (NCS) is the most accurate method for diagnosing median nerve abnormalities which help to decide the treatment plan (conservative or surgery) and to predict the prognosis after carpal tunnel release (CTR) operation.[2]
Reviewing the available literature,[3-9] it appears that to date, no proper correlation is delineated between clinical improvement and electrophysiological findings. The conventional NCS parameters such as distal motor latency (DML), distal sensory latency (DSL) and sensory nerve conduction velocity (SNCV) used in the past did not reflect the nerve impairment distal to the block. We undertook this study to evaluate the correlation between subjective symptoms and function indices compared to electrophysiological measures by comparing the self-administered Boston carpal tunnel questionnaire (BCTQ) consisting of symptom severity scale (SSS) and functional status scale (FSS)[10] against NCSs before and after CTR operation using conventional NCS and short-segment transcarpal techniques.
In our previous study, we have already shown that short-segment transcarpal motor conduction velocity (TMCV) is the most effective way to evaluate the condition of the median nerve after CTR[11] as neurological impairment of the median nerve in the form of demyelination or axonal degeneration can be detected more precisely by the short segment rather than the long segment technique which is evident from different studies.[12-14]
MATERIALS AND METHODS
Study design
This study was performed on 32 female patients in the age group 30–60 years presenting symptoms of CTS who attended the department of plastic surgery for 1 year and 10 months in a tertiary hospital in India. The study was conducted on thirty-nine hands, and bilateral CTR was carried out on seven patients.
Subject inclusion criteria
The patients who were included in the study met the criteria described in our previous study.[11]
The patients (39 hands) were categorised into three groups as per the American Association of the Electrodiagnostic Medicine criteria.
Group I: Moderate CTS (n = 9 hands) having prolonged DML and DSL with moderate reduction of SNAP and CMAP,
Group II: Severe CTS (n = 14 hands) prolonged DML and DSL with non-recordable SNAP and severe reduction of CMAP amplitude and
Group III: Extreme CTS (n = 16 hands) non-recordable CMAP and SNAP and thenar muscles atrophy.
Subject exclusion criteria
Patients having ailments resulting in neuropathy, such as diabetes, hypothyroidism, end-stage renal disease, autoimmune diseases, using drugs like INH, antiepileptics, chemotherapy, exposure to heavy metals and history of past medical or surgical treatment of CTS, were excluded from the study.
NCS
NCS was performed using RMS NCV EMG EP MARK II with Aleron 201 electromyograph with RMS stimulator using standard protocol in all the patients during pre-surgical and 6—and 9-month post-operation. Room and skin temperature were maintained over the nerve in the range of 25°C–36°C and 34°C–38°C, respectively, to avoid the effect of lower temperature on prolonging latency, increasing amplitude, and reducing conduction velocity.
The conventional median NCSs were performed by recording compound muscle action potential (CMAP) from abductor pollicis brevis (ABP) by placing the recording electrode on the ABP muscle belly and a reference electrode on distal tendinous insertion (at the distal metacarpophalangeal joint of the thumb). Bipolar stimulation was applied at the wrist between the tendons of the flexor carpi radialis and palmaris longus and at the elbow just medial to the brachial artery.
While performing the wrist-palm motor conduction study (short segment trans carpal technique) – the conventional method was used to stimulate the median nerve at the wrist, while to stimulate the nerve in the palm, the cathode was kept on a line from the wrist to 1st metacarpal space toward wrist[4,5] while the anode was placed toward the base of 5th digit distally to avoid short latency recording which could result in inaccuracy of wrist palm median motor conduction velocity (W-P MCV) as described in our previous study.[11] Necessary precautions were taken while recording W-P motor conduction. Although TMCV is the most effective parameter in evaluating median nerve condition, it is technically difficult as there is a possibility of stimulation of the deep branch of the ulnar nerve while stimulating the recurrent motor branch of the median nerve in the palm.[11-14] We have to be extremely cautious about the change in thenar twitch (abduction to adduction of thumb) or any modification of CMAP waveform configuration.
NCS data
Analysation of the following parameters.
DML: DML of the median nerve was recorded by stimulating the nerve 3 cm proximal to the distal crease of the wrist.
Forearm motor conduction velocity (FMCV): FMCV was calculated by dividing the distance between two points of stimulation (wrist and elbow) by the latency difference between the two stimulation points.
TMCV: TMCV was calculated by dividing the distance between two points of stimulation (wrist and palm) by the latency difference between the two stimulation sites.
The placement of the electrodes and stimulation sites is shown in [Figure 1].
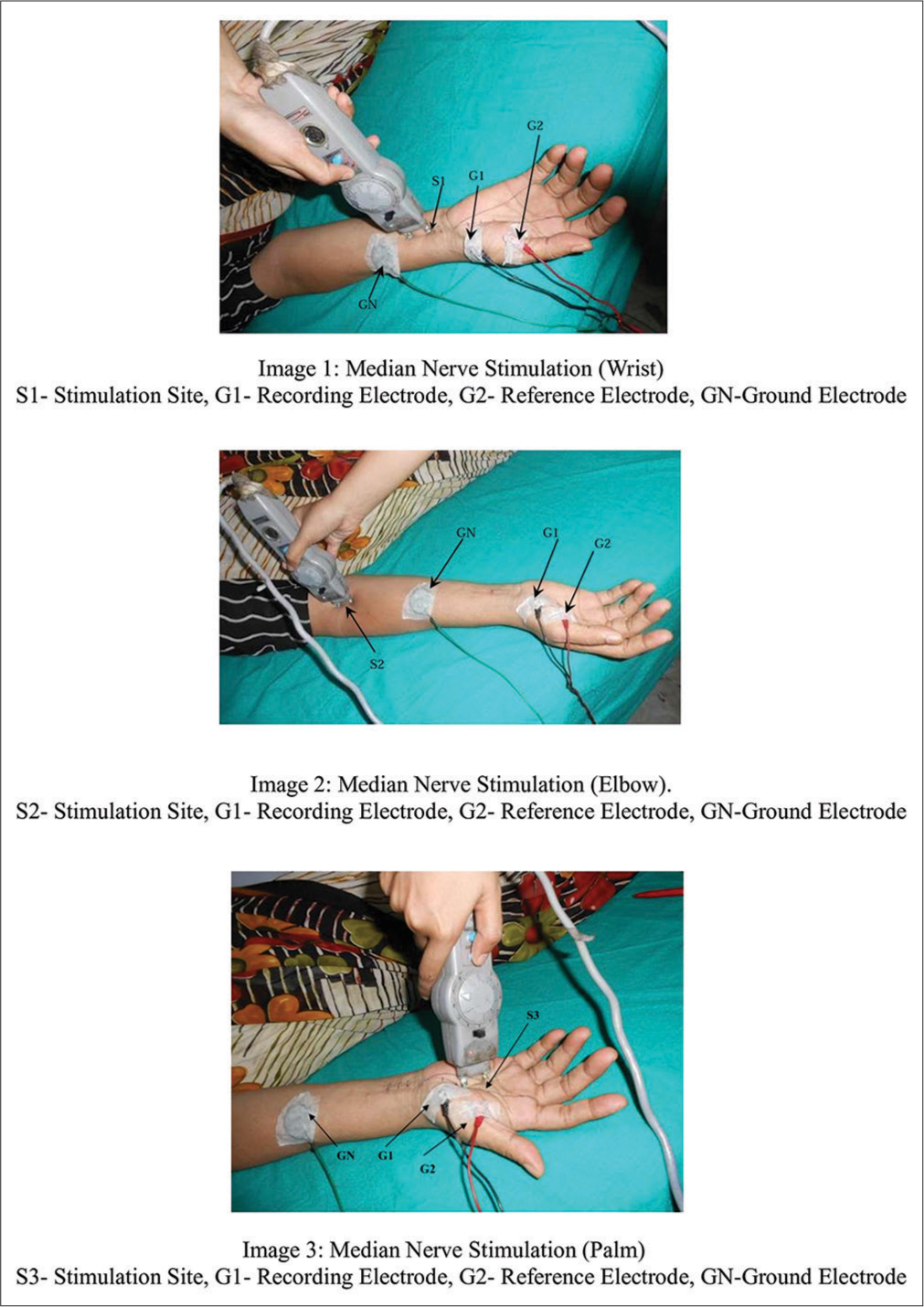
- Median nerve – motor nerve conduction study.
