
Translate this page into:
Perspectives of medical undergraduate students toward self-directed learning
*Corresponding author: M. Kiran, Department of Pharmacology, Mysore Medical College and Research Institute, Mysuru, Karnataka, India. drkiranmaiya8@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kiran M, Hema NG. Perspectives of medical undergraduate students toward self-directed learning. Indian J Physiol Pharmacol. 2024;68:176-80. doi: 10.25259/IJPP_30_2023
Abstract
Objectives:
Self-directed learning (SDL) is a process in which individuals take the initiative with or without the help of others in diagnosing their learning needs, formulating goals, identifying human as well as material resources for learning, implementing appropriate strategies and evaluating learning outcomes. In SDL, the onus of learning is on the learner and learning control is slowly transferred from facilitator to learner. Hence, this study helped to understand the SDL readiness in undergraduate medical students and figure out whether it differed between students of 2nd and 3rd professional years.
Materials and Methods:
The study was conducted on undergraduate medical students of 2nd and 3rd professional year of tertiary care medical college hospital in south India after receiving permission from the Institutional Ethics Committee. A total of 285 students were considered in this study from both years after informed consent. A pre-validated questionnaire of the self-rating scale for SDL (SRSSDL) tool was included, and it comprised five components, namely, awareness, learning strategy, learning activity, evaluation and interpersonal skills, with 12 questions in individual sections. Demographic data were expressed in percentages while the Chi-square test and independent sample Mann–Whitney U-test were applied to understand the differences between 2 professional years.
Results:
Out of 285 students, 56.8% had a moderate level of readiness, followed by a high level of readiness (42.9%). The majority of the students from both academic years had a moderate level of readiness toward SDL. Learning strategy had the highest mean response score of 3.7 ± 0.52, followed by awareness with 3.69 ± 0.49. This mean score reflects that the majority of participants’ responses recorded were either ‘sometimes’ or ‘often’ for various components of the SRSSDL tool. The distribution of awareness, learning strategy, learning activities, evaluation and interpersonal skills did not show any significant association across academic years and gender.
Conclusion:
The moderate level of readiness shows that areas of improvement must be identified and evaluated with teacher guidance when necessary. The SRSSDL tool can be used as a measure of evaluation, as it helps to classify student readiness toward SDL.
Keywords
Medical undergraduates
Self-directed learning
Self-rating scale for self-directed learning

INTRODUCTION
The objective of medical education is to enrich the knowledge and skills along with empowering Indian medical graduates to be good clinicians, leaders and lifelong learners, according to the competency-based medical education (CBME) curriculum of India.[1] Self-directed learning (SDL) is ‘a process in which individuals take the initiative with or without the help of others in diagnosing their learning needs, formulating goals, identifying human as well as material resources for learning, choosing and implementing appropriate strategies and evaluating learning outcomes’.[2] It comprises knowledge acquisition, accumulation and retrieving information by which the learner inculcates skills for effective SDL. The teacher takes up the role of facilitator and guides the learner about ‘learn how to learn’.[3] In SDL, the onus of learning is on the learner and learning control is slowly transferred from facilitator to learner.[4] The level of self-tuning of learners’ is found to be firmly correlated to their motivation, endurance, and academic performance.[5] When SDL was included in the CBME curriculum to a larger extent, it was misinterpreted as lone-reading or instructing the students to refer to the books in an unattended manner. It was included in the teaching schedule as an ill-planned session.[6] In higher education institutions such as professional courses, feedback and student evaluation is an integral element to measure the quality of learning they cater to. Assessment of student learning/effective teaching and course/content assessment has provided importance to preserving academic calibre, quality and relevance of course layout and delivery in the past few decades.[7] In 2007, Williamson devised the self-rating scale of SDL (SRSSDL), which is an efficient teaching/learning instrument. This tool caters a chance for learners to reflect on their behaviour and learning curve as well as be self-driven.[4] Self-learning skills have to be incorporated into students for lifelong and continuous academic development. Evaluating the SDL readiness among medical students will help the academicians to deduce the intent of education for SDL. Hence, the objective of the study was to understand the SDL readiness in undergraduate medical students and deduce whether SDL readiness varied between students of 2nd and 3rd professional years.
MATERIAL AND METHODS
Study design
This cross-sectional study was conducted in September 2022 for 2 days in a tertiary care teaching hospital in south India after receiving permission from the Institutional Ethics Committee (MMCRI/ECR/134/RR-19).
Study participants
A total of 285 undergraduate medical students in both 2nd and 3rd professional years were included, and the sample size was derived using a purposive sampling method.
