
Translate this page into:
Manometric profile of patients presented with dysphagia – A hospital-based descriptive study
 , K. Deepalakshmi1,, S. Mukundan2, P. Thirumal2, R. Vasanthi2, L. Venkatakrishnan2
, K. Deepalakshmi1,, S. Mukundan2, P. Thirumal2, R. Vasanthi2, L. Venkatakrishnan2
*Corresponding author: K. Deepalakshmi, Department of Physiology, PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India. drdeepalakshmik@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Yogisparan PV, Arun P, Vijayabaskaran S, Sairam V, Deepalakshmi K, Mukundan S, et al. Manometric profile of patients presented with dysphagia – A hospital-based descriptive study. Indian J Physiol Pharmacol. 2024;68:135-9. doi: 10.25259/IJPP_9_2024
Abstract
Objectives:
The prevalence of dysphagia is 16–22%. Achalasia is characterised by impaired relaxation of the lower oesophageal sphincter (LES) and absent oesophageal peristalsis. Minimally invasive procedures, endoscopic pneumatic balloon dilatation (PD) and peroral endoscopic myotomy (POEM) are treatments of choice. We aimed to assess the manometric profile of patients presented with dysphagia and pre- and post-LES pressure and integrated relaxation pressure (IRP) of patients who underwent PD and POEM.
Materials and Methods:
One hundred and twenty-nine patients presented with dysphagia underwent high resolution oesophageal manometry (HREM). Manometric parameters: IRP, LES and pattern of motility were noted. According to Chicago classification 4.0, those who are diagnosed with achalasia underwent PD (17) and POEM (15). Statistical analysis was performed using the Statistical Package for the Social Sciences version 28. Pre- and post-procedure values (IRP and basal LES) were compared using the Wilcoxon signed-rank test.
Results:
Out of 129 patients with dysphagia, 57 had increased IRP and 75 had simultaneous motility. The mean LES pressure and IRP were found to be 28 ± 19.82 and 17 ± 14.04 mmHg, respectively. On analysis, of patients who underwent procedures PD (17) and POEM (15), a statistically significant decrease in IRP was observed in patients with post POEM compared to post PD status (P = 0.005 and 0.017, respectively). Reduced basal LES pressure was observed in patients with post-POEM status compared to post-PD status, which was not statistically significant.
Conclusion:
About 44% of patients presented with dysphagia were diagnosed with achalasia cardia. POEM procedure was found to be more effective compared to pneumatic dilatation.
Keywords
Dysphagia
Peroral endoscopic myotomy
Pneumatic dilatation
High-resolution oesophageal manometry

INTRODUCTION
The western hemisphere seems to have done groundbreaking research on dysphagia. However, the east lags behind. In India, studies on dysphagia and its medical and surgical interventions are still said to be in their infancy.[1] The prevalence of dysphagia was reported as 16–22% in individuals above 50 years of age.[2] Another recent population-based study showed that the prevalence of dysphagia was about 17% in the adult population.[3] Aetiology of dysphagia ranges from benign to malignant conditions.[3]
Dysphagia, difficulty in swallowing is the common presentation of the patients suffering from Achalasia Cardia. Achalasia cardia is an oesophageal motor disorder which results from ineffective peristalsis and incomplete or absent lower oesophageal sphincter (LES) relaxation.[4] High-resolution oesophageal manometry (HREM) is the gold standard technique available for diagnosing and staging Achalasia cardia.[5] This technique assesses the upper oesophageal pressures, oesophageal contractility and peristalsis pattern, resting LES pressure and lower oesophageal relaxation. HREM is a rapid and direct method which avoids the use of contrast materials and exposure to radiation.
Treatment options available to reduce LES resting pressure include botulinum toxin injection, oral nitrates, disruption of muscular bundles of LES by laparoscopic myotomy, pneumatic dilation (PD) and peroral endoscopic myotomy (POEM).[6] In pneumatic dilation, a pneumatic balloon is passed through the LES, which disrupts the muscle fibres and reduces the pressure of the LES.[7] POEM is a relatively recent and minimally invasive procedure in which muscles in the lower part of the oesophagus, around the sphincter and in the upper stomach, are resected on endoscopic guidance.[4] In this present study, we aimed to assess the manometric profile of patients who presented with dysphagia in a tertiary care hospital in South India and also compare the outcomes of the interventional procedures POEM and Pneumatic Dilation in achalasia cardia patients.
