
Translate this page into:
Relation of interleukin-17 and high-sensitivity C-reactive proteins with sympathetic reactivity in pre-hypertensive young adult
*Corresponding author: Yogesh Saxena, Professor, Department of Physiology, Himalayan Institute of Medical Sciences, Swami Rama Himalayan University, Dehradun, Uttarakhand, India. drysaxena@rediffmail.com
-
Received: ,
Accepted: ,
How to cite this article: Saxena Y, Gupta R, Kotwal A, Ojha A. Relation of interleukin-17 and and high-sensitivity C-reactive proteins with sympathetic reactivity in pre-hypertensive young adult. Indian J Physiol Pharmacol 2020;64(3):221-8.
Abstract
Objectives:
Recent studies have shown that both innate and adaptive immunity response contributes to vascular dysfunction by vascular remodelling and later hypertension. Furthermore, the sympathetic activity mediates the vascular dysfunction through pro-inflammatory activity of immune system. In context to insidious onset hypertension, the study was planned to observe the association of immunity with the increased sympathetic activity in pre-hypertensive adults.
Materials and Methods:
Thirty healthy pre-hypertensive (as per JNC VII) non-smokers, non-alcoholic and non-obese male adults volunteers were recruited from the study area. Equal numbers of normotensive controls were taken for comparison. On reporting day, they were subjected to the recording of demographic and anthropometric measurements, hand grip dynamometry and later investigated for serum levels of interleukin-17 (IL-17) and high-sensitivity C-reactive proteins (hsCRP) after written informed consent. The data collected were analysed for differences in mean and association of immune and inflammatory markers with sympathetic activity by statistical tests.
Results:
Significantly higher values of weight, BMI, % BF, visceral fat, resting heart rate and IL-17 and a lower sympathetic reactivity was observed in pre-hypertensive subjects. Values of hsCRP was higher in prehypertensive but was not statistically significant.. IL-17 was a positive significant predictor with 4.7 times (P = 0.02) increase in odds of being pre-hypertensive, whereas sympathetic reactivity was a significant negative predictor (OR = 0.75; P = 0.001). SBP and DBP are both related negatively and significantly (P < 0.05) to the sympathetic reactivity suggesting that blood pressure is related to sympathetic nervous system. Furthermore, the hsCRP is observed to be related positively to the % BF and to only SBP and RHR, complimenting link of adiposity as an inflammatory process to blood pressure. IL-17 levels in blood are observed to be positively and significantly related to DBP.
Conclusion:
Elevated IL-17 levels are significant predictor of pre-hypertension along with lower sympathetic reactivity. No direct association was observed between IL-17 and sympathetic system except with raised DBP. Immune mechanism is part of pathogenesis of increased blood pressure in pre-hypertensive with enhanced baseline sympathetic activity.
Keywords
Pre-hypertensive
Interleukin-17
high-sensitivity C-reactive proteins
Sympathetic reactivity

INTRODUCTION
Pathophysiology of hypertension involves the infiltration of the vascular adventitia and perivascular adipose tissue by inflammatory immune cells. Recent studies have shown that both innate and adaptive immunity response contributes to vascular dysfunction by vascular remodelling and later hypertension.[1,2]
Early animal studies have observed the infiltration of T lymphocytes in kidney of hypertensive animals and their low number or absence is associated with lower blood pressure.[3] Further evidence showed that although there is almost always presence of T lymphocytes in hypertensive animals, their absence is not associated with vascular dysfunctions. Furthermore, adaptive transfer of T cells and not B cells restored the hypertensive response and vascular abnormalities in these animals.[4] Since polarisation of T cells is dependent on the activation of macrophages and dendritic cells which are the parts of innate immune system, it may be linked to immune and inflammatory disorders.
