
Translate this page into:
Normative data of upper limb nerve conduction in North Kerala population
*Corresponding author: S. Ram Kumar, Department of Neurology, Government Medical College, Kozhikode, Kerala, India. sramkumar1611@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ram Kumar S, Jose J. Normative data of upper limb nerve conduction in north Kerala population. Indian J Physiol Pharmacol. 2024;68:223-30. doi: 10.25259/IJPP_474_2023
Abstract
Objectives:
The objective of this study was to detect the normal motor amplitude, distal latency, conduction velocity, sensory amplitude, sensory latency and F-wave latency of upper limb nerves (Median nerve, ulnar nerve and radial nerve).
Materials and Methods:
It was a cross-sectional study conducted in the Department of Neurology, Government Medical College, Kozhikode, between 1 January 2022 and 31 December 2022. Nerve conduction studies (NCSs) were performed prospectively in the upper limbs of 311 carefully screened, healthy individuals of either sex, who were between the ages of 13 and 60 years, belonging to the North Kerala population, using the standardised technique.
Results:
The study population consisted of 54% males and 46% females. The mean age, height, weight and body mass index (BMI) of the study population were 39 ± 15 years, 163 ± 12 cm, 58 ± 11 Kgs and 22 ± 2.7 Kg/m2, respectively. The motor, sensory parameters and F-wave latency of median ulnar and radial nerves were established. We obtained a significant positive correlation between motor distal latency, sensory distal latency and F-wave latency of median and ulnar and radial nerves with age, height and weight. We obtained a significant negative correlation between motor distal amplitude, sensory distal amplitude and conduction velocity of median, ulnar, and radial nerves with age, height and weight. In our study, females had faster conduction velocity, shorter F-wave latency, motor distal latency, sensory latency and higher motor amplitude and sensory amplitude than males. BMI did not have a significant correlation with nerve conduction parameters in our study.
Conclusion:
Normative conduction parameters of commonly tested peripheral nerves of the upper limb were established for our electrophysiology laboratory. While performing NCS, it is essential to adapt values based on physiological factors such as age, gender, height, weight and BMI, which enhance the diagnostic sensitivity of the procedure and, thus, avoid misdiagnosis and mistreatment of various demyelinating and axonal disorders.
Keywords
Upper limb
Electrophysiology
Nerve conduction
Normative data
North Kerala

INTRODUCTION
Nerve conduction studies (NCSs) are a part of electrodiagnostic methods utilised in the clinics for assessing the normal functioning status of the peripheral nerves.[1] Each electrophysiology laboratory must establish standard values specific to its local population to identify individuals with abnormal results. Factors such as age, weight, height, gender and body mass index can influence the motor and sensory parameters of the nerve, and hence, it can affect the study results. With advancing age, conduction velocity decreases. There is a tendency for females to have shorter latency and higher conduction velocity. Slow conduction velocity has been observed in tall individuals. Therefore, while performing NCS, it is essential to adapt values based on physiological factors such as age, gender and height, which enhance the diagnostic sensitivity of the procedure.[2-7] There are not many studies on motor and sensory nerve conduction and the evaluation of various factors affecting the nerve parameters in the North Kerala population. One study was done on the North Kerala population by Ahammed Naseem et al., which studied only motor conduction study and the influence of height on it.[8] Hence, the primary objective of this research was to establish normal electrophysiological measurements for upper limb motor and sensory nerve conduction parameters within the North Kerala population. These measurements would then serve as our institute’s standard reference values in our laboratory.
MATERIALS AND METHODS
It was a cross-sectional study conducted in the Department of Neurology, Government Medical College, Kozhikode, between 1 January 2022 and 31 December 2022. The ethics clearance from the Institutional Ethics Committee (IEC) was obtained before the start of the study (GMCKKD/RP 2021/IEC/273). Healthy bystanders of patients, clinical and non-clinical staff of the institute, belonging to either sex, who were between the ages of 13 and 60 years and belonging to the North Kerala population, were carefully screened. After excluding smokers, alcoholics, volunteers with type 2 diabetes mellitus, systemic hypertension, obesity (≥25 kg/m2), history of any limb injury, history of neuropathy, symptoms of neuropathy, known neuromuscular disorders, myopathy and those on drugs causing neuropathy, consenting participants were subjected to preliminary NCS. Consent was obtained from the parents/guardians of all participants less than 18 years old. Bilateral upper limb fourth digit sensory peak latencies were measured for median and ulnar nerves, and those participants with a difference in the peak latency of ≥0.5 ms between the two nerves of the ipsilateral arm were regarded to have asymptomatic carpal tunnel syndrome and were excluded from further study. Three hundred and eleven participants were eligible, and baseline data were collected, including height, weight and body mass index (BMI), and were subjected to detailed NCS by qualified neurotechnologists using the NICHOLET EMG machine.
Participants were allowed to adapt to the standard room temperature of 27°C ± 2°C for 10 min. Filters were set at 2–5 kHz, and the sweep speed was 5 ms per division for motor study, and for sensory study, filters were at 20–3 kHz, and the sweep speed was 2 ms per division. Duration of stimulus for both motor and sensory study was at 100 ms. A current of supramaximal stimulus was delivered to get adequate responses. Median, ulnar and radial nerves of both upper limbs were tested. Three surface electrodes were utilised for recording purposes: An active electrode, a reference electrode and a ground electrode. The active electrode was positioned over the muscle belly, the reference electrode was placed on a nearby tendon or bone away from the muscle, and the ground electrode was positioned between the stimulator and the active electrode. Proper grounding is crucial to ensure that the obtained response is not distorted by excessive artefacts.