MATERIALS AND METHODS
This hospital-based descriptive study was conducted in a tertiary care hospital after obtaining the Institutional Ethical Committee clearance. Patients, both males and females, presented with complaints of dysphagia for both solids and liquids belonging to the age group between 18 and 65 years who reported to the gastroenterology department were included in the study. Patients with pregnancy, oesophageal or fundic varices, previous gastric/oesophageal surgery, oesophageal cancer, collagen disease, chronic alcoholics, uncontrolled diabetes, acute and advanced cardiopulmonary disease, systemic sclerosis and uncontrolled thyroid disorders were excluded from the study.
One hundred and twenty-nine patients fulfilled the inclusion and exclusion criteria, which were included in this study after general and systemic clinical examinations of patients were subjected to HREM. The HREM procedure was performed after overnight fasting. The procedure was performed after getting informed consent and explaining the procedure to the patient.
Procedure
A catheter was introduced transnasally till the oesophagogastric junction; with the help of pressure sensors placed throughout the catheter basal LES pressure and motility pattern were recorded. The catheter is guided with lubrication jelly. After locating the oesophagogastric junction, basal pressure LES was recorded for 30 seconds, and the patient was given 10 swallows of 5 mL water each. Findings were analysed using the Chicago Classification 4.0.
Thirty-two patients diagnosed with achalasia cardia underwent interventional procedures such as pneumatic dilation (PD) and peroral endoscopic myotomy (POEM). Out of 32 patients, 17 underwent pneumatic dilation (PD) and 15 underwent (POEM). Integrated relaxation pressure (IRP) and basal LES pressure were assessed post-procedure after a duration of 1 month. The rest of the 97 patients who presented with dysphagia and showed propagative/ineffective/fragmented/premature contractions in manometry were managed medically with proton-pump inhibitors, prokinetics and calcium channel blockers.
Statistical analysis was performed using the Statistical Package for the Social Science version 28. Pre- and post-procedure values (IRP and basal LES) were compared using Wilcoxon signed-rank test.
RESULTS
Descriptive statistics
One hundred and twenty-nine patients with dysphagia between the age group of 18–65 years participated in the study.
Among them, 44% had increased IRP. The average basal LES pressure was 28.81 mmHg (28.81 ± 19.82) and the average IRP was 17.08 mmHg (17.08 mmHg ± 14.04) [Table 1].
| Mean (mmHg)±Std. Deviation | |
|---|---|
| Basal LES Pressure | 28.81±19.82 |
| IRP | 17.0814.04 |
LES: Lower oesophageal pressure, IRP: Integrated relaxation pressure
With respect to motility, out of the total 129 patients, 71% had simultaneous/failed or absent peristalsis, 23% had propagative motility, 5% had ineffective (or fragmented) contractions, and the remaining 1% had premature contractions [Figure 1].
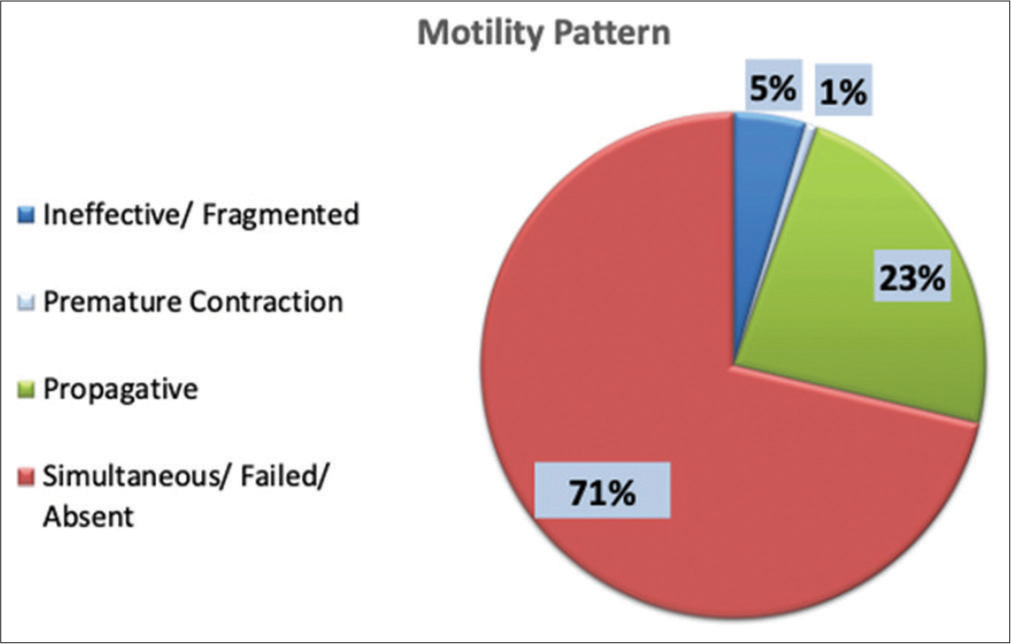
- Motility pattern.
