
Translate this page into:
Medication reconciliation to minimise medication errors: Iatrogenic hypercalcaemia as a case report
*Corresponding author: Souvik Majumder, Department of Pharmacology, Medical College Kolkata, Kolkata, West Bengal, India. souvik.majumder@ymail.com
-
Received: ,
Accepted: ,
How to cite this article: Majumder S, Chattaraj S, Roy S, Saha S. Medication reconciliation to minimise medication errors: Iatrogenic hypercalcaemia as a case report. Indian J Physiol Pharmacol. 2024;68:172-5. doi: 10.25259/IJPP_375_2023
Abstract
Hypercalcaemia is a relatively less common yet life-threatening electrolyte disorder and is caused by parathyroid-dependent and independent factors. This case report describes an elderly lady, a known patient of stable hypothyroidism, hypertension, type 2 diabetes mellitus and non-oliguric chronic kidney disease-IV who presented with complaints of gradually worsening drowsiness. Investigations revealed a hypercalcemic crisis; all other contributory investigations were unremarkable. She was put on intravenous saline rehydration, furosemide, pamidronate, and calcitonin. However, due to new-onset haemodynamic instability, cardiomyopathy, and worsening renal parameters, haemodialysis was initiated to reduce the serum calcium levels rapidly. The patient remained asymptomatic after that, and her renal parameters improved to near baseline levels, though cardiac function improvement was not obtained at the end of one month. History elicited from the patient after her neurological improvement revealed that failing to interpret the prescription of three orthopaedics she had visited lately, she followed all simultaneously and had thus consumed toxic levels of calcium and Vitamin D. Medication reconciliatory measures such as e-prescribing, computerised drug dispensing system, automated patient drug dispensing boxes and ‘brown-bagging’ all ongoing medications during the physician visits would ensure reduction in medication errors, thus avoiding adverse events, reducing uncalled for mortalities and morbidities and healthcare cost.
Keywords
Iatrogenic hypercalcemia
Medication reconciliation
Medication error
Drug dispensing

INTRODUCTION
Hypercalcaemia is a relatively less common yet life-threatening electrolyte disorder and is caused by parathyroid-dependent and independent factors. The parathyroid-related causes are typically due to primary or tertiary hyperparathyroidism.[1] Parathyroid-independent causes include calcium overdose, hypervitaminosis D, sarcoidosis and malignancy (through parathyroid hormone-related peptide [PTHrP]), among others.[2]
Symptoms of hypercalcemia, usually observed when serum calcium levels cross 12 mg/dL, include what is classically described as ‘groans, bones, stones, moans and psychic overtones’. Serum calcium is usually maintained within a narrow range from 8.5 to 10.5 mg/dL. Hypercalcemia can be classified into [3]
Mild hypercalcemia: 10.5–11.9 mg/dL
Moderate hypercalcemia: 12.0–13.9 mg/dL
Hypercalcaemic crisis: Above 14 mg/dL.
The general treatment includes adequate hydration and bisphosphonates with/without calcitonin subcutaneously and loop diuretics.[4] Newer options include receptor activators of nuclear factor κ-B ligand monoclonal antibodies like denosumab given at higher doses.[5]
Here, we report a clinical case of an elderly lady who was admitted with hypercalcaemia, revealed to be due to iatrogenic cause on workup, and further stresses the need for medication reconciliation, especially in the elderly, vulnerable population without any proper caregiver.
