
Translate this page into:
Influence of desynchronized circadian rhythm on working memory, concentration and divided attention on pink collar shift workers of a tertiary care hospital: A comparative cross-sectional study
*Corresponding author: Nirmala Subhash Anand, Department of Physiology, KAHERs Jawaharlal Nehru Medical College, Belgaum, Karnataka, India. nirmala17april@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rao S, Anand NS. Influence of desynchronized circadian rhythm on working memory, concentration and divided attention on pink collar shift workers of a tertiary care hospital: A comparative cross-sectional study. Indian J Physiol Pharmacol 2020;64(4):279-85.
Abstract
Objectives:
The objective of this study was to find the influence of desynchronized circadian rhythm on working memory, concentration, and divided attention among pink collar shift workers of KLE Hospital as offering 24-h emergency health-care services and hospital care for critical patients by working in shifts can lead to circadian misalignment which can further impair alertness and deteriorate the performance, increase the medical errors and can negatively impact shift workers' health and quality of patient care.
Materials and Methods:
Rey–Osterrieth complex figure test (ROCF) was performed to assess working memory by visual-spatial constructional ability and visual memory. Symbol digit modality test (SDMT) was conducted to assess concentration ability by divided attention, visual scanning, tracking, and motor speed. Following which, a recall test was conducted without any prior warning. Statistical analysis was performed by mean ± SD, unpaired t-test and P-value.
Results:
Shift workers’ and controls’ scores expressed as (mean score ± SD), respectively, were in ROCF copy test (33.52 ± 3.45) and (35.04 ± 3.45), in ROCF recall test (19.68 ± 3.71) and (26.6 ± 2.37), and SDMT correct scores were (49.16 ± 2.34) and (58.6 ± 4.11), SDMT error scores were (1.4 ± 2.32) and (1 ± 1.24), while SDMT total score was (50.56 ± 3.32) and (59.6 ± 5.65).
Conclusion:
Results obtained showed that the mean score for copy test in shift workers was comparatively low but not significant, while in recall test, it was significantly lower indicating lower accuracy to perform a task. Furthermore, their working memory was significantly affected. In the SDMT, the mean correct score was lower, the error score was slightly higher and the total score was significantly lower in shift workers, indicating lower accuracy to perform tasks involving concentration and attention, lower concentration and a significantly lesser speed while performing tasks.
Keywords
Concentration
Divided attention
Shift work
Sleep deterioration
Working memory

INTRODUCTION
Circadian rhythm is a biological rhythm having an endogenous free-running period lasting about 24 h, is entrain able and can keep up periodicity over the physiological temperature range despite changing kinetics.[1] Information regarding daytime is relayed through the eyes to the suprachiasmatic nucleus (SCN) of the hypothalamus, the biological clock and through those clocks in the rest of the body like the sleep-wake cycle may be synchronized. The pineal gland on receiving inputs from SCN secretes melatonin that modulates circadian activity.[2,3] Hypothalamus and reticular activating system mediate circadian rhythm at consciousness state.[4] The sleep-wake cycle is necessary to replenish and heal the body for its proper functioning. Health care setup demands nonstandard working hours to ensure continuity of care and managing critically ill patients, making it imperative for shift workers to sacrifice their sleep and sleeping in the normal rising phase of the circadian rhythm, against environmental zeitgebers, promoting wakefulness; difficulty falling asleep for long periods; because of which sleep duration is reduced, sleep interruption becomes frequent, perceived as less restorative sleep, inducing increased sleepiness during the following night shift.[5] The prefrontal, frontal cortex and thalamus are found to show a significant decrease in metabolic energy consumption in sleep-deprived states.[6] Attention and working memory being related to these areas of brain, are vulnerable to sleep deprived states. Studies have shown that night shift work can cause fatigue, which reduces the cognitive and executive performance of workers and doing successive shifts risk increases by about 6% on the second night, 17% by the third night and 36% by the fourth night.[7,8] Fatigue remains the major source of nurses’ errors in administering medication.