The stimulator employed consisted of two metal pad electrodes placed approximately 1.5–3 cm apart. During stimulation, the cathode (typically identified as black or the negative pole) was oriented toward the direction in which the nerve was to be stimulated. All measurements were conducted with supramaximal stimulation to ensure maximal response. For sensory NCS, an antidromic approach using ring electrodes was employed. F-wave studies entailed supramaximal stimulation of motor nerves, resulting in the generation of a large compound muscle action potential (CMAP) followed by a smaller, irregularly shaped CMAP. A minimum of ten stimuli were administered to obtain the F-wave on a rostered scale, and the minimum F-wave latency (F-min lat.) was recorded. For sensory studies, the radial, median and ulnar nerves were examined antidromically. The active ring electrode was placed over the thumb, middle finger and little finger to record responses along the radial, median and ulnar nerves, respectively. The reference electrode was placed about 4 cm distal to the active electrode. Median nerve stimulation was performed at 13 cm proximal to the active electrode and medial to the flexor carpi radialis tendon. For the ulnar sensory, nerve stimulation was performed 10 cm proximal to the active electrode and posterior to the flexor carpi ulnaris tendon. Radial nerve stimulation was performed 10 cm proximal to the active electrode along the lateral border of the radius. The interelectrode distance between the recording electrodes is 2.5–4 cm. In the motor conduction study of the median nerve, the active electrode was positioned at the centre of the abductor pollicis brevis muscle. The reference electrode was placed on the proximal phalanx of the thumb, approximately 3–4 cm distal to the active electrode. For distal stimulation, impulses were administered 3 cm proximal to the distal wrist crease, situated between the tendons of the flexor carpi radialis and palmaris longus. The proximal stimulation point was located at the elbow, just lateral to the brachial pulsation.
In the motor conduction study of the ulnar nerve, the active electrode was centred on the abductor digiti minimi muscle. The reference electrode was positioned distally over the fifth digit. Distal stimulation was applied 3 cm proximal to the distal wrist crease, slightly medial to the flexor carpi ulnaris tendon. The proximal stimulation point was situated at the elbow, approximately 3–4 cm distal to the medial epicondyle, with both the wrist and elbow flexed at 90°. In the radial nerve motor conduction study, an active electrode was placed on the extensor indicis proprius with hand hand-pronated two-finger breadth proximal to the ulnar styloid. The reference electrode was placed on the ulnar styloid. Distal stimulation was given over the ulnar over 4–6 cm 3 cm proximal to the active recording electrode. The proximal stimulation point was at the elbow in the groove between the biceps and brachioradialis muscle.
For motor nerves, the following parameters were analysed: The distal motor latency, CMAP amplitude and motor nerve conduction velocity. For sensory nerves, distal sensory onset latency and sensory nerve action potential amplitude (SNAP) were recorded.
Data assessment was done using the Statistical Package for the Social Sciences software. MS Word and Excel were used to generate tables and charts. P < 0.05 was taken as significant. The correlation was assessed using the Pearson coefficient(r).
RESULTS
A total of 311 carefully screened healthy participants were studied during the study period. Of the total, 168 (54%) were male and 143 (46%) were female. The baseline characteristics of the study population (n = 311) are given in Table 1.
| Variables | Mean±SD |
|---|---|
| Age (in years) | 39±15 |
| Height (in cm) | 163±12 |
| Weight (in Kg) | 58±11 |
| BMI (Kg/m2) | 22±2.7 |
SD: Standard deviation, BMI: Body mass index
Median nerve motor and sensory parameters
The median nerve motor and sensory parameters of the study population are given below in Figure 1.
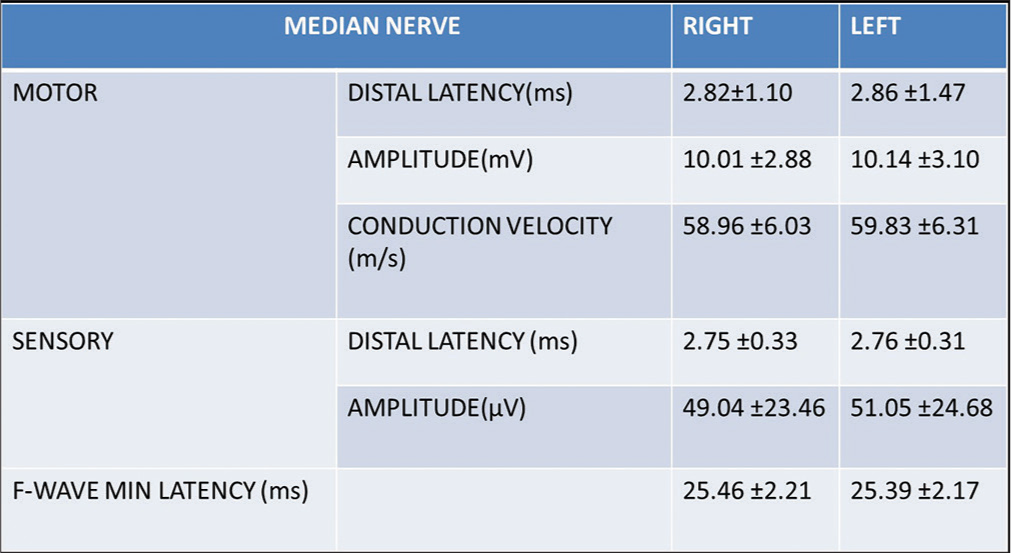
- The motor and sensory parameters of the median nerve of the study population (n = 311) (ms-milliseconds, mV-millivolts, m/s-metres/second and µV-microvolts).
Ulnar nerve motor and sensory parameters
The ulnar nerve motor and sensory parameters of the study population are given below in Figure 2.