Study instrument
SRSSDL Tool, which is a pre-validated and self-assessment tool for students to monitor their learning skills, was used as a study instrument. SRSSDL scale is a free-to-use scale, and permission from the original authors was requested through the mail. The scale includes 60 learning behaviour statements under five broad categories of awareness, learning strategies, learning activities, evaluation and interpersonal skills, with 12 questions in each section. Students’ responses for every statement are recorded using a five-point rating scale, following which the scores are calculated and interpreted, as shown in Figure 1.[8]
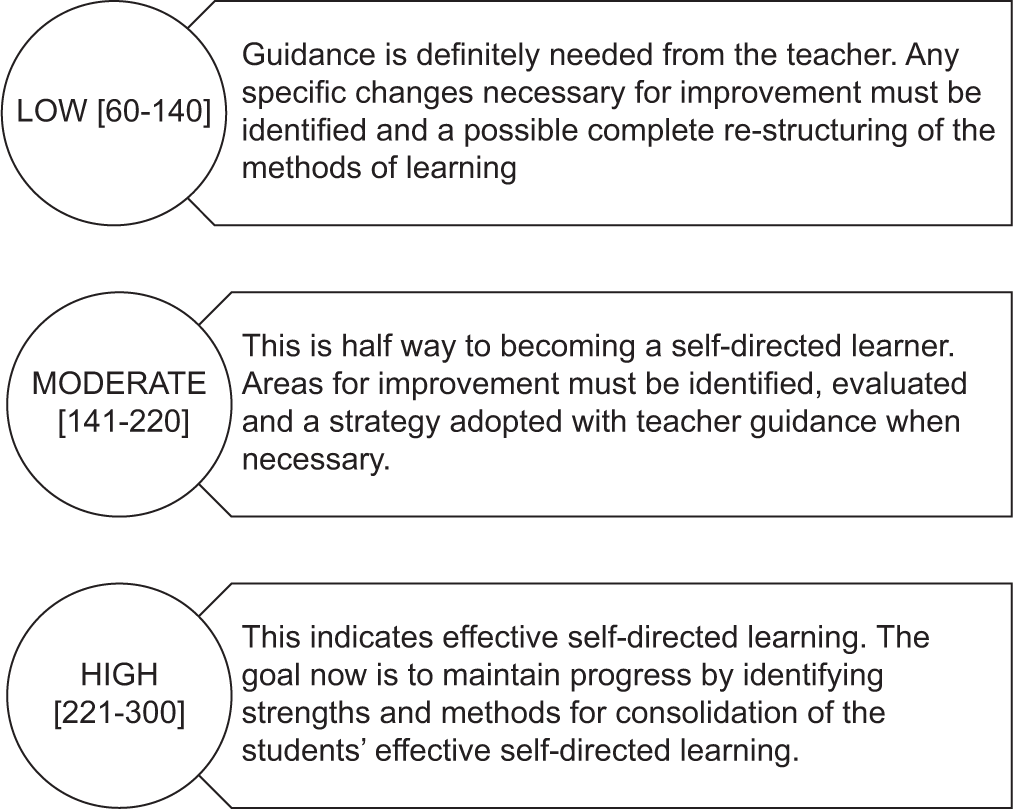
- Self-rating scale for self-directed learning score and its interpretation.
The data were recorded with a self-administered pre-validated SRSSDL tool, which was provided to the students of 2nd and 3rd professional years of undergraduate medical students in two separate sessions through online Google Form after they were briefed about the intent of the study and manner of filling the study instrument. They were given a duration of 48 h to fill the form and record the response. The consent to be a part of the study was mentioned in the form as a check box, and the students were not compelled to take part in the survey.
Statistical data analysis
Demographic data were expressed in numbers and percentages, while results from analyses of the SRSSDL tool were expressed as mean and standard deviation. The Chi-square test and independent sample Mann–Whitney U-test were used to analyse the difference between 2 professional years. P = 0.05 or less to be considered significant.
RESULTS
The study was conducted on medical undergraduates in 2nd—and 3rd-year MBBS. A total of 285 participants took part in the study from both academic years. The demographic features of students are summarised below in Table 1.
| Parameter | Number (n=285) | Percentage |
|---|---|---|
| Professional year | ||
| Second | 137 | 48.1 |
| Third | 148 | 51.9 |
| Gender | ||
| Male | 179 | 62.8 |
| Female | 106 | 37.2 |
n: Number of students
The SRSSDL tool was considered to evaluate the readiness of students for SDL. Out of 285 students had a moderate level of readiness (56.8%) followed by a high level of readiness (42.9%). The majority of the students from both professional years had a moderate level of readiness toward SDL, as shown in Figure 2.