[9] Studies have also found that the ability to divide attention between multiple tasks is impaired in sleep deprivation,[10] while some others did not show any association between the two states the role of high cognitive engagement and motivation related to simple attention tasks.[11] In our study, we assumed that for a high cognition and attention-demanding job of a health care worker, divided attention should show greater impairment during sleep deprivation and merely increased effort and cognitive resources recruitment might be insufficient to compensate fully. Imaging studies in sleep-deprived have shown reduced alertness, impaired attention, working memory, logical reasoning, and decision making.[12] Desynchronized circadian rhythm also causes significant health problems among them.[13] Working memory, concentration, divided attention and making quick decisions for patient management which are of utmost importance become questionable. Sleep deprivation has been shown to affect working memory and decision making,[14] while others found it to remain stable for higher-order executive functions in even sleep-deprived conditions due to a generation of motivation and interest, leading to a compensatory effort to do good.[15] This could be true as health workers due to indulgence in such a noble profession, where there is an emotional connection with the patients during the continuous act of serving them and a positive motivational drive to treat them as soon as possible. Furthermore, sleep, distress, and fatigue-related disorders of health workers are still underestimated.[16] Health care demands workers to be at an acceptable cognitive level to fulfill the high level of responsibilities and to deal with workplace stressors, including high workload, demanding work hours and making critical judgments.[17] Adolescence and young adulthood are the period of development in which there is high reporting of cognitive and affective disorders such as anxiety and depression[18] and these have been associated with cognitive deficits such as memory, attention and executive performance[19] and have been shown to persist with remissions[20] with poor neuropsychological performance and have been linked to poor outcomes.[21] Hence, there is a need to identify targets for suitable intervention at an early stage as one factor that could potentially be associated with cognitive impairment is sleep and desynchronized circadian rhythm. Theories and hypothesis regarding how disordered sleep patterns and circadian rhythm misalignment can affect neurocognitive abilities are evolving rapidly with a better understanding of the neurobiology of sleep-wake regulation and also the conflicting nature of research-based evidence regarding the subject, possibly due to differences in the extent of sleep deprivation and the cognitive tasks used across studies, and paucity of data in the young adult population in Indian context provides a platform that we should intrigue the topic and study in-depth about it.
MATERIALS AND METHODS
Study design
This was a comparative cross-sectional study.
Participants’ description
The study population of 30 nurses doing shift work at KLEH, Belagavi, and 30 age and gender-matched daytime working controls were selected and enrolled for data collection according to predetermined inclusion-exclusion criteria and the sample size was calculated.
Sociodemographic details [Table 1].
| Age | 19–23 years |
|---|---|
| Sex | Female |
| Hours of actual sleep | Average 4–5 h of daytime sleep in shift workers (nurses) as compared to 7–8 h of nighttime sleep in the controls working in day hours |
| Qualifications | Nurses doing night shift at KLE Hospital and daytime working controls |
| Substance abuse | Nil |
| History of endocrine disorders | Nil |
Sample size estimation
Expected reduction-(mean) = d = 13.4
SD = 40= σ Power = 80%
α error= 0.05; indicates the probability that differences revealed by statistical analysis really do exist.
One-sided Zα = 1.65 and β error = 0.2; statistical procedures result in a judgment of no significant differences when the differences do exist.
Inclusion criteria
Nurses aged between 19 and 23 years, doing hospital duties in shifts and age- and gender-matched daytime working controls, without any hearing difficulty being tested with a tuning fork, without any visual difficulty being tested by Snellen’s and Jaeger’s chart, and not having any muscular disorder were included in the study.
Exclusion criteria
Having H/O diabetes or any other major illness, H/o alcohol consumption or tobacco chewing in any form, and H/O any psychiatric illness or any medication affecting sleep were excluded from the study.