The Graphical representation of the temporal changes in NCV recordings in pre-operative, 6 months post-operative and 9 months post-operative follow up of all the 3 groups of patients - moderate (Group I), severe (Group II) and extreme (Group III) CTS are illustrated in Figures 2-4 respectively.
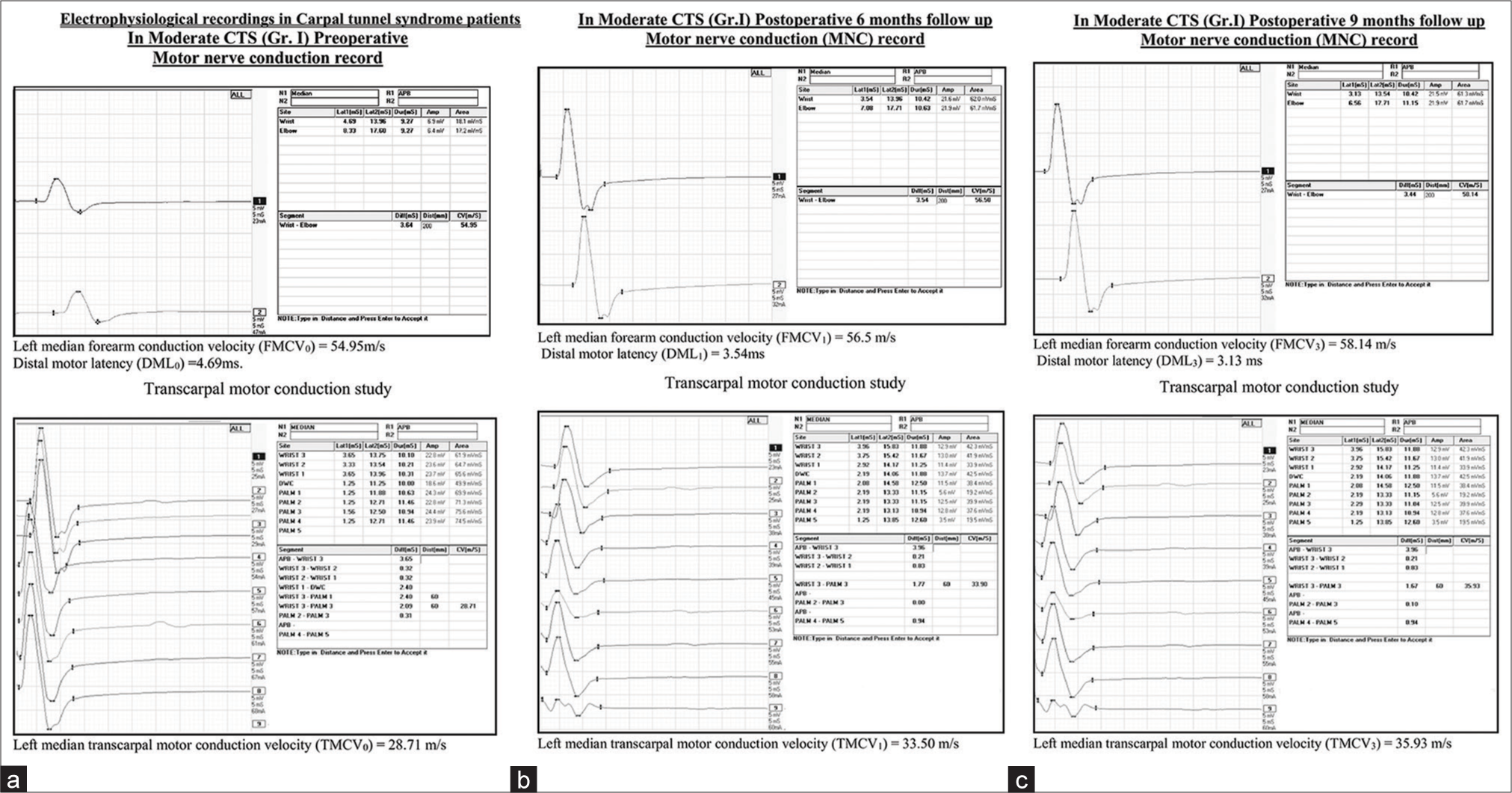
- (a) Pre-operative NCS in Group I moderate CTS patients. (b) Post-operative 6 months NCS in Group I moderate CTS patients. (c) Post-operative 9 months NCS in Group I moderate CTS patients. NCS: Nerve conduction study, CTS: Carpal tunnel syndrome.