Based on the Chicago classification, out of the 129 patients presented with dysphagia, 70 were found to have achalasia cardia. Of the 70 patients, 75% were managed medically, and 25% underwent procedural intervention [Figure 2].
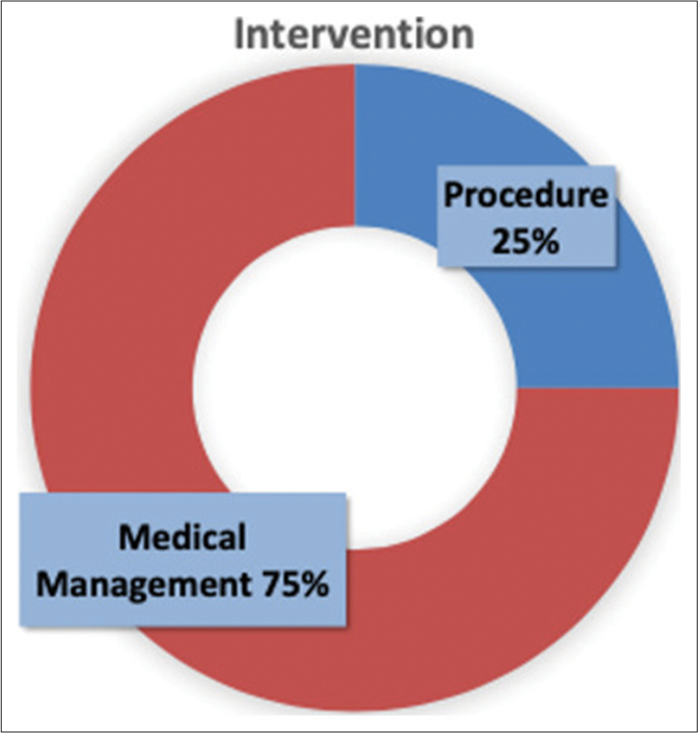
- Intervention type.
Comparative statistics
Out of the 32 patients who underwent intervention, peroral oesophageal endoscopic myotomy (POEM) was performed in 15 patients and pneumatic balloon dilatation (PD) was done in 17 patients [Figure 3]. The efficacy of the intervention was assessed based on the comparison between the pre- and post-procedural values, paired sample test (Wilcoxon signed-rank test) was used for statistical analysis.
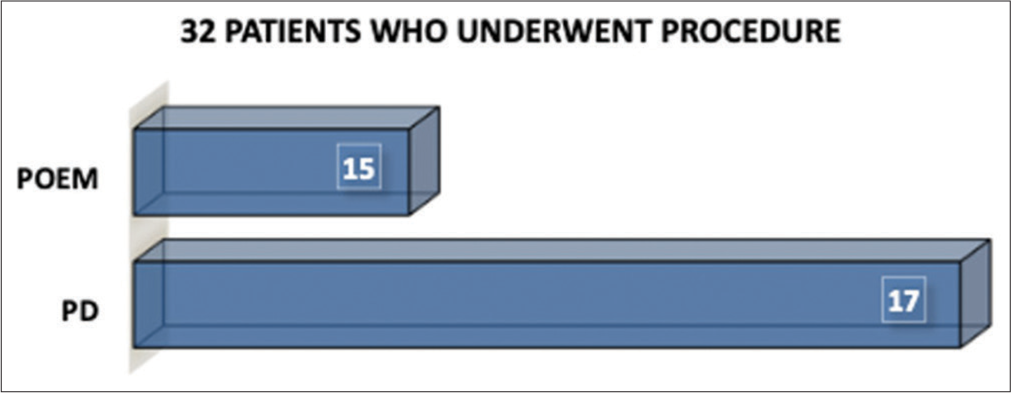
- Descriptive bar diagram of patients who underwent Peroral Esophageal Myotomy and Pneumatic Dilatation Procedures. POEM: Peroral oesophageal myotomy, PD: Pneumatic dilatation.