Procedure: The study was cleared by the Institutional Ethics Committee on Human Subjects Research (Ref: MDC/DOME/77). Based on predetermined inclusion-exclusion criteria, the sample population was chosen. All the participants were explained about the nature of the study and a voluntary informed written consent for participation was taken from them before the start of the study. The following tests were conducted:
Rey–Osterrieth complex figure (ROCF) test is a neuropsychological test that was done to assess the working memory of participants by visual-spatial constructional ability and visual memory. Different cognitive abilities such as planning, organizational skills, problem-solving strategies, visual-spatial abilities, attention, working memory, perceptual, motor, and episodic memory functions mediated by the prefrontal cortex were assessed. It was done in 2 parts: a copy trial, followed by a recall trial 3 min later. The complex figure for both copy and recall was evaluated for its drawing accuracy (1 point), correct placement (1 point). Each element was scored from 0 to 2 and the total range of scores range between 0 and 36. The copy score reflects the accuracy of the original picture drawn, while the recall score deals with the memory component. No warning regarding the memory component was given. Scoring was done from a total score of 36 for both copy and recall. Scoring was done from a total score of 36 for both copy and recall. Studies have used Kappa coefficients and Pearson correlations to evaluate reliability, demonstrated reliability to be high (r > 0.90).[22] Cohen’s Kappa coefficients indicated moderate to a high inter-rater agreement for the organizational elements.[23] Being a nonverbal test, ROCF has an advantage over other tests such as verbal digit span test to assess recall and location learning test, where the participant can use their verbal strategies in the learning phase to remember the location of the object. Multiple studies conducted have found a correlation between ROCF test and metabolic rate of the frontal lobe. One such study being conducted by Melrose et al.,[24] and also studies have shown frontal lobe involvement in dysregulated sleep patterns.
Symbol digit modality test (SDMT) was done to assess concentration ability by divided attention, visual scanning, tracking, and motor speed. Each participant was given a sheet having 8 lines with 15 symbols in each line, below which box is provided to write the corresponding number. The coding key was provided at the top of the page. Participants were given instructions to scan the key and write down the number corresponding to each symbol, as rapidly as possible in 90 s. Scoring involves summing the number of correct substitutions (max = 120). This test was conducted between the ROCA copy and recall test. Total scores, correct scores, and error scores were calculated, and the mean value of each was calculated. Validity research shows that SDMT is a good measure of processing speed or efficiency with a reliability coefficient of .80 for the written version and .76 for the oral version in normal adults.[25] Furthermore, multiple studies have used SDMT test to assess the speed of processing or the psychomotor abilities in the chosen age group.[26]
Statistical analysis
Statistical analysis involved quantitative variables summarized through mean and standard methods of deviation (mean ± SD). P-value and t-value were calculated. “P = 0.001” was considered statistically significant.
RESULTS
Test result tables and graphs
ROCF copy test: To assess working memory (check accuracy) [Table 2]
-
SDMT: To assess concentration ability by divided attention, visual scanning, tracking, and motor speed
3. ROCF recall test: to assess working memory by visual-spatial constructional ability and visual memory (to assess cognitive abilities such as planning, organizational skills, problem-solving strategies, attention, and working memory) [Table 6].