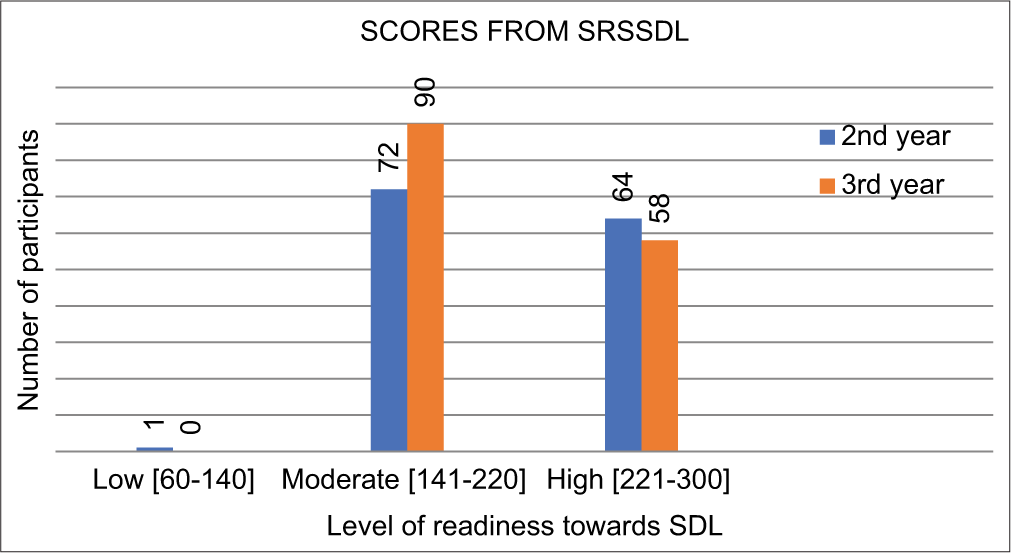
- Level of readiness of study participants of both professional years. SRSSDL: Self-rating scale for self-directed learning, SDL: Self-directed learning.
Five components of the SRSSDL tool were analysed to obtain the mean response score of the study participants, which is depicted in Table 2. This mean score reflects that the majority of participants’ responses recorded were either ‘sometimes’ or ‘often’ for various components of the SRSSDL tool. To understand whether academic year and gender influenced the scoring of the SRSSDL tool, subgroup analysis using an independent sample Mann–Whitney U-test was performed, which is depicted in Table 2. The distribution of awareness, learning strategy, learning activities, evaluation and interpersonal skills did not show any significant association across academic year and gender.
| Components | Mean±SD | -value* | |
|---|---|---|---|
| Year | Gender | ||
| Awareness | 3.69±0.49 | 0.07 | 0.48 |
| Learning strategy | 3.7±0.52 | 0.48 | 0.36 |
| Learning activities | 3.53±0.55 | 0.75 | 0.48 |
| Evaluation | 3.58±0.57 | 0.65 | 0.3 |
| Interpersonal skill | 3.61±0.6 | 0.8 | 0.59 |
The Chi-square test was used to analyse any significant association regarding readiness toward SDL between 2nd year and 3rd year MBBS students. Students felt peer coaching, group discussions and role play as an effective way for complex learning. They consider the teacher as a facilitator. All the questions which showed significant differences are shown in Table 3.
| Question | Chi-square statistic (P-value*) |
|---|---|
| I consider teachers as facilitators of learning rather than providing information only | 12.46 (0.01) |
| I have a break during long periods of work | 11.62 (0.02) |
| I need to keep my learning routine separate from my other commitments | 15 (0.05) |
| I feel that I am learning despite not being instructed by the lecturer | 12.34 (0.01) |
| I participate in group discussions | 39.35 (0.000) |
| I find peer coaching effective | 15.17 (0.004) |
| I find role play is a useful method for complex learning | 25.52 (0.000) |
| I find interactive teaching-learning sessions more effective than just listening to lectures | 14.39 (0.006) |
| My inner drive directs me toward further development and improvement in my learning | 18.48 (0.001) |
| I arrange my self-learning routine in such a way that it helps develop a permanent learning culture in my life | 14.63 (0.006) |
| I raise relevant questions in teaching-learning sessions | 9.18 (0.05) |
| I am able to analyse and critically reflect on ideas, information or any learning experiences | 14.92 (0.05) |
| I find both success and failure inspire me to further learning | 9.38 (0.05) |
| I am able to identify my role within a group | 10.12 (0.03) |
DISCUSSION
CBME emphasises Indian Medical Graduates function as lifelong learners and have a continuous commitment to improve knowledge and skills.[1] Primarily SDL is an advanced level active learning method that improves cognitive skills and accelerates self-sufficiency in learning of the students where the responsibility of learning is inclined toward the students.[9] Goal achievement, autonomous behaviour, self-handling and motivation are a few of the personal attributes necessary for SDL to be effective.[2]
Wang and Holcombe advise that the sustainability of self-moderated learning relies considerably on the level of persistence and effort the learner devotes to achieve the assigned tasks.[10] Badyal et al. recommend that SDL if conducted appropriately, can have a high impact on medical education. The orientation of facilitators and the readiness of students must be considered well in advance to introduce SDL sessions efficiently.[11] Patra et al. observed that 67% of the students were satisfied, and 66% were driven to study further following the SDL session.[12] Hence, SDL can be considered an effective method of learning in motivated learners.