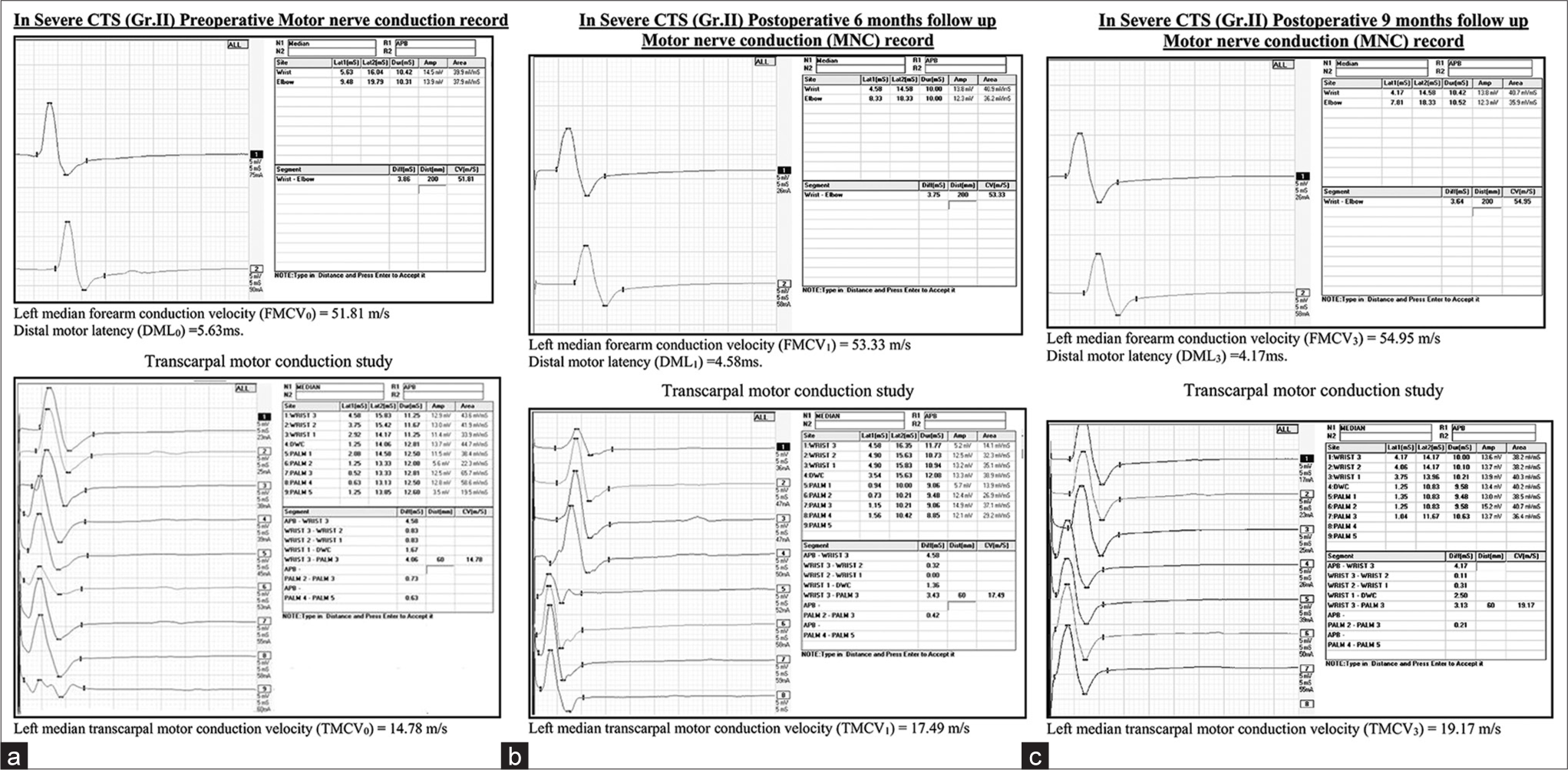
- (a) Pre-operative NCS in Group II severe CTS patients. (b) Post-operative 6 months NCS in Group II severe CTS patients. (c) Post-operative 9 months NCS in Group II severe CTS patients. NCS: Nerve conduction study, CTS: Carpal tunnel syndrome.
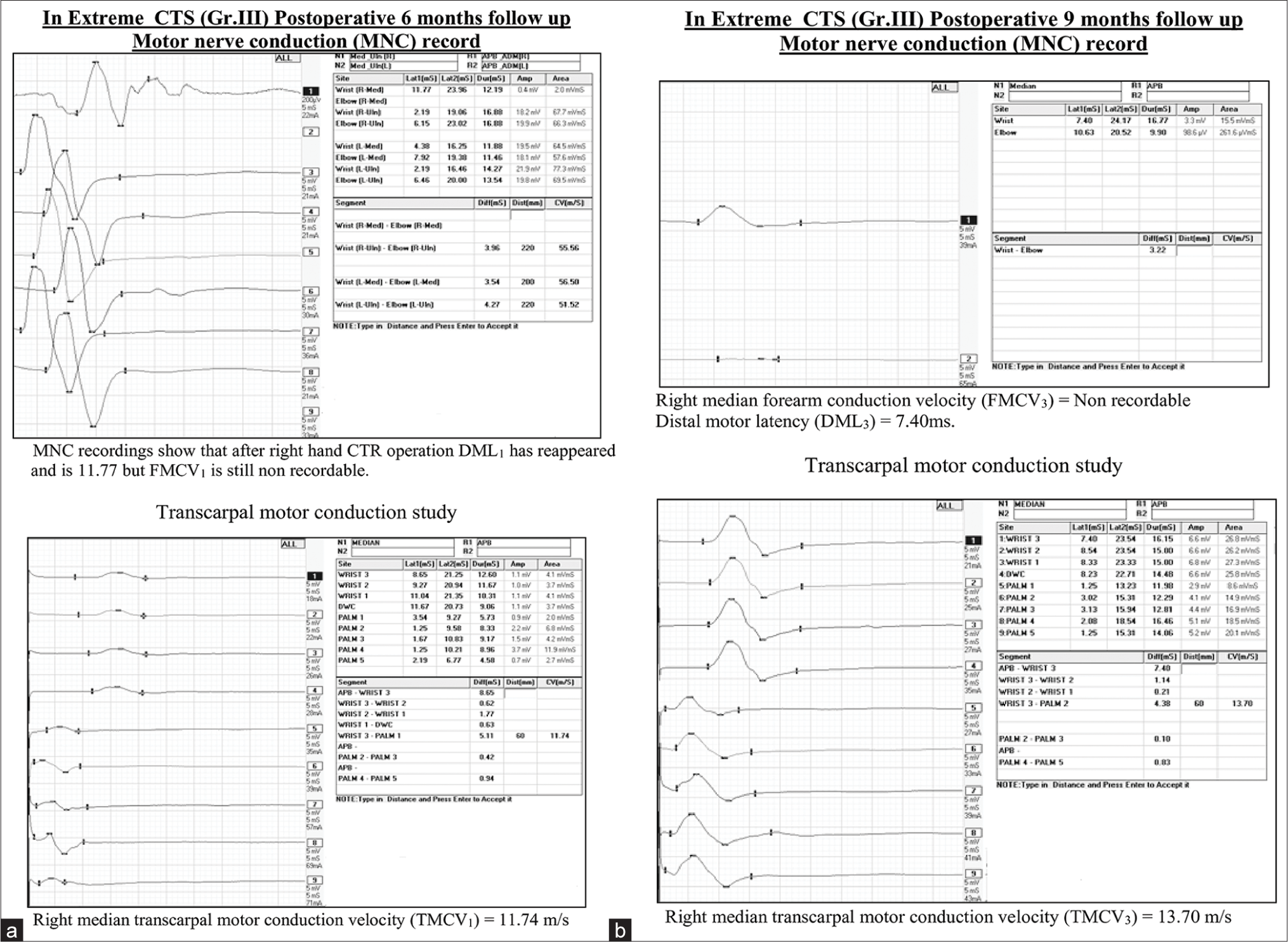
- (a) Post-operative 6 months NCS in Group III extreme CTS patients. (b) Post-operative 9 months NCS in Group III extreme CTS patients. NCS: Nerve conduction study, CTS: Carpal tunnel syndrome. NCS: Nerve conduction study, CTS: Carpal tunnel syndrome.