| ROCF copy test | Shift workers | Controls | t-value | P-value |
|---|---|---|---|---|
| Score | 33.52±3.45 | 35.04±3.45 | 1.52±0.99 | 0.13 |
P value= 0.13 (statistically non- significant)
| SDMT mean correct score | Shift workers | Daytime controls | t-value | P-value |
|---|---|---|---|---|
| Score | 49.16±2.34 | 58.6±4.11 | 10.93±0.86 | 0.001* |
P value = 0.001 (* statistically significant)
| Symbol digit modality test mean error score | Shift workers | Daytime controls | t-value | P-value |
|---|---|---|---|---|
| Score | 1.4±2.32 | 1±1.24 | 0.83±0.48 | 0.40 |
P value = 0.40 ( statistically non- significant)
| Symbol digit modality test mean total score | Shift workers | Daytime controls | tvalue | pvalue |
|---|---|---|---|---|
| Score | 50.56±3.32 | 59.6±5.65 | 7.55±1.19 | 0.001* |
P value = 0.001 (* statistically significant)
| Rey–Osterrieth complex figure recall test | Shift workers | Daytime controls | tvalue | pvalue |
|---|---|---|---|---|
| Mean score | 19.68±3.71 | 26.6±2.37 | 8.64±0.80 | 0.001* |
P value = 0.001 (* statistically significant)
DISCUSSION
The present study was conducted on pink collar shift workers in the health care setup of KLE Hospital to assess the effects of desynchronized circadian rhythm on working memory, concentration, and divided attention and comparing them with age- and gender-matched daytime working controls. No significant difference was observed in the ROCF copy test among the two groups [Figure 1]; although, shift workers’ mean score was low in comparison to controls. The possible explanation for not significant ROCF copy test results could be the correct fundamental approach adopted by the participants by organizing the stimulus figure into meaningful perceptual units while copying it, that is, starting to copy figure with global external features and then the local internal details in the construction process. Working memory was significantly affected in shift workers which are contrary to the hypothesis; we made that pink collar health workers doing shift work, working memory component might not be affected due to indulgence in such a noble profession where there becomes an emotional connect with the patients during a continuous act of serving and curing them and a positive drive to treat them; as soon as, possible could be a positive drive of motivation for some. It is also contrary to some other studies which found WM performance remains stable for higher-order executive functions in even sleep-deprived condition due to the generation of motivation and interest, leading to a compensatory effort to perform well in those conditions.