Autoimmune and inflammatory disorders development have been linked to the subset of T helper cells that secrete the interleukins 17, (for their actions), levels of which found to be raised in (being) several of the autoimmune and inflammatory disorders such as rheumatoid arthritis, psoriasis multiple sclerosis and inflammatory bowel disease.[5] Recent evidence also suggests the involvement of interleukin-17 (IL-17) in cardiovascular diseases including coronary atherosclerosis and hypertension when compared to those with BP <120/80 mmHg.[6]
Sympathetic overactivity can activate adaptive immune cells through β2-adrenergic receptors (ARs) that are expressed especially on T cells[7] and cytokines released form activated immune cells serve as messengers to the brain, to provide immune system functional information that is utilised by the sympathetic nervous system (SNS) to coordinate all the systems required for an appropriate immune response.[8] Pre-clinical studies provide evidence indicating that the production of cytokines, including interleukin-17, contributes to high blood pressure, likely through the effects on both the kidney and vasculature. IL17 peripherally causes a pro-inflammatory milieu in smooth muscle upregulating several genes of inflammation[2] to induce phosphorylation of the endothelial NO synthase impairing the endothelium- dependent vasodilatation.[9]
Since IL-17 plays a critical role in hypertension and has been found raised in pre-hypertension,[7,10] it was hypothesised that along with other factors, IL-17 might contribute to the vascular inflammation in pre-hypertension. Furthermore, the cardiovascular damage caused by excessive stimulation of the SNS and their receptors (α- and β-adrenergic receptors) is mediated through a pro-inflammatory activation of the immune system.[11]
With multiple studies[12,13] having demonstrated an increased sympathetic activity in pre-hypertensive subjects the study was proposed to investigate serum levels of IL-17 in prehypertensive and to evaluate the relationship of IL-17 with inflammatory and sympathetic activity in pre-hypertension in young adult population.
MATERIALS AND METHODS
This observational analytical study was conducted in the Department of Physiology, Himalayan Institute of Medical Sciences, Swami Ram Nagar, Dehradun, over a period of 12 months. The study subjects were recruited from a representative group of residents, employees and students of Swami Ram Himalayan University, Dehradun, to complete the sample size for each group. A sample size of 26 in each group was obtained using the sampling size formula for the differences of means for serum IL-17 between normotensive and pre-hypertensive[10] of 1.9 at 80% of power and an α error of 0.05 with population variance of 6. To improve the strength of the study and considering dropouts of participants of 10%, a sample size of 30 in each group was reached.
Inclusion criteria for pre-hypertensive group (n=30) were apparently healthy subjects with the blood pressure – systolic 120–139 mmHg and/or a diastolic 80–89 mmHg and for normotensive group (n = 30) were apparently healthy subjects with blood pressure systolic < 120 mmHg and diastolic < 80 mmHg as per the JNC VII criteria.[11,14]
Exclusion criteria were common for normotensive and prehypertensive groups and consisted of history of any chronic disease such as DM and hypertension, history of smoking/ alcohol consumption/active infection and those with BMI ≥30 kg/m2.
The recruited subjects were asked to report to the department of physiology in the morning hours after a good night’s rest and following a light breakfast. Volunteers were asked to avoid caffeine and any kind of physical exercise in the past 24 h. They were subjected to the following investigation after written informed consent.
Medical history
Relevant medical history (based on exclusion criteria) was taken, including history of present illness, past illness, personal history, drug history, family history and history of allergic reactions
Clinical examination was done to rule out active and chronic infection.
Baseline characteristics
Demographic indices and basal physiologic parameters were recorded that included name, age, gender, address, occupation, basal systolic and diastolic blood pressure and resting heart rate (RHR).
Obesity indices measurement
Body weight, percentage body fat, BMI and visceral fat were measured using an impedance body composition analyser. The instrument works on a patented foot to foot pressure contact electrode bioelectrical impedance analysis technique. The subjects after emptying bladder were asked to stand barefoot and with minimal clothing on the foot pad of the instrument. They were told to stand there till the reading was displayed on the panel
Sympathetic reactivity by sustained hand grip (SHG) method.