A confirmatory factor analysis was performed by Cadorin et al. to assess the validity of the SRSSDL tool, and it was found that it contributes to determining learning requirements among students and healthcare professionals. This helps facilitators to recognise and include tactics to improve SDL potential.[13] However, Greveson and Spence have observed that contextual factors such as cultural, social, past experiences and educational settings impact the motivation and ability of learners to be self-directed. This may explain the concerns of learners’ difficulty and stability across different health professional groups and varying learning backgrounds.[14]
In our study, the SRSSDL tool, which was used to analyse the readiness of students toward SDL, showed that 56.8% had a moderate level and 42.9% with a high level of readiness, which was similar to the findings by Madhavi and Madhavi 64 and 36 readiness toward moderate and high levels.[15]
Koirala et al. observed the various factors affecting the readiness for SDL and found that grade and performance in the previous academic year exerted a significant association (P = 0.025) with SRSSDL levels.[16] In a study by Atta and Alghamdi for assessing the effectiveness of SDL against problem-based learning, it was observed that SDL proves to be less valuable for promoting self-readiness in students with low scores in SRSSDL and frequent sessions in small groups or panel discussions are strongly advocated for students to improve readiness with SDL.[17]
In our study, there was no significant association in the distribution of various components of the SRSSDL tool with gender, which was similar to findings by Gyawali et al. conducted on 1st-year medical students.[18]
Prachita and Vrushali found that clinical students had significantly higher mean total SRSSDL scores as compared to pre-clinical students in all subdivisions of the tool, while Linda et al., in their study, noted that 1st professional year students’ scores were considerably high on SRSSDL scale subcategories. This was attributed to students who casually recorded answers with respect to their belief that they should be essential and that they overestimated their strength of SDL skills or exhibited threshold effect and/or social desirability bias.[19,20] In contrast to above findings, our study did not show any significant difference in mean total SRSSDL score among students of 2nd and 3rd professional years.
Few components, such as the inclusion of role play, group discussion and peer tutoring in the SRSSDL questionnaire, showed statistically significant values in our study. Sourya et al. observed that role-play could be utilised as an effective method for learning medicine as there was a significant improvement in the cognitive, affective and psychomotor domains.[21] The same findings were reflected in our study as students felt role-play to be a useful method for complex learning. Roshni and Rahim, in their study, were in favour of group discussion as the scores for overall learning experience were found to be significantly higher for a group discussion as compared to the lecture. They strongly advocated that it improves the duration of attentiveness in students, analysing the concepts and recall, which was similar to our findings.[22] Burgess et al. found that students were of the opinion that peer mentoring program offers opportunities as it provides a framework within the medical syllabus for students to practice and enrich their medical knowledge and academic expertise.[23]
Limitation
Long-term outcomes after categorising students based on their readiness were not evaluated; this can be taken up as further scope of our study. This study was conducted to understand the readiness or perception of students toward SDL based on their prior sessions and experience in previous academic years. The SRSSDL scale is lengthy and time-consuming as it includes sixty questions, which can hinder students from giving prompt responses. It is a scale which was initially designed to analyse the readiness of nursing students toward SDL and is not extensively used for medical students.
CONCLUSION
The moderate level of readiness in the majority of students shows that areas of improvement must be identified and evaluated with teacher guidance when necessary. The suitability of SDL as a learning method in students can be measured with the SRSSDL tool, as it helps to classify the student readiness toward SDL and its acceptance. Future studies under these categories are needed before larger consideration of the SRSSDL tool for surveys in medical education can be done.