Clinical outcome
Assessment of severity of symptoms and functional impairment in patients with CTS was done with the help of the Boston self-administered questionnaire, [10] which comprises of:
SSS: It consists of 11 questions with multiple-choice responses to measure the severity of main complaints such as pain and paresthesia. Scores are calculated as the mean of 11 responses, ranging from 1 to 5 points, with higher scores indicating greater severity.
FSS: Made up of eight questions to assess the difficulty in performing daily activities. Scores are calculated as the mean of eight responses ranging from 1 to 5 points.
BCTQ was distributed among the patients before the operation and after 6 and 9 months of the operation, and their responses were recorded. In bilateral cases, separate questionnaires were administered.
Statistical analysis
Quantitative data are presented with mean and standard deviation in the tables. MS Office Excel 2007 and Graph Pad Prism version 5.01 (San Diego; CA: Graph Pad Software Inc 2007) were used for statistical analysis and graphical representation. “P < 0.05” was considered as significant. The Spearman correlation coefficient assessed the correlation between BCTQ and NCS parameters. Subsequently, the correlation between the changes in BCTQ and changes in NCS parameters (calculated as the difference between the basal values and those at 9 months post-operative follow-up values) was assessed with the Pearson correlation coefficient.
We have used the Friedman one-way repeated measure analysis of variance test to assess the statistically significant improvement in BCTQ and NCS parameters in three exposures – pre-operative, 6- and 9-months post-CTR in all the three groups. Further, we have used Dunn’s multiple comparison tests to compare the statistically significant improvement in the three exposures: pre-operative versus 6 months post-operative, pre-operative versus 9 months post-operative and 6 months post-operative versus 9 months post-operative.
RESULTS
In our study, all the patients were female and aged between 45 and 55 years, having a mean weight of 55.14 ± 5.76 kg and a mean height of 150.7 ± 1.52 cm.
Table 1 shows statistically significant (P < 0.001) improvement in SSS and FSS of BCTQ in all three groups of patients after 6 and 9 months of follow-up.
| Groups | BCTQ Parameters | |||||
|---|---|---|---|---|---|---|
| SSS (Mean±SD) | FSS (Mean±SD) | |||||
| Pre-operative SSS0 | Post-operative 6 months SSS6 | Post-operative 9 months SSS9 | Pre-operative FSS0 | Post-operative 6 months FSS6 | Post-operative 9 months FSS9 | |
| Gr. I (n=9) | 2.83±0.08 | 1.4±0.10 | 1.23±0.05 | 2.78±0.06 | 1.55±0.05 | 1.21±0.06 |
| Gr. II (n=14) | 3.54±0.25 | 1.83±0.09 | 1.58±0.05 | 3.08±0.11 | 1.75±0.10 | 1.57±0.09 |
| Gr. III (n=16) | 4.45±0.17 | 2.29±0.09 | 1.89±0.19 | 3.61±0.22 | 1.88±0.15 | 1.78±0.09 |
n=number of hands, Gr I: Moderate CTS, Gr II: Severe CTS and Gr III: Extreme CTS. SD: Standard deviation, SSS: Symptom severity scale, FSS: Functional status scale, CTS: Carpal tunnel syndrome, BCTQ: Boston carpal tunnel questionnaire.
In all three groups, there is a statistically significant improvement of the conventional NCS parameter DML as well as short-segment technique TMCV in a 6-month follow-up period, which consistently improved in the 9-month follow-up period (P < 0.001) when compared to preoperatively as evident from the Table 2. In all 16 hands of extreme CTS patients of Group III, both FMCV and TMCV were non-recordable before the operation. FMCV became recordable in eight hands after 6-month follow-up, but TMCV became recordable in all 16 hands. Hence, in extreme CTS patients (Group III), we failed to show statistically significant improvement in FMCV, but in Group I and Group II patients, FMCV showed significant improvement in comparison to pre-operative values.
| NCS Parameter | Groups | Pre-operative (Mean±SD) | Post-operative 6 months (Mean±SD) |
Post-operative 9 months (Mean±SD) |
|---|---|---|---|---|
| DML (ms) | Gr. I (n=9) | 4.74±0.10 | 3.59±0.05 | 3.41±0.12 |
| Gr. II (n=14) | 7.41±2.05 | 4.91±0.47 | 4.13±0.48 | |
| Gr. III (n=16) | NR | 5.44±0.76 | 4.62±0.62 | |
| FMCV (m/s) | Gr. I (n=9) | 55.53±0.76 | 58.24±0.67 | 58.73±0.59 |
| Gr. II (n=14) | 46.41±5.45 | 54.53±1.34 | 55.84±1.54 | |
| Gr. III (n=16) | NR | 18.51±19.14 | 21.73±22.50 | |
| TMCV (m/s) | Gr. I (n=9) | 28.55±0.79 | 35.82±0.71 | 37.36±1.61 |
| Gr. II (n=14) | 12.15±2.51 | 17.89±0.68 | 19.25±1.08 | |
| Gr. III (n=16) | NR | 16.03±0.97 | 18.39±1.41 |
SD: Standard deviation, CTS: Carpal tunnel syndrome, NCS: Nerve conduction study, DML: Distal motor latency, FMCV: Forearm conduction velocity, TMCV: Transcarpal motor conduction velocity, NR: Non-recordable, n: Number of hands, Gr II: Severe CTS and Gr III: Extreme CTS
Table 3 shows the Spearman correlation between BCTQ parameters (SSS and FSS) and NCS parameters (DML, FMCV and TMCV) in all three groups of patients preoperatively and 6 and 9 months after the operation. Spearman correlation coefficients preoperatively were statistically significant in most of the cases but after CTR, it became non-significant.