Baseline BP and HR were recorded in sitting position. The subject was asked to hold the dynamometer in the non-dominant hand, with the arm by the side of the body, with the pointer on the dial adjusted at zero and the base rested on the palm. Before the test, maximum voluntary contraction (MVC) was recorded. The subject was instructed to squeeze the dynamometer with maximum isometric effort for at least 5 s and the result was recorded, no other body movement was allowed. After this, the subject was asked to press hand grip dynamometer at 30% of MVC for 3 min.[15] The alteration in the BP and HR just before the release of hand grip was taken as the index of response to hand grip test. The relative consistency of the hemodynamic changes which occur during the isometric handgrip exercise test indicates that it is a simple and a reliable method for studying the cardiovascular response to stress.[16]
Immunological and inflammatory markers
Blood sampling for serum IL17 and and high-sensitivity C-reactive proteins (hsCRP) was done under basal conditions and after taking aseptic precautions. The samples were collected from cubital vein in a plain yellow top Vacutainer for the estimation of IL17 and hsCRP estimation at NABL certified immunology laboratory of hospital. The freshly collected samples were centrifuged for 15 min and serum stored at –80°C until further analysis. Serum samples were thawed and quantitative measurements of IL17 and hsCRP will be performed by immunoassay method using a commercially procured kit.
RESULTS
The study was conducted on 30 pre-hypertensive volunteers with equal number of controls. Descriptive analysis of baseline parameters of demographic, anthropometry and cardiovascular parameters observed that the two groups were homogenous with age, height and weight. Indices of obesity including BMI, % body fat (%BF) and five of visceral fat (VF) were significantly different between the two groups with prehypertensive having a higher value for the variables than normotensive. Significantly higher values of RHR were also observed in pre-hypertensive group. As would be expected, the groups were different for the mean arterial pressure (MAP) with pre-hypertensive subjects having a higher MAP as compared to normotensive [Table 1].
| Parameters | Normotensive (n=30) | Pre-hypertensive (n=30) | P-value |
|---|---|---|---|
| Age (years) | 30.39±7.1 | 31.07±7.2 | 0.714 |
| Height (cm) | 169.70±6.96 | 169.58±4.97 | 0.935 |
| Weight (kg) | 68.0±11.5 | 72.6±9.51 | 0.097 |
| BMI (kg/m2) | 23.49±3.25 | 25.21±2.36 | 0.022 |
| %BF | 21.2±6.50 | 23.91±3.2 | 0.049 |
| VF% | 7.59±3.9 | 9.60±3.0 | 0.029 |
| RHR (beats/min) | 68.16±5.5 | 74.37±8.9 | 0.002 |
| MAP (mmHg) | 85.72±4.5 | 97.96±4.2 | 0.001 |
VF: Visceral fat, WC: Waist circumference, RHR: Resting heart rate, MAP: Mean arterial pressure
On analysis of sympathetic reactivity and blood inflammatory markers, it was observed that IL-17 was higher in pre-hypertensive in comparison to normotensive and the difference was significant. Sympathetic reactivity assessed by change in DBP following isometric exercise was significantly lower in pre-hypertensive than in normotensive [Table 2].
| Parameters | Normotensive (n=33) | Pre-hypertensive (n=33) | P-value |
|---|---|---|---|
| Change in DBP (mmHg) | 27±10.9 | 15.5±11.5 | 0.001 |
| #hsCRP (ng/ml) | 876.93 (451.5–2270.9) | 2189.8 (551.48–3481) | 0.051 |
| #IL-17 (pg/ml) | 2.96 (0.2–4.5) | 3.67 (2.1–5.7) | 0.039 |
Binary logistic regression analysis was applied to determine the independent role played by significantly different independent variables with pre-hypertensive. Model for prediction of being pre-hypertensive was statistically significant and could explain only 83.6% variability of the odds of prehypertension. It was observed that IL-17 value is positive and significant (b = 1.56; P= 0.02; OR = 4.79) predictor of probability of odds of pre-hypertensive with the OR indicating that for every one unit increases on this predictor the odds of pre-hypertensive change by a factor of 4.7 (the odds are increasing) with higher value of IL-17 more likely in pre-hypertensive than in normotensive. Sympathetic reactivity is negative and significant (b = –0.28; P = 0.001; OR =0.75 [CI 0.63–0.89]) predictor of probability of odds of pre-hypertensive and decreasing value is more likely to be pre-hypertensive than normotensive and the difference is statistically significant (P = 0.020) [Table 3].