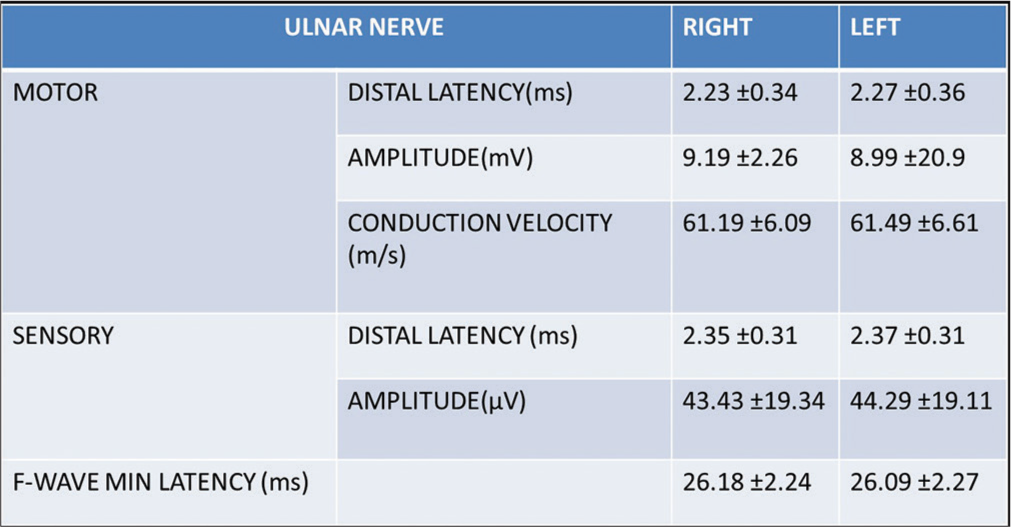
- The motor and sensory parameters of the ulnar nerve of the study population (n = 311). (ms-milliseconds, mV-millivolts, m/s-metres/second and µV-microvolts).
Radial nerve motor and sensory parameters
The radial nerve motor and sensory parameters of the study population are given below in Figure 3.
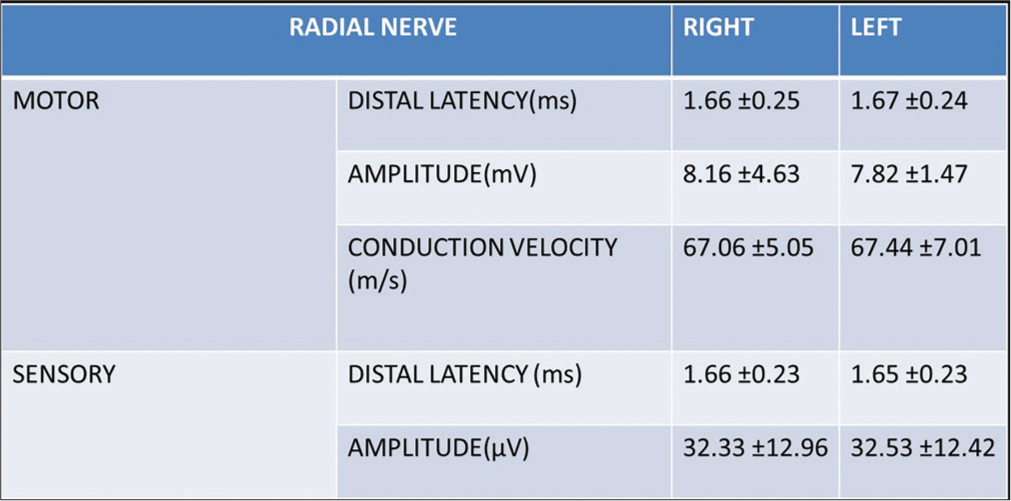
- The motor and sensory parameters of the radial nerve of the study population (n = 311). (ms-milliseconds, mV-millivolts, m/s-metres/second and µV-microvolts).
We analysed the correlation of different nerve parameters with age, sex, height, weight and BMI of the study population.
Correlation of age and different nerve parameters
In our study, we analysed age with different nerve parameters of median, ulnar and radial nerves and we obtained significant positive and negative correlation of various parameters with age.
Age and median nerve
There existed significant positive correlation between age and left median distal latency (r = 0.122, P-0.032, n = 311), right F-wave latency(r = 0.432, P −< 0.001, n = 311), left F-wave latency (r = 0.396, P −< 0.001, n = 311), right sensory latency (r = 0.367, P −< 0.001, n = 311) and left sensory latency (r = 0.324, P −< 0.001, n = 311).
There existed significant negative correlation between age and right distal amplitude (r = −0.285, P −< 0.001, n = 311), left distal amplitude (r = −0.274, P −< 0.001, n = 311), right and left conduction velocity (r = −0.223, P −< 0.001, n = 311), (r = −0.25, P −< 0.001, n = 311), respectively, and right and left sensory amplitude (r = −0.514, P −< 0.001, n = 311), (r = −0.514, P −< 0.001, n = 311), respectively.
Age and ulnar nerve
There existed significant positive correlation between age and right and left ulnar distal latency (r = 0.242, P −< 0.001, n = 311), (r = 0.185, P = −0.001, n = 311) respectively, right F-wave latency (r = 0.401, P −< 0.001, n = 311), left F-wave latency (r = 0.405, P −< 0.001, n = 311), right sensory latency (r = 0.247, P −< 0.001, n = 311) and left sensory latency (r = 237, P −< 0.001, n = 311).
There existed significant negative correlation between age and right distal amplitude (r = −0.197, P −< 0.001, n = 311), left distal amplitude (r = −0.167, P −< 0.001, n = 311), right and left conduction velocity (r = −0.15, P = −0.008, n = 311), (r = −0.153, P= −0.007, n = 311), respectively, and right and left sensory amplitude (r = −0.446, P −< 0.001, n = 311), (r = −0.455, P −< 0.001, n = 311), respectively.
Age and radial nerve
There existed a significant positive correlation between age and right radial distal latency (r = 0.194, P = −0.001, n = 311).
There existed significant negative correlation between age and right and left conduction velocity (r = −0.252, P −< 0.001, n = 311), (r = −0.099, P = −0.082, n = 311), respectively, right and left sensory amplitude (r = −0.185 P = −0.001, n = 311), (r = −0.152, P = −0.007, n = 311), respectively.