| Motor NCS | BCTQ parameters | ||||||
|---|---|---|---|---|---|---|---|
| Group | SSS | FSS | |||||
| Pre-operative SSS0 (r) | Post-Operative 6 months SSS6 (r) |
Post-operative 9 months SSS9 (r) |
Pre-operative FSS0 (r) | Post-operative 6 months FSS6 (r) |
Post-operative 9 months FSS9 (r) |
||
| DML | Gr. I (n=9) | 0.967** | 0.143 | 0.116 | 0.753* | 0.294 | 0.041 |
| Gr. II (n=14) | 0.638* | 0.374 | 0.197 | 0.359 | 0.314 | 0.170 | |
| Gr. III (n=16) | — | 0.365 | 0.314 | — | 0.409 | 0.309 | |
| FMCV | Gr. I (n=9) | −0.883** | −0.267 | −0.166 | −0.636 | −0.166 | −0.108 |
| Gr. II (n=14) | −0.620* | −0.388 | −0.322 | −0.361 | −0.293 | −0.207 | |
| Gr. III (n=16) | — | −0.202 | −0.035 | — | −0.212 | −0.048 | |
| TMCV | Gr. I (n=9) | −0.916** | −0.543 | −0.400 | −0.661 | −0.366 | −0.167 |
| Gr. II (n=14) | −0.605* | −0.473 | −0.143 | −0.501 | −0.262 | −0.148 | |
| Gr. III (n=16) | — | −0.121 | −0.092 | — | −0.426 | −0.272 | |
Table 4 shows the Pearson correlation coefficient between the changes in BCTQ and changes in NCS parameters (calculated as the difference between the basal values and those at 9 months post-operative follow-up values), which is statistically non-significant in all three groups of patients.
| Motor NCS Parameters | Groups | BCTQ parameters | |
|---|---|---|---|
| SSS9-0(r) | FSS9-0(r) | ||
| DML9-0 | Gr. I (n=9) | 0.184 | 0.003 |
| Gr. II (n=14) | 0.452 | 0.165 | |
| Gr. III (n=16) | 0.221 | 0.001 | |
| FMCV9-0 | Gr. I (n=9) | −0.407 | −0.157 |
| Gr. II (n=14) | −0.359 | −0.156 | |
| Gr. III (n=16) | −0.468 | 0.386 | |
| TMCV9-0 | Gr. I (n=9) | −0.370 | −0.160 |
| Gr. II (n=14) | −0.403 | −0.090 | |
| Gr. III (n=16) | −0.110 | −0.213 | |
The subscript 9–0 in all the parameters denotes the change between pre-operative and 9-month post-operative follow-up value, r: Pearson correlation coefficient, n: Number of hands, NCS: Nerve conduction study, BCTQ: Boston carpal tunnel questionnaire, Gr II: Severe CTS and Gr III: Extreme CTS
Figures 5-7 show the correlation between BCTQ parameters (SSS and FSS) and TMCV preoperatively and 6 and 9 months after CTR in all three groups of patients.
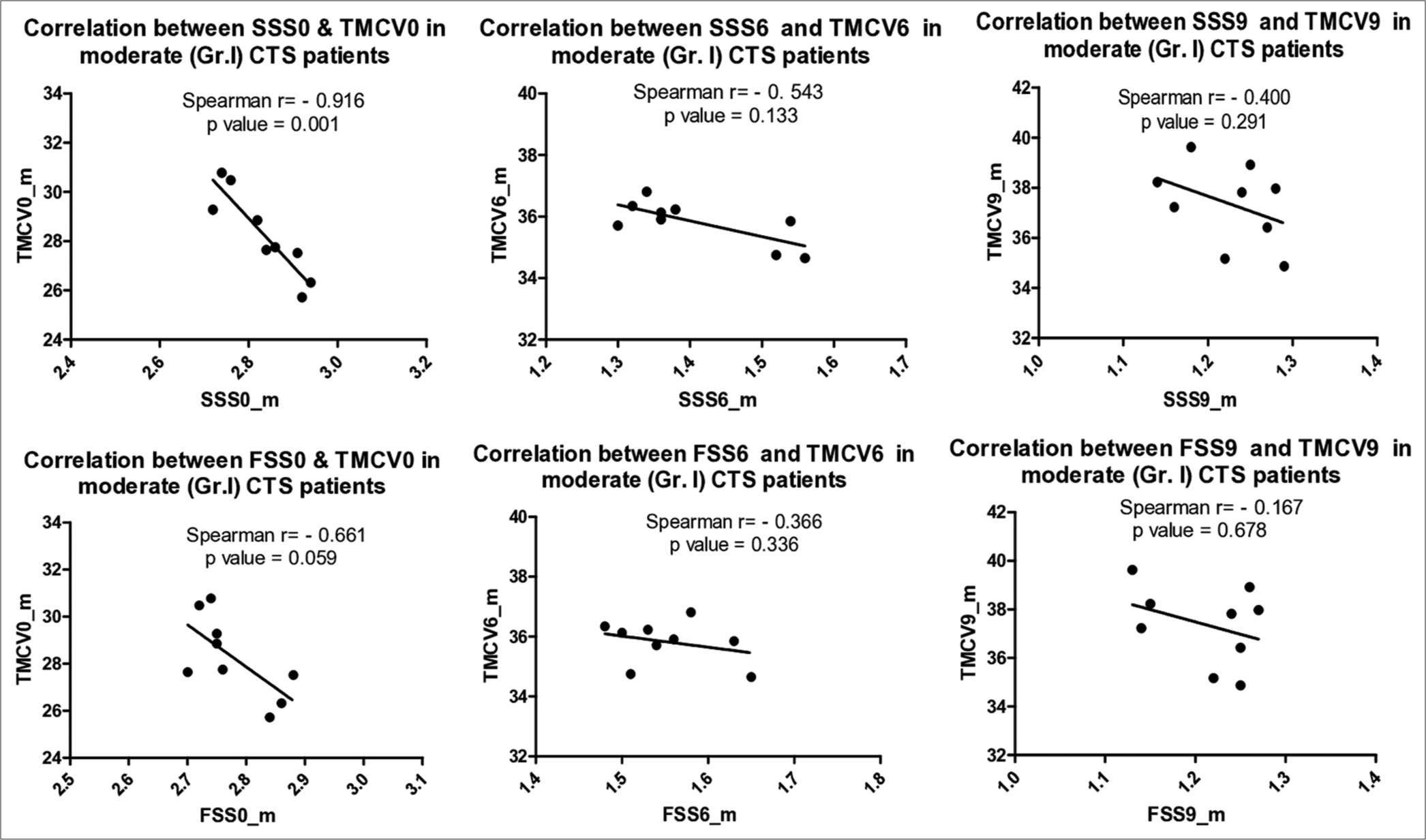
- Correlation between BCTQ (SSS and FSS) and TMCV preoperative and 6 and 9 months postoperative in moderate (Group I) CTS patients. BCTQ: Boston carpal tunnel questionnaire, SSS: Symptom severity scale, FSS: Functional status scale, TMCV: Transcarpal motor conduction velocity, CTS: Carpal tunnel syndrome.