| β | P-value | Odds ratio (CI) | |
|---|---|---|---|
| BMI | 0.284 | 0.673 | 1.329 (0.39–4.9) |
| % body fat | 0.087 | 0.610 | 1.090 (0.78–1.52) |
| VF % | –0.287 | 0.475 | 0.751 (0.34–1.6) |
| Sympathetic reactivity | –0.281 | 0.001 | 0.755 (0.63–0.89) |
| IL-17 (pg/dl) | 1.568 | 0.020 | 4.799 (1.2–17.6) |
[Table 4] shows correlation of significantly different risk factors and inflammatory markers with SBP and DBP (n=60).
| SBP | DBP | RHR | MAP | BMI | %BF | VF | Sympathetic reactivity | hsCRP ng/ml | IL-17 pg/ml | |
|---|---|---|---|---|---|---|---|---|---|---|
| SBP (mmHg) | 1 | 0.717** | 0.394** | 0.886** | 0.317* | 0.265* | 0.324* | –0.331** | 0.340** | 0.175 |
| DBP (mmHg) | 1 | 0.306* | 0.958** | 0.148 | 0.071 | 0.190 | –0.428** | 0.045 | 0.267* | |
| RHR | 1 | 0.365** | 0.134 | 0.163 | 0.106 | –0.107 | 0.265* | 0.034 | ||
| MAP | 1 | 0.228 | 0.156 | 0.260* | –0.420** | 0.169 | 0.249 | |||
| BMI (Kg/m2) | 1 | 0.791** | 0.936** | 0.094 | 0.250 | 0.171 | ||||
| %BF | 1 | 0.700** | .0032 | 0.385** | 0.096 | |||||
| VF | 1 | 0.066 | 0.384** | 0.113 | ||||||
| Sympathetic reactivity | 1 | 0.101 | –0.071 | |||||||
| hsCRP (ng/ml) | 1 | –0.038 | ||||||||
| IL-17 (pg/ml) | 1 |
SBP and DBP are both related negatively and significantly (P<0.05) to the sympathetic reactivity suggesting that blood pressure is related to SNS. Furthermore, the hsCRP is observed to be related positively to the % BF (P=0.001), VF (P=0.001), SBP (P=0.002) and RHR (P=0.019), complimenting link of adiposity as an inflammatory process to blood pressure. IL-17 levels in blood are observed to be positively and significantly related to DBP [Table 4]