Correlation of height with different nerve parameters
In our study, we analysed height with different nerve parameters of median, ulnar and radial nerves and we obtained significant positive and negative correlation of various parameters with height.
Height and median nerve
There existed a significant positive correlation between height and right F-wave latency (r = 0.392, P −< 0.001, n = 311), left F-wave latency (r = 0.406, P −< 0.001, n = 311), right sensory latency (r = 0.270, P −< 0.001, n = 311) and left sensory latency (r = 0.262. P −< 0.001, n = 311).
There existed significant negative correlation between height and right distal amplitude (r = −0.139, P = −0.014, n = 311), left distal amplitude (r = −0.122, P = −0.031, n = 311), right and left conduction velocity (r = −0.209, P −< 0.001, n = 311), (r = −0.248, P −< 0.001, n = 311), respectively, and right and left sensory amplitude (r = −0.306, P −< 0.001, n = 311), (r = −0.296, P −< 0.001, n = 311), respectively.
Height and ulnar nerve
There existed a significant positive correlation between height and right and left ulnar distal latency (r = 0.308, P −< 0.001, n = 311), (r = 0.240, P −< 0.001, n = 311), respectively, right F-wave latency (r = 0.427, P −< 0.001, n = 311), left F-wave latency (r = 0.428, P −< 0.001, n = 311), right sensory latency (r = 0.291, P −< 0.001, n = 311) and left sensory latency (r = 0.293, P −< 0.001, n = 311).
There existed a significant negative correlation between height and right and left conduction velocity (r = −0.227, P −< 0.001, n = 311), (r = −0.252, P −< 0.001, n = 311), respectively, right and left sensory amplitude (r = −0.317, P −< 0.001, n = 311), (r = −0.333, P −< 0.001, n = 311), respectively.
Height and radial nerve
There existed a significant positive correlation between height and right and left radial distal latency (r = 0.194, P = −0.001, n = 311) (r = 0.116, P = −0.042, n = 311), respectively.
There existed significant negative correlation between height and right and left conduction velocity (r = −0.199, P −< 0.001, n = 311), (r = −0.132, P = −0.02, n = 311), respectively, right and left sensory amplitude (r = −0.121, P = −0.034, n = 311), (r = −0.140, P = −0.014, n = 311), respectively.
Correlation of weight with different nerve parameters
In our study, we analysed weight with different nerve parameters of median, ulnar and radial nerves and we obtained significant positive and negative correlation of various parameters with weight.
Weight and median nerve
There existed a significant positive correlation between weight and right F-wave latency (r = 0.368, P −< 0.001, n = 311), left F-wave latency (r = 0.366, P −< 0.001, n = 311), right sensory latency (r = 0.216, P −< 0.001, n = 311) and left sensory latency (r = 0.169, P −< 0.001, n = 311).
There existed significant negative correlation between weight and right and left conduction velocity (r = −0.224, P −< 0.001, n = 311), (r = −0.216, P −< 0.001, n = 311), respectively, right and left sensory amplitude (r = −0.231, P −< 0.001, n = 311), (r = −0.238, P −< 0.001, n = 311), respectively, and right median motor distal amplitude (r = −0.132, P = −0.02, n = 311).
Weight and ulnar nerve
There existed significant positive correlation between weight and right and left ulnar distal latency (r = 0.291, P −< 0.001, n = 311), (r = 0.208, P −< 0.001, n = 311) respectively, right F-wave latency (r = 0.367, P −< 0.001, n = 311) and left F-wave latency (r = 0.365, P −< 0.001, n = 311), right sensory latency (r = 0.243, P −< 0.001, n = 311) and left sensory latency (r = 0.217, P −< 0.001, n = 311).
There existed a significant negative correlation between weight and right and left conduction velocity (r = −0.221, P −< 0.001, n = 311), (r = −0.230, P −< 0.001, n = 311), respectively, right and left sensory amplitude (r = −0.247, P −< 0.001, n = 311), (r = −0.264, P −< 0.001, n = 311) respectively.
Weight and radial nerve
There existed a significant positive correlation between weight and right radial distal latency (r = 0.139, p = −0.014, n = 311).
There existed a significant negative correlation between weight and right and left conduction velocity (r = −0.200, P −< 0.001, n = 311), (r = −0.170, P = −0.003, n = 311), respectively.
Correlation of BMI with different nerve parameters
In our study, we analysed BMI with different nerve parameters of median, ulnar and radial nerves and we obtained significant positive and negative correlation of various parameters with BMI.
BMI and median nerve
There existed a significant positive correlation between BMI and right median F-wave latency (r = 0.115, P = −0.043, n = 311).
BMI and radial nerve
There existed a significant negative correlation between BMI and left radial distal latency (r = −0.125, −0.027, n = 311).
Correlation of gender with different nerve parameters
In our study, we found that females had significantly faster right and left median, ulnar, right radial conduction velocity and higher right and left median, ulnar, radial sensory distal amplitude and lower median sensory, median F-wave latency, right and left ulnar distal latency, ulnar sensory latency and ulnar F-wave latency compared to males, which are illustrated in Figures 4-9 given below.