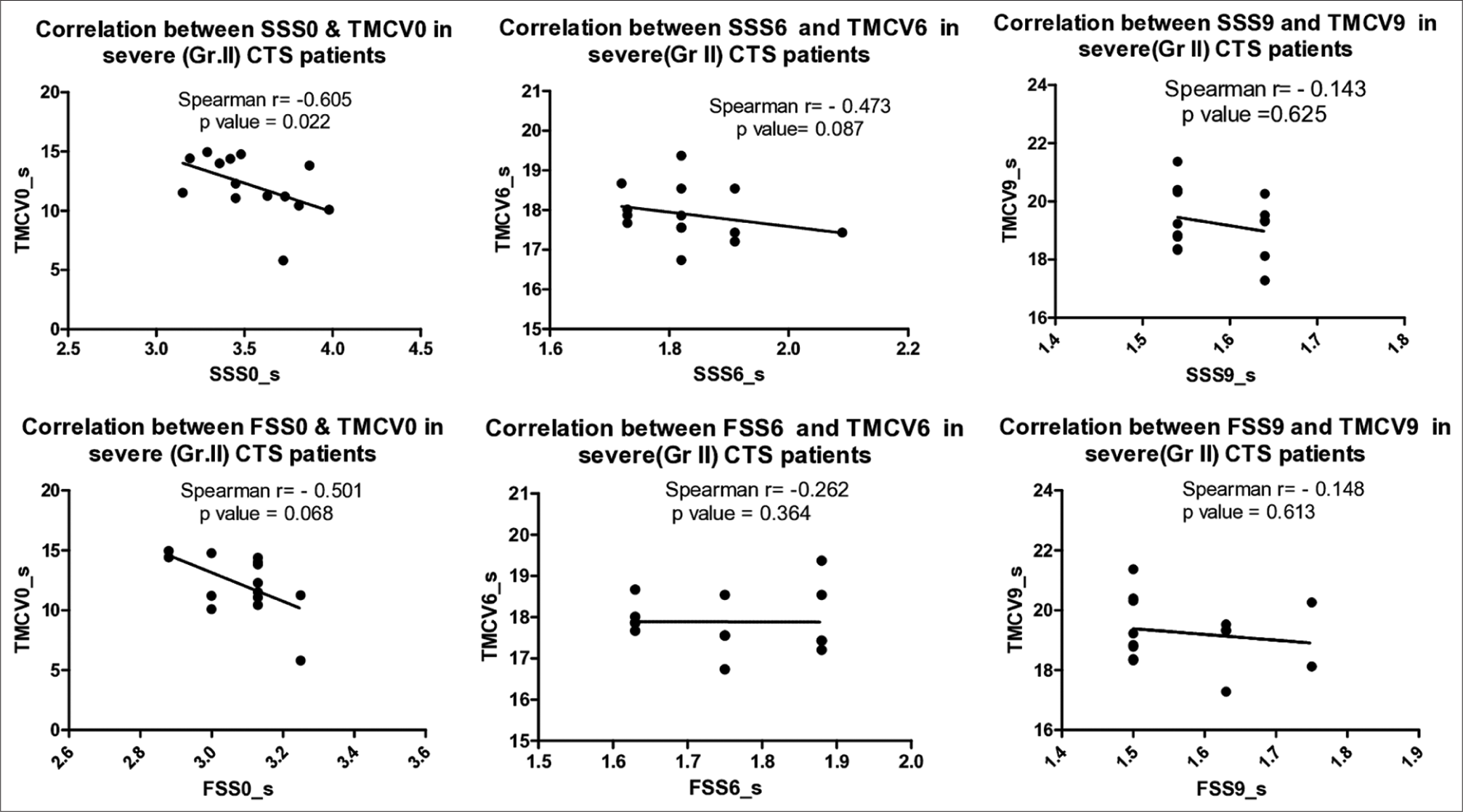
- Correlation between BCTQ (SSS and FSS) and TMCV preoperative and 6 and 9 months postoperative in severe (Group II) CTS patients. BCTQ: Boston carpal tunnel questionnaire, SSS: Symptom severity scale, FSS: Functional status scale, TMCV: Transcarpal motor conduction velocity, CTS: Carpal tunnel syndrome.