CASE REPORT
A 74-year-old hypertensive, diabetic, hypothyroid Indian lady, a known patient of non-oliguric chronic kidney disease – Stage IV, presented to the hospital with complaints of gradually worsening drowsiness for about a week. Social history revealed that she is community ambulatory and lives alone, with no proper caregiver and drug adherence/overdosage history could not be elicited then. Initial examination revealed a Glasgow Coma Scale (GCS) of E2V2M4, stable haemodynamic parameters with no significant findings on neurological examination. She was electively intubated for her poor GCS; initial investigations revealed polymorphic leucocytosis (Total leucocytic count of 14,200/cu mm with 84% neutrophilic predominance), calcium levels of 14.3 mg/dL and profound azotaemia (Urea/Creatinine – 266 mg/dL/5.5 mg/dL); other electrolytes were normal and albumin was 4.2 g/dL and procalcitonin on admission was normal. A point-of-care ultrasonogram (POCUS) revealed grossly collapsible inferior vena cava (IVC), denoting severe dehydration with normal cardiac ejection fraction (EF) of 66% and medical renal disease. Other relevant investigations: Blood for serum protein electrophoresis revealed hypoalbuminemia with marginal hyper-gammaglobulinemia and absence of M proteins; urine did not contain Bence Jones protein; blood and urine for microbiological cultures and toxicological screening were negative; serum phosphate and 25(OH) Vit D were normal; PTHrP normal and parathyroid hormone was borderline low normal; chest X-ray and high-resolution computed tomography (CT) scan of thorax was normal, and serum angiotensin-converting enzyme was normal; CT scan of brain and magnetic resonance imaging brain revealed chronic ischaemic changes with mild diffuse cerebral and cerebellar atrophy; no palpable or radiologically visible lymph nodes [Table 1]. Thus, primary hyperparathyroidism, paraneoplastic syndrome, granulomatous disease and multiple myeloma were ruled out. A cerebrospinal fluid study performed in view of the poor sensorium also turned out to be within normal limits.
| Parameter | Day 1 | Day 2 | Day 3 | Day 5 | Day 7 | After 1 month |
|---|---|---|---|---|---|---|
| Hb (gm%) | 11.6 | 10.9 | 10.6 | 11.4 | ||
| TLC (/cu. Mm) | 14200 | 11300 | 8400 | 7300 | ||
| Urea (mg/dl) | 266 | 110 | 118 | 76 | ||
| Creatinine (mg/dl) | 5.5 | 3.7 | 2.1 | 2.0 | ||
| Calcium (mg/dl) | 14.3 | 13.3 | 9.8 | 9.4 | 8.4 | 9.1 |
| Others | TSH- 3.16. Phosphate- 3.3. SPEP- Normal. |
Trop I Positive; CK- 89; CK-MB- 14. | ||||
| Urine- no BJP. PTH-10.09. vit D- 22.6 | ||||||
| Echo-cardiogram | EF 66% | EF 32% | EF 36% |
Hb: Haemoglobin; TLC: Total Leucocytic Count; TSH: Thyroid Stimulating Hormone; SPEP: Serum Protein Electrophoresis; BJP: Bence-Jones Protein; PTH: Parathyroid hormone; EF: Left Ventricular Ejection Fraction; Trop I: Troponin I; CK: Creatine Kinase; CK-MB: Creatine Kinase MB isoenzyme
Vigorous IVC-guided hydration with 0.9% Normal Saline – 150 mL/h was initiated and titrated to achieve euvolemic status, along with judicious use of furosemide 10 mg iv 8th hourly, calcitonin 200 units subcutaneously 12th hourly and pamidronate 90 mg iv once daily. However, on the 2nd day, she developed acute-onset hypotension with a heart rate of 40–45/min, Mobitz II A-V block, for which iv atropine (0.6 mg) was administered, intravenous norepinephrine infusion and urgent haemodialysis (HD) was initiated. However, the HD had to be aborted midway due to worsening hypotension. A repeat POCUS revealed a generalised hypokinetic left ventricle with an EF of 32%. Blood for Troponin I was positive, Creatine Kinase (CK), CK-MB isoenzyme and electrocardiogram were within normal limits. A provisional diagnosis of hypercalcemia-induced cardiomyopathy was concluded.
Post-HD, her calcium levels remained high at 13.3 mg/dL, and a repeat HD was planned on day 3 of hospitalisation while the medical management continued. Post the second HD, a dramatic improvement in calcium levels to 9.8 mg/dL was observed. The patient showed a gradual improvement overall; her improved GCS to E4V5M6 ensured that she was extubated, Ryle’s tube was removed, oral feeding was started, all haemodynamic supports could be stopped, and further, HD was not continued in view of improving renal function with normal urine output and stable calcium levels.