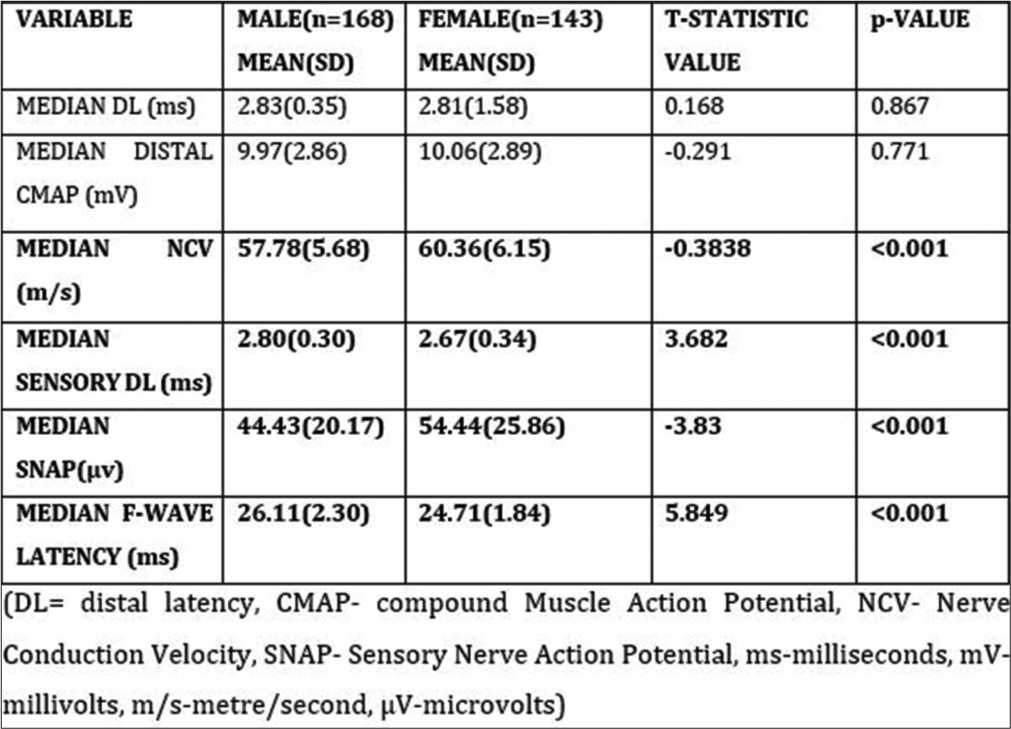
- Correlation of the right median nerve conduction parameters with gender. Parameters (variable) entered in bold values indicates significant p-value.
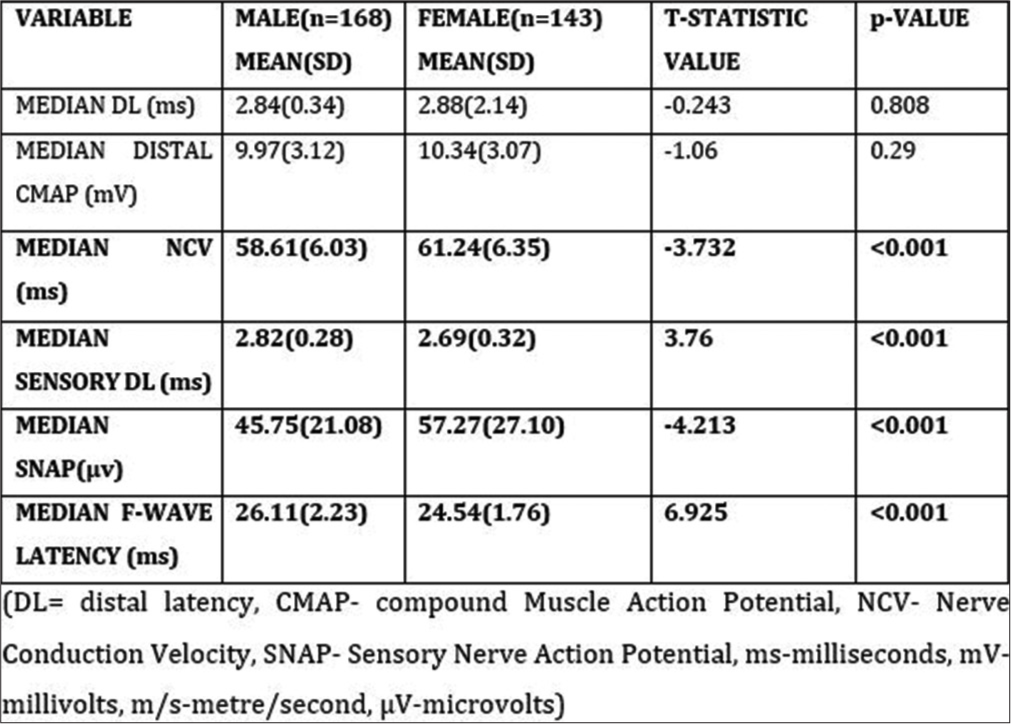
- Correlation of the left median nerve conduction parameters with gender. Parameters (variable) entered in bold values indicates significant p-value.
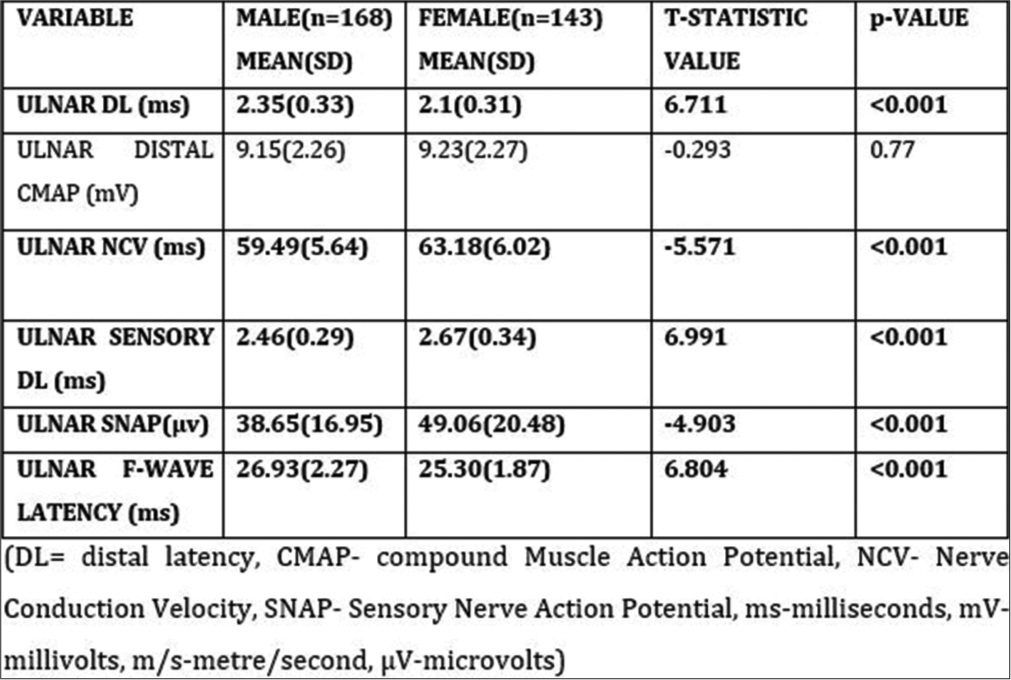
- Correlation of the right ulnar nerve conduction parameters with gender. Parameters (variable) entered in bold values indicates significant p-value.