[15] In the SDMT, shift workers’ mean correct score was lower, the mean error score was slightly higher, and the total score was significantly lower [Figure 2]; indicating that they have lower accuracy, while performing tasks involving concentration and attention have lower concentration, and a significantly lesser speed to performing a task. The results of our study are as per imaging studies in sleep-deprived showing reduced alertness, impaired attention, working memory, logical reasoning, and decision making,[12] and studies showing that sustaining attention, ignoring task-irrelevant information, and doing multi-tasking effectively are also impaired during sleep deprivation.[27] Most authors observed that fatigue related to night shifts can increase the risk of human errors and injuries and can negatively affect the quality of patient care.[28] Results regarding divided attention are in accordance to our assumption that for a high cognition and attention demanding jobs like of a pink collar health care worker, divided attention should show greater impairment during sleep deprivation, merely increased effort and cognitive resources recruitment might be insufficient to compensate, and a majority of studies that have shown that ability to divide attention between multiple tasks is impaired in sleep-deprived conditions.[10] In the ROCF recall test, shift workers score was significantly low [Figure 3]; indicating lower accuracy to perform a task, which is as per studies showing fatigue induced due to accumulation of sleep deprivation remains the major source of nurses’ errors in administering medication.[9]

- Rey–Osterrieth complex figure copy test showing mean scores of shift workers and daytime working controls.
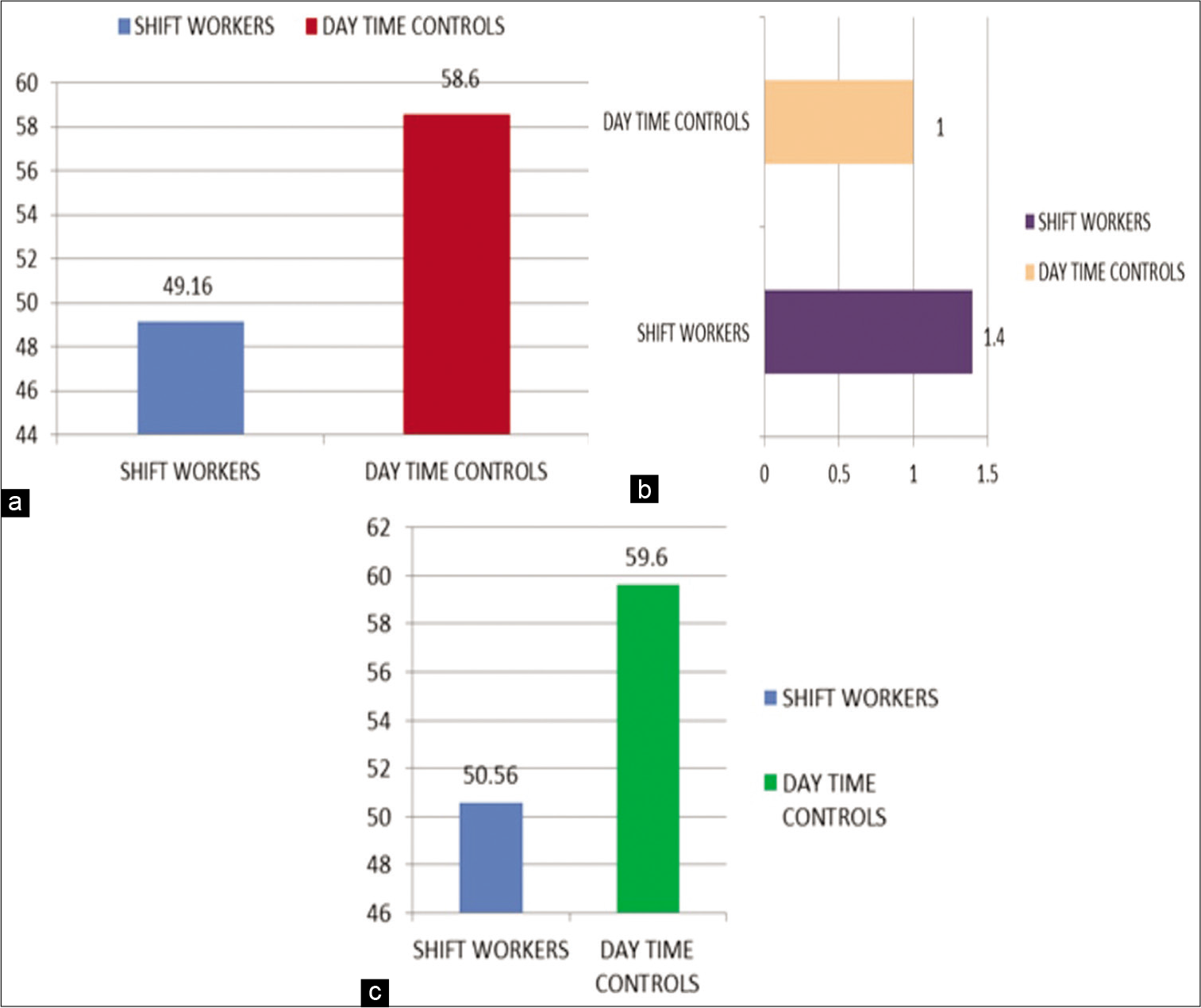
- (a) Symbol digit modality test showing mean of correct scores of shift workers and daytime working controls. (b) Symbol digit modality test showing mean of error scores of shift workers and daytime working controls. (c) Symbol digit modality test showing mean of total scores of shift workers and daytime working controls.