History elicited from the patient after her neurological improvement revealed that she had visited three different orthopaedics in the past year for worsening pain in multiple joints and restricted mobilisation. A review of the three prescriptions yielded that all contained oral calcium formulations, equivalent to 500 mg elemental calcium and Vitamin D3 500 IU 12th hourly, non-opioid analgesics and nutraceuticals. On interviewing, it was known that she was not informed by the orthopaedic to stop her ongoing medications. She had been following all three prescriptions simultaneously, thus amounting to a cumulative daily dose of 3000 mg elemental calcium and 3000 IU Vitamin D. The standard maximum daily dose of calcium for people aged more than 50 years is 2000 mg.[6] Her other daily medications include levothyroxine 75 mcg once daily, prazosin 5 mg and cilnidipine 10 mg once daily, atorvastatin 10 mg once daily, voglibose 0.3 mg twice daily with meals, dapagliflozin 10 mg once daily, linagliptin 5 mg once daily and insulin glargine 10 units subcutaneously once daily at bedtime.
On the 7th day of hospitalisation, when she was planned for discharge, her creatinine had returned to near-baseline levels of 2.1 mg/dL (estimated glomerular filtration rate 24.3 mL/min/1.73 m2), calcium nadir of 8.4 mg/dL and haemodynamically stable and she had remained off HD after the initial 2 episodes. At her routine follow-up after 1 month, she was doing well with creatinine of 2.0 mg/dL, calcium of 9.1 mg/dL, haemodynamically and neurologically fit with normal urine output and no significant abnormalities on systemic examination. Her EF was still 36% with a generalised hypokinetic left ventricle, and further evaluation of coronary arteries for any salvageable cause was planned.
Thus, it can be concluded that lack of medication reconciliation led to life-threatening iatrogenic hypercalcemia in this patient, amounting to a profound financial burden, mental and emotional trauma and an increase in disability-adjusted life years (DALY).
DISCUSSION
With an increasing geriatric population living alone without any proper caregiver, medication reconciliation plays an essential role in ensuring proper delivery of healthcare. Medication reconciliation refers to a process that seeks to assure that the medications which a patient is supposed to take are the same as what they are actually taking. Medication errors like this can cause near misses like this incidence of hypercalcemia if they are controlled in time or may even be fatal if untreated, thus adding to the mortality, morbidity and increase in DALY due to improper medical attention. To reduce errors and harm associated with loss of medical information, as patients transfer among community-based and hospital providers or between them, medication reconciliation is an effective process. The process entails the following steps: [Figure 1].[7,8]
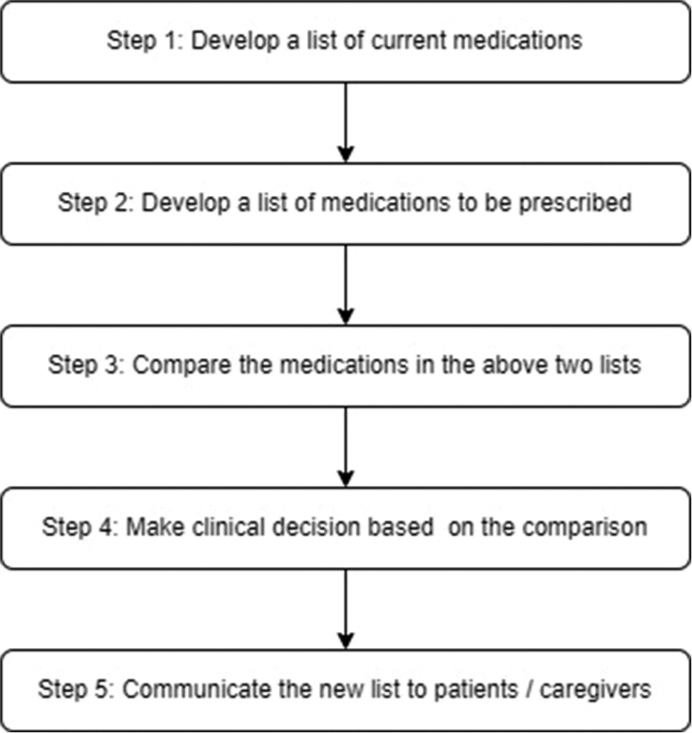
- Steps of medication reconciliation.