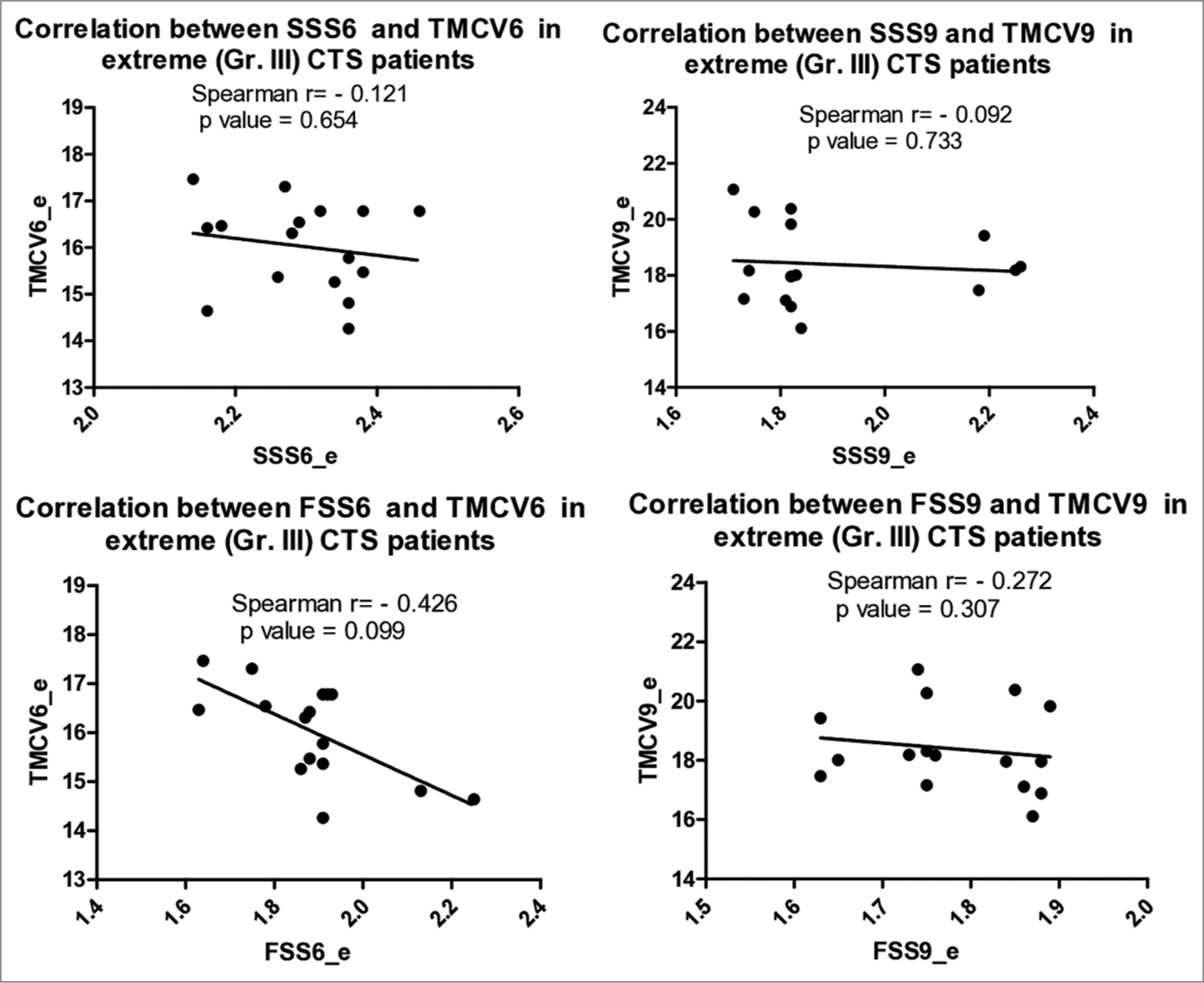
- Correlation between BCTQ (SSS and FSS) and TMCV 6 and 9 months postoperative in extreme (Group III) CTS patients. TMCV was non recordable preoperatively in this group so the correlation could not be calculated. BCTQ: Boston carpal tunnel questionnaire, SSS: Symptom severity scale, FSS: Functional status scale, TMCV: Transcarpal motor conduction velocity, CTS: Carpal tunnel syndrome.
DISCUSSION
In the present study, we have shown statistically significant improvement of Boston carpal tunnel questionnaire parameters – SSS and FSS and also motor NCS parameters – DML, FMCV and TMCV in all the three groups of patients (Group I n = 9 hands, Group II n = 14 hands and Group III n = 16 hands) after CTR operation which is well documented in previous studies.[3-5,15-22]
Although there was a significant correlation between BCTQ parameters – SSS and FSS and motor NCS parameters – DML, FMCV and TMCV in all three groups of CTS patients preoperatively, we found that the Spearman correlation coefficient value decreased and became statistically non-significant after 6 and 9 months of CTR operation. This leads us to the conclusion that in the pre-operative period, clinical outcome and NCS motor parameters were proportional; however, after CTR, there was more improvement in clinical parameters than motor NCS parameters. Several studies documented significant improvement in BCTQ and NCS parameters, but no correlation was found between clinical outcome and NCS.[5-9,23-29] In India, a study showed a significant correlation between BCTQ parameters and motor and sensory parameters in CTS patients[30] which corroborates with our pre-operative findings but no study has been conducted comparing pre- and post-operative cases. Our study was attempted to find the correlation between symptomatic improvement and electrophysiological parameters before and after CTR.
Dhong et al.[23] found SSS correlated with motor latency (Pearson’s correlation coefficient 0.35; P = 0.004) than with sensory latency (Pearson’s correlation coefficient 0.25; P = 0.05). Although Rotman et al.[3] found a significant correlation between DML before CTR and 1 h after operation; no significant correlation was recorded between clinical outcome and 3 and 6-month post-surgical DML. Schrijver et al.[7] found a modest correlation between two clinical symptoms (night awakening and night paresthesia) and median–unnar latency differences and not between the
BQ scores and absolute sensory latency or motor conduction measures. Similarly, Green et al.[4] observed no significant correlation between SSS and median conduction measures and a weak correlation between FSS and median sensory conduction preoperatively, but following surgery, both SSS and FSS showed no significant correlation with conventional NCS. BCTQ and NCS measure different aspects of outcome after CTR operation. Self-administered questionnaires are more susceptible to confounding by subjective information by the patients, whereas NCS demonstrates objective evidence of median nerve function.[7] Therefore, patient satisfaction after a successful operation plays a key role in the BCTQ score; hence, the correlation between BCTQ parameters and NCS motor parameters becomes non-significant after CTR. In our study, there was no significant correlation between the difference of the baseline value from 9 months post-operative of BCTQ parameters with that of NCS motor parameters in all three groups, which are also supported by Mondelli et al.[5] and Schrijver et al.[7]
In spite of the fact that there is no correlation between BCTQ and NCS, pre-operative NCS is necessary to confirm the diagnosis, evaluate the severity, predict the prognosis, determine pathophysiology (axonal loss versus demyelination) and also to exclude other pathologies like cervical radiculopathy, brachial plexopathy, spondylotic myelopathy or polyneuropathy.[7,11,31]
Pre-operative NCS provides a baseline value to differentiate between the recurrence of nerve compression and inadequate release of transverse ligament after CTR.[7,31] In patients who have undergone CTR but symptoms have not been resolved, post-operative NCS provides the only way to determine the cause of failure, which can be due to the presence of other pathology or surgical complications such as neuroma formation, pisohamate pain, hypertrophic scar, pillar pain, scar tenderness, infection, reflex sympathetic dystrophy, lesions of palmer and motor branch.[5-7,31]
Limitations
In India, mild and moderate groups of patients are vehemently unwilling to go through the CTR procedure. Furthermore, the sensory parameters DSL and SNCV of 8 hands out of 14 severe and all the16 hands of extreme CTS patients were non-recordable in both pre-and post-CTR, so we cannot use sensory NCS parameters to establish a correlation between BCTQ and DSL or SNCV. In Group III, extreme CTS patients, FMCV was recordable in eight out of 16 hands at 6 months follow-up, which consistently and continuously improved at 9-month follow-up. Our study continued to 9 months post-operation, but FMCV remains non-recordable in the rest of the extreme CTS patients and, therefore, to demonstrate the return of FMCV in all patients, long-term follow-up is required.