Acknowledgment
We would like to thank the Head of Department of Pharmacology for his support and guidance in conducting the study.
Ethical approval
The research/study approved by the Institutional Review Board at MYSORE MEDICAL COLLEGE AND RESEARCH CENTRE, number MMCRI/ECR/134/RR-19, dated 02 August 2022.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Competency based undergraduate curriculum for the Indian medical graduate. 2018. New Delhi: Medical Council of India; Available from: https://www.mciindia.org/CMS/information-desk/for-colleges/ug-curriculum [Last accessed on 2022 Jul 25]
- [Google Scholar]
- Self-directed learning: A guide for learners and teachers New York: Cambridge Book Co.; 1975.
- [Google Scholar]
- Learning theories: The basics to learn in medical education. Int J Appl Basic Med Res. 2017;7:1-3.
- [CrossRef] [PubMed] [Google Scholar]
- Self-direction in a problem-based learning program. Nurse Educ Today. 2004;24:277-85.
- [CrossRef] [PubMed] [Google Scholar]
- Teaching writing to at-risk students: The quality of evidence for self-regulated strategy development. Except Child. 2009;75:303-18.
- [CrossRef] [Google Scholar]
- Self-directed learning readiness of Asian students: Students perspective on a hybrid problem-based learning curriculum. Int J Med Edu. 2016;7:385-92.
- [CrossRef] [PubMed] [Google Scholar]
- Student evaluation of the usefulness of the self-rating scale of self-directed learning tool in the FdSc in health and social care course. J Healthc Commun. 2017;2:48.
- [CrossRef] [Google Scholar]
- The development of self-rating scale of self-directed learning. Nurse Res. 2007;14:65-72.
- [CrossRef] [PubMed] [Google Scholar]
- Academic performance and the practice of self-directed learning: The adult student perspective. J Furth High Educ. 2017;41:44-59.
- [CrossRef] [Google Scholar]
- Adolescents' perceptions of school environment, engagement, and academic achievement in middle school. Am Educ Res J. 2010;47:633-62.
- [CrossRef] [Google Scholar]
- Triple Cs of self-directed learning: Concept, conduct, and curriculum placement. CHRISMED J Health Res. 2020;7:235-9.
- [CrossRef] [Google Scholar]
- Module to facilitate self-directed learning among medical undergraduates: Development and implementation. J Edu Health Promot. 2020;9:231.
- [CrossRef] [PubMed] [Google Scholar]
- The self-rating scale of self-directed learning tool: findings from a confirmatory factor analysis. J Nurs Edu Pract. 2017;7:31-7.
- [CrossRef] [Google Scholar]
- Self-directed learning-the importance of concepts and contexts. Med Educ. 2005;39:348-9.
- [CrossRef] [PubMed] [Google Scholar]
- Readiness for self-directed learning among undergraduate medical students of Andhra Medical College, Visakhapatnam. Int J Community Med Public Health. 2017;4:2836-40.
- [CrossRef] [Google Scholar]
- Factors affecting self-directed learning readiness of the undergraduate nursing students from Purbanchal university, Nepal: A cross-sectional study. J Chitwan Med Coll. 2021;11:31-5.
- [CrossRef] [Google Scholar]
- The efficacy of self-directed learning versus problem-based learning for teaching and learning ophthalmology: A comparative study. Adv Med Educ Pract. 2018;9:623-30.
- [CrossRef] [PubMed] [Google Scholar]
- Readiness for self-directed learning among first semester students of a medical school in Nepal. J Clin Diagn Res. 2011;5:20-3.
- [Google Scholar]
- Evaluation of self-directed learning readiness among undergraduate students in an Indian Physical Therapy Institute. Int J Sci Healthc Res. 2021;6:1-6.
- [CrossRef] [Google Scholar]
- An initial validation study of the self-rating scale of self-directed learning for pharmacy education. Am J Pharm Educ. 2018;82:280-6.
- [CrossRef] [PubMed] [Google Scholar]
- Role play-an effective tool to teach clinical medicine. J Contemp Med Edu. 2014;2:91-6.
- [CrossRef] [Google Scholar]
- Small group discussions as an effective teaching-learning methodology for learning the principles of family medicine among 2nd-year MBBS students. J Family Med Prim Care. 2020;9:2248-52.
- [CrossRef] [PubMed] [Google Scholar]
- Peer tutoring in a medical school: Perceptions of tutors and tutees. BMC Med Educ. 2016;16:85-92.
- [CrossRef] [PubMed] [Google Scholar]