Effective approaches to proper implementation of medication reconciliation may include:
The use of a computerised centralised drug dispensing system with an individual user ID (maybe based on some universally valid government-issued ID). The system may be tuned to raise an alarm if medications with the same composition are requisitioned before the scheduled time of refill of the previously purchased medicines.
E-prescribing in generic names (auto-generated) in addition to branded ones. Although this may seem like a huge hurdle, this solution is not a distant possibility nowadays with the increasing adoption of technology in the medical field. Moreover, the government hospitals of many states are now adept at tele-consultations and e-prescribing.
Automated and pre-programmed drug dispensing boxes to dispense medicines to the elderly in a timely manner and
Brown-bagging all ongoing medications during routine physician visits for easier medication reconciliation efforts from the doctor.
This will ensure minimising medication errors, proper dispensing of drugs, and promoting rational prescribing.
Iatrogenic hypercalcemia due to calcium and Vitamin D toxicities is becoming increasingly common with the use of over-the-counter drugs and the increasing geriatric population with their associated age-related comorbidities such as osteoporosis and renal dysfunction.[9] Kato et al. opine that calcium supplementation of more than 2500 mg/day elicits adverse effects on body mineral balance.[10] In view of the multimodal improvement of modern healthcare, this incidence of iatrogenic hypercalcemia warrants its reporting for future references and comparison and may stand out as a learning lesson to implement stricter measures for medication reconciliation.
Limitations
The cardiomyopathy observed was provisionally diagnosed to be due to hypercalcemia in the circumstance of the incident; confirmation to certainty needs further interventional investigations and exclusion of a myriad of factors. Implementing effective medication reconciliatory measures in the context of an increasing geriatric population with increased life expectancy, and hence, comorbidity burden remains a challenge, especially in the setting of a lack of trained caregivers.
CONCLUSION
Increased lifespan also brings with it the unfulfilled gap of geriatric healthcare, thus creating incidences of medication errors and its disastrous effects. Proper implementation of medication reconciliation will ensure minimizing such errors.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Primary hyperparathyroidism: Review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos Int. 2017;28:1-19.
- [CrossRef] [PubMed] [Google Scholar]
- Secondary hyperparathyroidism: Review of the disease and its treatment. Clin Ther. 2004;26:1976-93.
- [CrossRef] [PubMed] [Google Scholar]
- Serum calcium In: Walker HK, Hall WD, Hurst JW, eds. Clinical methods: The history, physical, and laboratory examinations (3rd ed). Boston: Butterworths; 1990. Available from: https://pubmed.ncbi.nlm.nih.gov/21250045/ [Last accessed on 2023 Jul 07]
- [Google Scholar]
- Hypercalcemia of malignancy and new treatment options. Ther Clin Risk Manag. 2015;11:1779-88.
- [CrossRef] [PubMed] [Google Scholar]
- Dietary reference intakes for calcium and vitamin D Washington, DC: The National Academies Press; 2011.
- [Google Scholar]
- Chapter 37: Medication reconciliation In: Advanced pharmacology (2nd ed). New Delhi: PharmaMed Press; 2019. p. :483-9.
- [Google Scholar]
- Iatrogenic hypercalcemia postrenal transplantation. Kidney Int Rep. 2018;4:487-90.
- [CrossRef] [PubMed] [Google Scholar]
- Hypercalcemia induced by excessive intake of calcium supplement, presenting similar findings of primary hyperparathyroidism. Endocr J. 2004;51:557-62.
- [CrossRef] [PubMed] [Google Scholar]