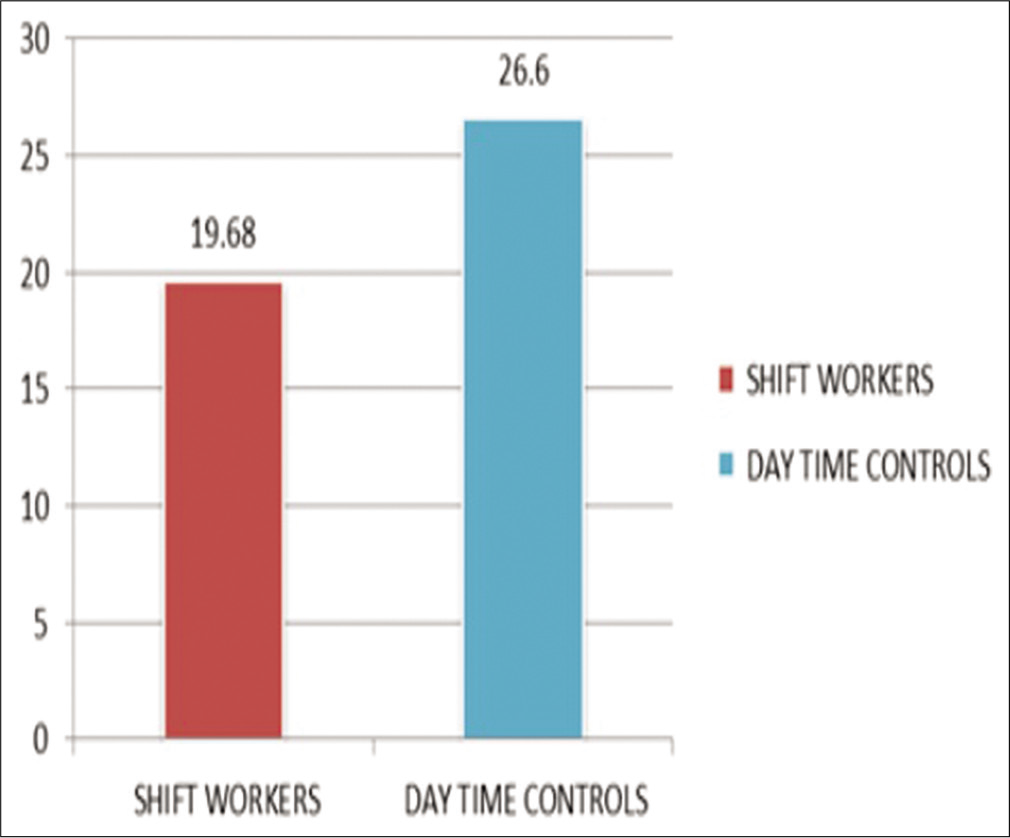
- Rey–Osterrieth complex figure recall test showing mean scores of shift workers and daytime working controls.
CONCLUSION
Caregivers, especially nurses in health setup need to deal with workplace stressors such as high workload, demanding working hours, making critical judgments about fluctuating clinical conditions of the patients, and play a pivotal role in immediate detection and initiating appropriate interventions, with constantly organizing and reorganizing their priorities even at heightened fatigue level, have to make emotional interactions with patients’ and their relatives, and to ensure patients’ safety. To effectively perform these roles, they need to possess psychomotor, affective, cognitive, and complex thinking abilities for planning a suitable course of action. The cognitive status of nurses also has important implications for understanding the origin of medical errors. Shift work done by them to meet health care demands is found to deteriorate their health and even putting patients’ life to risk. Hence, it becomes of utmost importance to take measures regarding the same. It could be done by doing proper health assessment of the employee before shift work, giving suitable rest breaks, insuring regular and predictable schedules, offering at least an 8-h gap between shifts by proper working hours management, and maintaining adequate lighting and temperature control in hospitals, by implementing ergonomics to reduce adverse effects of shift work, so that nurses, other health care workers, and paramedical staff can deliver proper and continuous care to the patients’ without significantly affecting themselves. It can be done by doing proper health assessment of the employee before shift work, giving suitable rest breaks, insuring regular and predictable schedules, offering at least an 8-h gap between shifts by proper working hours management, and maintaining adequate lighting and temperature control in hospitals, by implementing ergonomics to reduce adverse effects of shift work, so that nurses, other healthcare workers, and paramedical staff can deliver proper and continuous care to the patients’ without significantly affecting themselves.
Acknowledgment
This is an STS project taken under Jawaharlal Nehru Medical College, KAHER. I would like to sincerely thank all the participants who volunteered to be a part of this study as well as the technical support staff.
Declaration of patient consent
Institutional Review Board permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Chronobiology: Biological Timekeeping Sunderland, Massachusetts, USA: Sinauer Associates Inc.; 2004. p. :67-105.
- [Google Scholar]
- Synchronizing effects of melatonin on diurnal and circadian rhythms. Gene Comp Endocrinol. 2018;258:215-21.