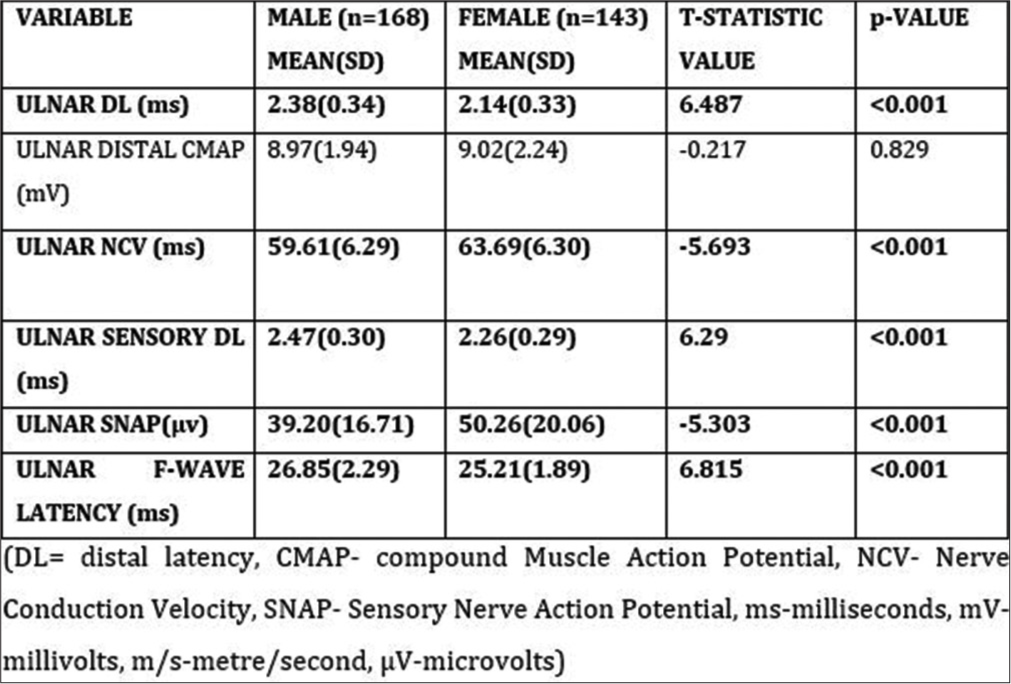
- Correlation of the left ulnar nerve conduction parameters with gender. Parameters (variable) entered in bold values indicates significant p-value.
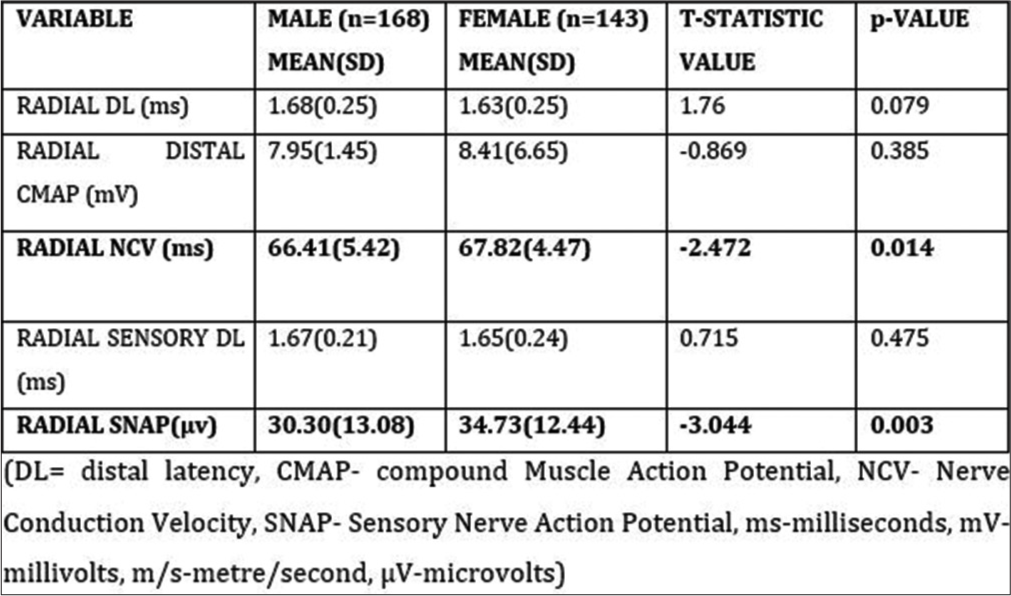
- Correlation of the right radial nerve conduction parameters with gender. Parameters (variable) entered in bold values indicates significant p-value.