CONCLUSION
Relief of symptoms, improvement of function scale and patient satisfaction are important determinants of the success of CTR operation. It may appear that NCS is not essential in assessing the outcome after the operation, but it cannot be completely abandoned as an unneeded luxury because it provides additional information about the different aspects of the median nerve. Hence, clinicians should use BCTQ and NCS in combination to evaluate the status of the median nerve after a CTR operation.
Acknowledgments
The authors are grateful to the study subjects who gave consent for the research work.
Ethical approval
The study was approved by the Institutional Review Board at Institute of Post Graduate Medical Education and Research, Kolkata, vide Memo No. Inst/IEC/80 dated 5th February 2013.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- The first description of carpal tunnel syndrome. J Hand Surg Eur Vol. 2007;32:195-7.
- [CrossRef] [Google Scholar]
- Time course and predictors of median nerve conduction after carpal tunnel release. J Hand Surg. 2004;29:367-72.
- [CrossRef] [Google Scholar]
- The relationship of pre-and postoperative median and ulnar nerve conduction measures to a self-administered questionnaire in carpal tunnel syndrome. Neurophysiol Clin. 2012;42:231-9.
- [CrossRef] [Google Scholar]
- Relationship between the self-administered Boston Questionnaire and electrophysiological findings in follow-up of surgically treated carpal tunnel syndrome. J Hand Surg Br. 2000;25:128-34.
- [CrossRef] [Google Scholar]
- Assessment of outcome of carpal tunnel syndrome: A comparison of electrophysiological findings and a self-administered Boston questionnaire. J Hand Surg Br. 2002;27:259-64.
- [CrossRef] [Google Scholar]
- Correlating nerve conduction studies and clinical outcome measures on carpal tunnel syndrome: Lessons from a randomized controlled trial. J Clin Neurophysiol. 2005;22:216-21.
- [Google Scholar]
- Do nerve conduction studies predict the outcome of carpal tunnel decompression? Muscle Nerve. 2001;24:935-40.
- [CrossRef] [Google Scholar]
- Protocol of outcome evaluation for surgical release of carpal tunnel syndrome. Neurosurgery. 2003;53:343-50.
- [CrossRef] [Google Scholar]
- A self-administered questionnaire for the assessment of severity of symptoms and functional status in carpal tunnel syndrome. J Bone Joint Surg Am. 1993;75A:1585-92.
- [CrossRef] [Google Scholar]
- Neuroelectrophysiological evaluation of carpal tunnel syndrome before and after surgical intervention. Indian J Rheumatol. 2023;18:199-204.
- [CrossRef] [Google Scholar]
- Comparison of motor conduction technique in the diagnosis of carpal tunnel syndrome. Neurology. 2002;58:1603-7.
- [CrossRef] [Google Scholar]
- Comparison of sensitivity of transcarpal median motor conduction velocity and conventional conduction technique in electrodiagnosis of carpal tunnel syndrome. Clin Neurophysiol. 2006;117:984-91.
- [CrossRef] [Google Scholar]
- Transcarpal motor conduction velocity in carpal tunnel syndrome. Muscle Nerve. 2001;24:966-8.
- [CrossRef] [Google Scholar]
- Median nerve function in patients undergoing carpal tunnel release pre-and post-operative nerve conductions. Electromyogr Clin Neurophysiol. 2003;43:393-7.
- [Google Scholar]
- Evolution of clinical, electrophysiological, and radiological aspects of the carpal tunnel syndrome before and after surgery. Acta Neurol Belg. 2017;117:903-8.
- [CrossRef] [Google Scholar]
- The benefit of carpal tunnel release in patients with electrophysiologically moderate and severe disease. J Hand Surg Am. 2015;40:438-44.e1.
- [CrossRef] [Google Scholar]
- Electrodiagnostic grade and carpal tunnel release outcomes: A prospective analysis. J Hand Surg Am. 2018;43:425-31.
- [CrossRef] [Google Scholar]
- Changes in electrophysiological parameters after surgery for the carpal tunnel syndrome. J Clin Neurophysiol. 2010;27:224-6.
- [CrossRef] [Google Scholar]
- Changes in electrophysiological parameters after open carpal tunnel release. Adv Biomed Res. 2012;1:46.
- [CrossRef] [Google Scholar]
- Delayed electrophysiological recovery after carpal tunnel release for advanced carpal tunnel syndrome: A two-year follow-up study. J Clin Neurophysiol. 2013;30:95-7.
- [CrossRef] [Google Scholar]
- Comparing the outcome of a carpal tunnel decompression at 2 weeks and 6 months. J Hand Surg Br. 2007;32:1154-8.
- [CrossRef] [Google Scholar]
- Correlation of electrodiagnostic findings with subjective symptoms in carpal tunnel syndrome. Ann Plast Surg. 2000;45:127-31.
- [CrossRef] [Google Scholar]
- Carpal tunnel syndrome: The correlation between outcome, symptoms and nerve conduction study findings. J Hand Surg Br. 2001;26:475-80.
- [CrossRef] [Google Scholar]
- Clinical and neurophysiological outcome of surgery in extreme carpal tunnel syndrome. Clin Neurophysiol. 2001;112:1237-42.
- [CrossRef] [Google Scholar]
- Relationships between clinical symptom severity scales and nerve conduction measures in carpal tunnel syndrome. Muscle Nerve. 1999;22:497-501.
- [CrossRef] [Google Scholar]
- Electrophysiological responsiveness and quality of life (Quick DASH, CTSI) evaluation of surgical treated carpal tunnel syndrome. J Orthop Sci. 2009;14:17-23.
- [CrossRef] [Google Scholar]
- Sensitivities of sensory nerve conduction study parameters in carpal tunnel syndrome. J Clin Neurophysiol. 2006;23:565-7.
- [CrossRef] [Google Scholar]
- Italian multicentre study of carpal tunnel syndrome. Differences in the clinical and neurophysiological features between male and female patients. J Hand Surg Br. 1999;24:579-82.
- [CrossRef] [Google Scholar]
- Carpal Tunnel syndrome: Analyzing efficacy and utility of clinical tests and various diagnostic modalities. J Neurosci Rural Pract. 2015;6:504-10.
- [CrossRef] [Google Scholar]
- Electrodiagnostic studies in the surgical treatment of Carpal Tunnel syndrome-a systematic review. J Clin Med. 2021;10:2691.
- [CrossRef] [Google Scholar]