- [CrossRef] [PubMed] [Google Scholar]
- Wellness with Artificial Light. Available from: https://www.walalight.com/white-paper-released-on-promoting-elder-wellness-with-artificial-light [Last accessed on 2020 Jul 08]
- [Google Scholar]
- Why the SCN influences the whole body: Role of the hypothalamus and reticular activating system. Sleep Biol Rhythms. 2009;7:224-5.
- [CrossRef] [Google Scholar]
- Shift work and disturbed sleep/wakefulness. Occup Med (Lond). 2003;53:89-94.
- [CrossRef] [PubMed] [Google Scholar]
- Neural basis of alertness and cognitive performance impairments during sleepiness II Effects of 48 and 72 h of sleep deprivation on waking human regional brain activity. Thalamus Relat Syst. 2003;2:199-229.
- [CrossRef] [Google Scholar]
- Investigation of the effect of unusual work shifts and sleeps deprivation on cognitive performance in workers in an automotive industry. Iran Occup Health. 2019;16:26-35.
- [Google Scholar]
- Shift work, safety and productivity. Occup Med (Lond). 2003;53:95-101.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of total sleep deprivation on divided attention performance. PLoS One. 2017;12:e0187098.
- [CrossRef] [PubMed] [Google Scholar]
- A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychol Bull. 2010;136:375-89.
- [CrossRef] [PubMed] [Google Scholar]
- Sleep loss and performance: No safe duration of a monotonous task. Physiol Behav. 1998;64:599-604.
- [CrossRef] [Google Scholar]
- The trouble with circadian clock dysfunction: Multiple deleterious effects on the brain and body. Neurosci Biobehav Rev. 2014;40:80-101.
- [CrossRef] [PubMed] [Google Scholar]
- A time to think: Circadian rhythms in human cognition. Cogn Neuropsychol. 2007;24:755-89.
- [CrossRef] [PubMed] [Google Scholar]
- The impact of sleep deprivation on decision making: A review. J Exp Psychol Appl. 2000;6:236-49.
- [CrossRef] [PubMed] [Google Scholar]
- Sleep disorders and work: Guidelines for health surveillance, risk management and prevention. Med Lav. 2013;104:251-66.
- [Google Scholar]
- Physician wellness: A missing quality indicator. Lancet. 2009;374:1714-21.
- [CrossRef] [Google Scholar]
- Lifetime prevalence and ageof-onset distributions of mental disorders in the World Health Organization's world mental health survey initiative. World Psychiatry. 2007;6:168-76.
- [Google Scholar]
- A review on cognitive impairments in depressive and anxiety disorders with a focus on young adults. J Affect Disord. 2008;106:1-27.
- [CrossRef] [PubMed] [Google Scholar]
- Attention and executive functions in remitted major depression patients. J Affect Disord. 2005;89:125-35.
- [CrossRef] [PubMed] [Google Scholar]
- Meta-analysis of the association between cognitive abilities and everyday functioning in bipolar disorder. Bipolar Disord. 2012;14:217-26.
- [CrossRef] [PubMed] [Google Scholar]
- Rey Complex figures Test and Recognition Trial: Professional Manual Odessa: Psychological Assessment Resources; 1995.
- [Google Scholar]
- Interrater reliability: The kappa statistic. Biochem Med (Zagreb). 2012;22:276-82.
- [CrossRef] [Google Scholar]
- Association between cerebral metabolism and rey-osterrieth complex figure test performance in Alzheimer's disease. J Clin Exp Neuropsychol. 2013;35:246-58.
- [CrossRef] [PubMed] [Google Scholar]
- Cognitive performance, sleepiness, and mood in partially sleep deprived adolescents: The need for sleep study. Sleep. 2016;39:687-98.
- [CrossRef] [PubMed] [Google Scholar]
- Unintended consequences of external testing in elementary schools. Educ Meas Issues Pract. 1991;10:7-11.
- [CrossRef] [Google Scholar]
- Sleepiness enhances distraction during a monotonous task. Sleep. 2006;29:573-6.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of rotating night shifts: Literature review. J Adv Nurs. 2005;50:433-9.
- [CrossRef] [PubMed] [Google Scholar]