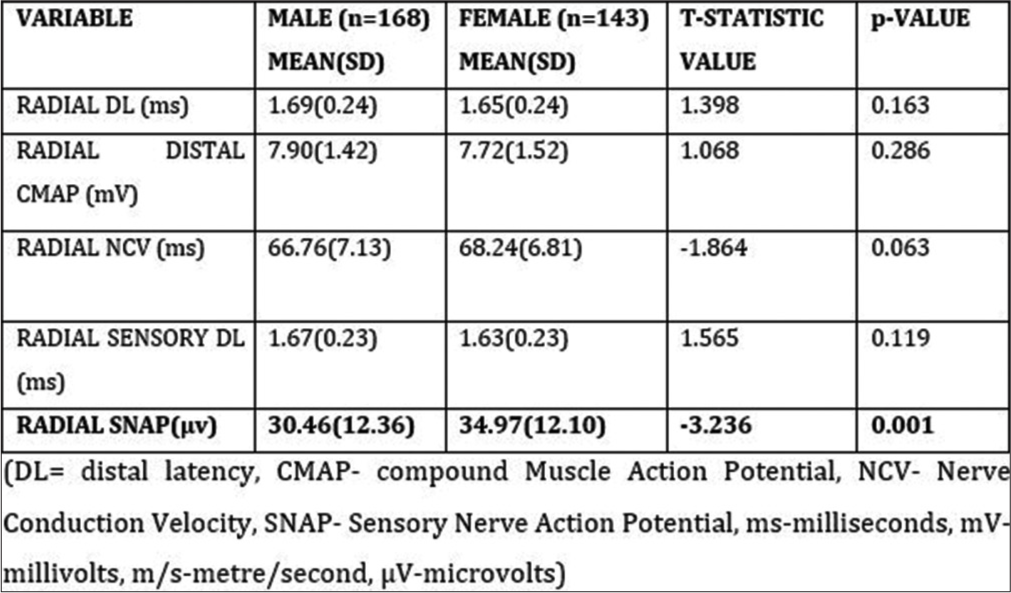
- Correlation of the left radial nerve conduction parameters with gender. Parameters (variable) entered in bold values indicates significant p-value.
DISCUSSION
Median nerve
The median motor distal latency of the right and left upper limbs in our study was 2.82 ± 1.10 ms and 2.86 ± 1.47 ms, respectively. This value was lower than most of the studies that were conducted in Kerala[8], other parts of India and the world.[1,2,9-18] The lower values in our study may be due to a higher sample size than the other studies, strict exclusion of asymptomatic carpal tunnel syndrome and a higher percentage of the younger population in the study group causing lower distal latency. The values of motor distal amplitude, conduction velocity, median sensory latency, sensory amplitude and median F-wave min latency were in agreement with other studies.[1-2,5-6,9,10,12-15,19-20]
Ulnar nerve
The ulnar nerve motor distal latency, distal amplitude, conduction velocity, ulnar sensory distal latency distal amplitude and ulnar F-wave min latency values were in agreement with other studies.[1,2,5,6,9,10,12-15,19,20] The ulnar sensory distal latency, distal amplitude, and ulnar F-wave min latency values were similar to that of Pawar et al.[17], Ahammed Naseem et al.,[8] Kumari et al.,[20] Garg et al.,[15] Robinson et al.,[2] Oh,[21] Kimura,[18] Balasubramaniam et al.[13] and Shehab,[9] Hennessey et al.[12,22,23]
Radial nerve
The radial motor distal latency of the right and left upper limb in our study was 1.66 ± 0.25 ms and 1.67 ± 0.24 ms, respectively. This was lower when compared to studies done by Chouhan,[24] Gassel and Diamantopoulos,[25] Jebsen[26] and Young et al.[27] The distal amplitude and nerve conduction velocity values were in agreement with the previous studies.[24-27] The sensory distal latency in our study was lower, and sensory distal amplitude was higher as compared to the study done by Chouhan.[24] The lower values of motor and sensory latency and higher distal sensory amplitude as compared with another study may be due to the higher sample size and the higher percentage of the younger study population.
It was observed in our study that as age increases, motor and sensory distal latency increases, F-wave latency prolongs motor and sensory amplitude decreases, and conduction velocity becomes slow. The reason for this is decreased nerve fibres, reduction in nerve diameter and change in fibre membrane and myelination due to ageing.[3,28,29] We found that as the height increases, motor and sensory distal latency increases and F-wave latency prolongs, motor and sensory amplitude decreases, and conduction velocity becomes slow. A study done on North Kerala population by Ahammed Naseem et al.[8] established that height influenced nerve conduction parameters. We observed that as the weight increases, motor and sensory distal latency increases, and F-wave latency prolongs, motor and sensory amplitude decreases, and conduction velocity becomes slow.
In this study, BMI had a significant positive correlation with the right F-wave median latency and a significant negative correlation with the left radial distal latency. No other correlation was obtained for the ulnar nerve and the other parameters of the median and radial nerves. Other investigators showed significant slowing of conduction and decreased amplitude in people with high BMI.[6,30-32] This may be due to the majority (57.23%) of normal BMI group in our study.
In our study, we found that females had significantly faster conduction velocity and higher right and left median, ulnar and radial sensory distal amplitude and lower median sensory, median F-wave latency, right and left ulnar distal latency, ulnar sensory latency and ulnar F-wave latency compared to males. The possible cause of gender differences in median and ulnar sensory amplitude study may be related to smaller finger circumference in females.[3] The less subcutaneous tissue in fingers closer to the recording of sensory response in females can explain the higher SNAP amplitude than in males.[3,33] The strengths of this study lay in the large sample size, excluding asymptomatic carpal tunnel syndrome and the involvement of the teenage population. We acknowledge that this study did not evaluate the technical factors and temperature which may influence the nerve conduction study. We recommend that age-adjusted, weight-adjusted, height-adjusted and gender-adjusted reference data be created to avoid misinterpretations of the nerve conduction study and, hence, the diagnosis.