When the pre (30.51 ± 20.01 mmHg) and post (19.94 ± 11.71 mmHg) resting lower oesophageal pressures of the patients who underwent pneumatic balloon dilatation were compared, no significant difference was found. Similarly, the pre (22.38 ± 14.21 mmHg) and post (13.19 ± 10.76 mmHg) IRP values were compared, and no statistical significance was found.
In the patients who underwent POEM, the pre (33.84 ± 30.14 mmHg) and post (19.72 ± 13.92 mmHg) LES pressures were compared, and there was no statistical significance.
However, the post-IRP value (8.393 ± 7.779 mmHg) was significantly decreased when compared to the pre-IRP value (20.35 ± 11.34 mmHg) [Table 2].
| Motility pattern | Pre/post | Mean (mmHg)±Std. Deviation | Significance |
|---|---|---|---|
| PD: LES | Pre-procedure | 30.511±20.012 | 0.084 |
| Post-procedure | 19.941±11.716 | ||
| PD: IRP | Pre-procedure | 22.382±14.212 | 0.017 |
| Post-procedure | 13.194±10.763 | ||
| POEM: LES | Pre-procedure | 33.840±30.148 | 0.125 |
| Post-procedure | 19.72613.922 | ||
| POEM: IRP | Pre-procedure | 20.353±11.345 | 0.005 |
| Post-procedure | 8.3937.779 |
LES: Lower oesophageal pressure, IRP: Integrated relaxation pressure, PD: Pneumatic dilatation, POEM: Peroral oesophageal myotomy
DISCUSSION
HREM is claimed to be the diagnostic tool for diagnosing common motor disorders of the oesophagus such as achalasia cardia, diffuse oesophageal spasm, nutcracker oesophagus and hypertensive LES.[8] Results of the randomised trial conducted by Roman et al. revealed that oesophageal motility disorders and achalasia were more frequently diagnosed with HREM than with conventional manometry.[9] Misra et al., in their study, elaborated that manometric features of achalasia cardia include absent peristalsis in the body of the oesophagus with incomplete relaxation of the LES.[10] Increased or normal resting LES pressure (LES <30 mmHg) and IRP >15 mmHg is conclusive of achalasia cardia.[11]
In our study, we observed 44% of patients had increased that IRP % and, 36.4% had increased basal LES pressure and 77% had ineffective motility which included simultaneous peristalsis, fragmented and premature contractions. In 2017, Goyal et al., in their study conducted among patients with dysphasia, reported that 43.8% had ineffective oesophageal motility, 26.3% had achalasia cardia, 6.9% had a distal oesophageal spasm and 19.4% had normal manometric findings.[12]
In our study, 32 patients underwent interventional procedures, peroral oesophageal endoscopic myotomy (POEM) was performed in 15 patients and pneumatic balloon dilatation was done in 17 patients. In a study conducted among achalasia cardia patients who underwent pneumatic dilatation, the success rate observed was found to be ranging from 75% to 91% after 6 months and 73–81% after 12 months.[13,14] In patients those who underwent PD, the efficacy wanes with time and complications reported include perforation (2%) and heartburn (15–35%).[15,16] In our study, an achalasia patient who underwent pneumatic balloon dilatation reported to have decreased in resting LES pressure and IRP at the end of 1 month follow-up.
POEM was reported to be a safe and effective treatment option compared to PD and Hellers myotomy, with a success rate of 82–100%.[17,18] In the present study, 15 patients who underwent POEM, the post-IRP values were found to be significantly reduced. In line with our present study, authors reported a significant decrease in the LES pressure and IRP from 33 ± 1.7 and 30 ± 1.4 mmHg to 14 ± 1.2 and 13 ± 1.6 mmHg, respectively, over a period 6 months in study conducted among 2373 patients with achalasia cardia.[19] A study done among 40 achalasia patients who failed to show positive outcomes prior to pneumatic dilation showed favourable results after POEM with an Eckardt score 3 or less.[20] Results of the study conducted among 21 patients also showed similar results.[21] In a follow-up study, both technical (97%) and clinical success (93%) were observed in about 551 achalasia patients who underwent POEM procedure.[22]
We wish to extend our present study with larger sample size, and also, we wish to include the symptomatic profile, Eckardt score and the follow-up of clinical and manometric profiles over a year of the achalasia cardia patients who underwent interventional procedures. Moreover, we wish to conduct multicentric studies in future to determine manometric profiles of normal healthy volunteers to add significance to the normative values held for the Indian population.