CONCLUSION
The normative motor conduction, sensory conduction and F-wave latency values of median, ulnar and radial nerves were established. Therefore, while performing NCS, it is essential to adapt values based on physiological factors such as age, gender and height which enhance the diagnostic sensitivity of the procedure.
Ethical approval
The research/study was approved by the Institutional Review Board at Government Medical College, Kozhikode, number GMCKKD/RP2021/IEC/273, dated 05 October 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Normative data for median nerve conduction in healthy young adults from Punjab, India. J Neurosci Rural Pract. 2017;8(Suppl 1):S83-8.
- [Google Scholar]
- Influences of height and gender on normal nerve conduction studies. Arch Phys Med Rehabil. 1993;74:1134-8.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of age, sex, and anthropometric factors on nerve conduction measures. Muscle Nerve. 1992;15:1095-104.
- [CrossRef] [PubMed] [Google Scholar]
- Gender and arm length: Influence on nerve conduction parameters in the upper limb. Arch Phys Med Rehabil. 1994;75:265-9.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of age, gender, height, and weight on late responses and nerve conduction study parameters. Acta Neurol Taiwan. 2009;18:242-9.
- [Google Scholar]
- Nerve conduction study among healthy Malays. The influence of age, height and body mass index on median, ulnar, common peroneal and sural nerves. Malays J Med Sci. 2006;13:19-23.
- [Google Scholar]
- Effect of aging on sensory nerve conduction study parameters. Muscle Nerve. 2004;29:716-20.
- [CrossRef] [PubMed] [Google Scholar]
- Normative data of upper limb motor nerve conduction in Northern Kerala population and effect of height on motor nerve conduction velocity. Natl J Physiol Pharm Pharmacol. 2016;6:340-4.
- [CrossRef] [Google Scholar]
- Normative data of nerve conduction studies in the upper limb in Kuwait: Are they different from the western data? Med Princ Pract. 1998;7:203-8.
- [CrossRef] [Google Scholar]
- Normative values for nerve conduction study among healthy subjects from Aurangabad, India. Int J Recent Trends Sci Technol. 2013;8:56-61.
- [Google Scholar]
- Motor and sensory ulnar nerve conduction velocities: Effect of elbow position. Arch Phys Med Rehabil. 1983;64:227-32.
- [Google Scholar]
- Median and ulnar nerve conduction studies: Normative data for young adults. Arch Phys Med Rehabil. 1994;75:259-64.
- [CrossRef] [PubMed] [Google Scholar]
- Upper limb nerve conduction parameters of healthy young adults. Asian Pac J Health Sci. 2016;3:121-6.
- [CrossRef] [Google Scholar]
- Gender effect on upper limb nerve conduction study in healthy individuals of North India. J Pharm Biomed Sci. 2013;33:1589-93.
- [Google Scholar]
- Nerve conduction studies in the upper limb in the Malwa region-normative data. J Clin Diagn Res. 2013;7:201-4.
- [CrossRef] [PubMed] [Google Scholar]
- Nerve conduction studies in healthy Iraqis: Normative data. Iraqi J Med Sci. 2009;7:75-92.
- [Google Scholar]
- Normative data of upper limb nerve conduction in Central India. Indian J Physiol Pharmacol. 2011;55:241-5.
- [Google Scholar]
- Principles and pitfalls of nerve conduction studies. Ann Neurol. 1984;16:415-29.
- [CrossRef] [PubMed] [Google Scholar]
- Motor nerve conduction studies of median nerve in young adult group. Int J Bio Med Res. 2012;3:1751-3.
- [Google Scholar]
- Influence of age, height, gender on median and ulnar nerve conduction study. Natl J Physiol Pharm Pharmacol. 2018;8:202-6.
- [Google Scholar]
- Clinical electromyography: Nerve conduction studies Baltimore: Williams and Wilkins; 1993. p. :13-696.
- [Google Scholar]
- The study of F-waves in normal healthy individuals. Internet J Neurol. 2013;16:1-8.
- [Google Scholar]
- F-wave latency in healthy subjects. 2011. Erisim. Available from: https://medind/nic/in/jaw/t10/i2/jawt10i2p59/pdf [Last accessed on 2023 Sep 04]
- [Google Scholar]
- Normal motor and sensory nerve conduction velocity of radial nerve in young adult medical students. J Clin Diagn Res. 2016;10:CC01-3.
- [CrossRef] [PubMed] [Google Scholar]
- Pattern of conduction times in the distribution of the radial nerve: A clinical and electrophysiological study. Neurology. 1964;14:222-31.
- [CrossRef] [PubMed] [Google Scholar]
- Motor conduction velocity of distal radial nerve. Arch Phys Med Rehabil. 1966;47:12-6.
- [Google Scholar]
- Standardized nerve conduction studies in the upper limb of the healthy elderly. Am J Phys Med Rehabil. 1992;71:263-71.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of aging on nerve conduction velocities and late responses in healthy individuals. J Neurosci Rural Pract. 2018;9:112-6.
- [CrossRef] [PubMed] [Google Scholar]
- Ulnar nerve motor conduction velocity correlates with body mass index in Indian young healthy subjects. Natl J Physiol Pharm Pharmacol. 2018;8:310-3.
- [CrossRef] [Google Scholar]
- Effect of height and BMI on nerve conduction velocity. Indian J Clin Anat Physiol. 2015;2:231-4.
- [CrossRef] [Google Scholar]
- Association of nerve conduction velocity with total body fat mass and body mass index in type 2 diabetes mellitus. J Clin Diagn Res. 2020;14:CC04-7.
- [CrossRef] [Google Scholar]
- Human sensory nerve compound action potential amplitude: Variation with sex and finger circumference. J Neurol Neurosurg Psychiatry. 1980;43:925-8.
- [CrossRef] [PubMed] [Google Scholar]