CONCLUSION
Our study results showed that 44% of patients presented with dysphagia were diagnosed with achalasia cardia. POEM procedure was found to be more effective when compared to pneumatic dilatation.
Ethical approval
The research/study approved by the Institutional Review Board at PSG Institute of Medical Sciences and Research, number 22/120, dated 01 June 2022.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Dysphagia research in India: A status report. J Indian Speech Lang Hear Assoc. 2018;32:39.
- [CrossRef] [Google Scholar]
- A prospective study evaluating the etiologic spectrum in patients with dysphagia in coastal Odisha using clinical features and endoscopy. J Dig Endosc. 2019;10:107-11.
- [CrossRef] [Google Scholar]
- Clinical profile of patients presenting with dysphagia-an experience from a tertiary care center in North India. JGH Open. 2019;4:472-6.
- [CrossRef] [PubMed] [Google Scholar]
- Peroral endoscopic myotomy (POEM) for achalasia. J Thorac Dis. 2019;11(Suppl 12):S1618-28.
- [CrossRef] [PubMed] [Google Scholar]
- Esophagography in patients with esophageal achalasia diagnosed with high-resolution esophageal manometry. J Neurogastroenterol Motil. 2018;24:403-9.
- [CrossRef] [PubMed] [Google Scholar]
- ACG clinical guideline: Diagnosis and management of achalasia. Am J Gastroenterol. 2013;108:1238-49.
- [CrossRef] [PubMed] [Google Scholar]
- The efficacy of balloon dilation in achalasia is the result of stretching of the lower esophageal sphincter, not muscular disruption. Dis Esophagus. 2016;29:262-6.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical application of esophageal high-resolution manometry in the diagnosis of esophageal motility disorders. J Neurogastroenterol Motil. 2016;22:6-13.
- [CrossRef] [PubMed] [Google Scholar]
- High-resolution manometry improves the diagnosis of esophageal motility disorders in patients with dysphagia: A randomized multicenter study. Am J Gastroenterol. 2016;111:372-80.
- [CrossRef] [PubMed] [Google Scholar]
- Manometric and symptomatic spectrum of motor dysphagia in a tertiary referral center in northern India. Indian J Gastroenterol. 2010;29:18-22.
- [CrossRef] [PubMed] [Google Scholar]
- High-resolution esophageal manometry: Interpretation in clinical practice. Curr Opin Gastroenterol. 2017;33:301-9.
- [CrossRef] [PubMed] [Google Scholar]
- Esophageal motility disorders-symptomatic and manometric spectrum in Punjab, northern India. Indian J Gastroenterol. 2017;36:202-8.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscope-guided pneumatic dilatation of esophageal achalasia without fluoroscopy is another safe and effective treatment option: A report of Taiwan. Surg Laparosc Endosc Percutan Tech. 2008;18:8-12.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of a better outcome of pneumatic dilatation in patients with primary achalasia. J Gastroenterol. 2010;45:153-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pneumatic dilation versus laparoscopic Heller's myotomy for idiopathic achalasia. N Engl J Med. 2011;364:1807-16.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic and surgical treatments for achalasia: A systematic review and meta-analysis. Ann Surg. 2009;249:45-57.
- [CrossRef] [PubMed] [Google Scholar]
- Peroral endoscopic myotomy as a novel treatment for achalasia: Patient selection and perspectives. Clin Exp Gastroenterol. 2020;13:485-95.
- [CrossRef] [PubMed] [Google Scholar]
- Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy. 2010;42:265-71.
- [CrossRef] [PubMed] [Google Scholar]
- Peroral endoscopic myotomy: A meta-analysis. Endoscopy. 2016;48:1059-68.
- [CrossRef] [PubMed] [Google Scholar]
- Peroral endoscopic myotomy (POEM) for esophageal primary motility disorders: Analysis of 100 consecutive patients. J Gastrointest Surg. 2015;19:161-70. discussion 170
- [CrossRef] [PubMed] [Google Scholar]
- Effect of peroral endoscopic myotomy in achalasia patients with failure of prior pneumatic dilation: A prospective case-control study. J Gastroenterol Hepatol. 2014;29:1609-13.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term outcomes of per-oral endoscopic myotomy in achalasia patients with a minimum follow-up of 4 years: A multicenter study. Endosc Int Open. 2020;8:E650-5.
- [CrossRef] [PubMed] [Google Scholar]