SBP is positively but insignificantly related with obesity indices (BMI, %BF and VF) and hsCRP in normotensive but obesity markers are positively % significantly related with hsCRP as well as with sympathetic reactivity [Figure 1]. SBP although was significantly and positively related to obesity markers (BMI, %BF and VF) and hsCRP in pre-hypertensive [Figure 2].
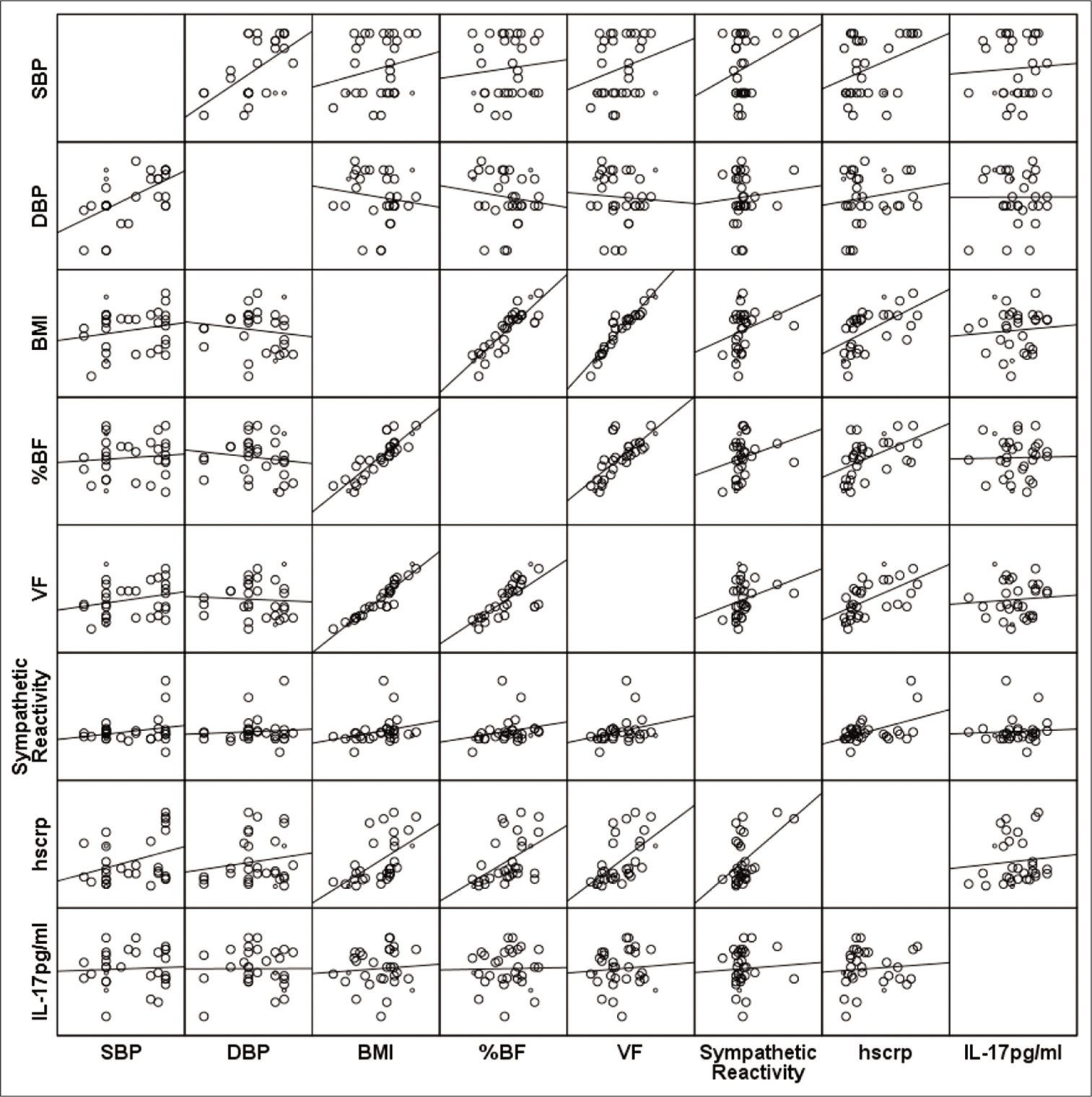
- Correlation matrix of blood pressure with obesity indices, sympathetic reactivity and inflammatory markers in normotensive.
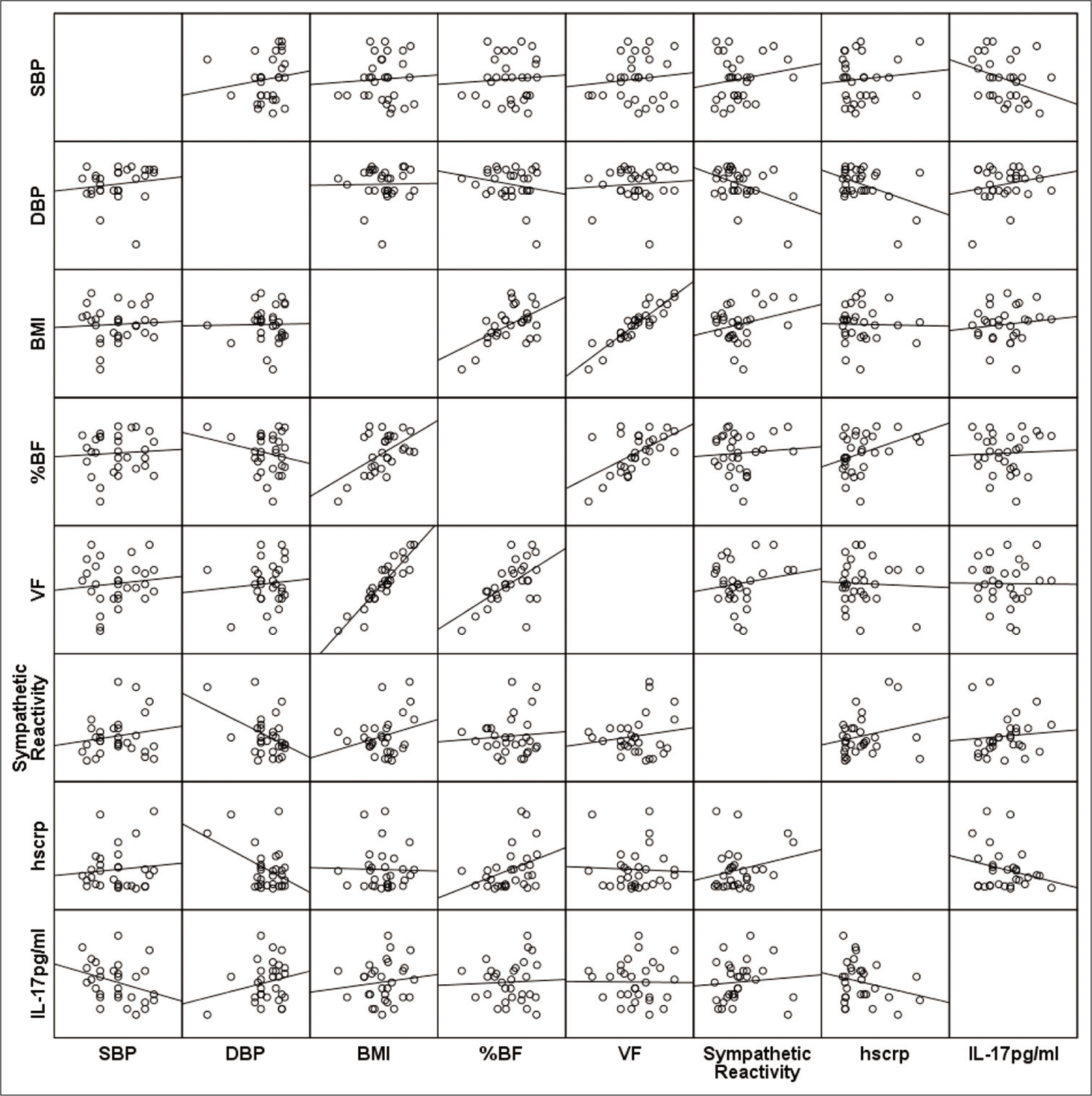
- Correction matrix of blood pressure with obesity indices, sympathetic reactivity and inflammatory markers in pre-hypertensive.
DISCUSSION
Inflammation of the vasculature, with an infiltration of immune cells, is a known and important pathological mechanism in the development of cardiovascular diseases, especially hypertension.[17] Recently, evidences also indicate that chronic low-grade inflammation is an important contributing factor in the development of prehypertension.[18,19] Along significant contribution from the immune system, an increase in SNS activity is also known to contribute in pathophysiology of pre-hypertension. Our study examined the levels of inflammatory (hs-CRP) and immune markers (IL-17) and investigated their association with the activity of SNS in pre-hypertensive young adults.
A total of 30 pre-hypertensive subjects from 20 to 40 years of age and equal number of age- and height- matched normotensive were investigated. Obesity indices BMI, % BF and %VF were found to be significantly higher in prehypertensive subjects but were in non-obese levels and correlated well with the previous studies.[20,21] RHR was significantly increased in pre-hypertensive subjects in our study which can be attributed to higher basal sympathetic tone. High sympathetic drive is one of the major factors in the development of high blood pressure[22] as evidenced by higher RHR in our study population. Evidence suggests that elevated blood pressure is initiated and maintained by increased sympathetic tone, generated by rostral ventrolateral medulla, which is influenced by cortical and hypothalamic impulses, blood-borne gases and chemicals including cytokines.[23] Contrary to our finding, study on African young pre-hypertensive adults observed a lower RHR than normotensive though not significant and in females.[24]
Change in DBP during SHG test[25] was used to assess the impaired sympathetic response. Significant difference in values of change in DBP was observed between normotensive and pre-hypertensive groups with the prehypertensive showing a lesser increase in the diastolic blood pressure following SHG test, which signifies increase in basal sympathetic tone and elevated basal DBP in prehypertensive subjects.[21,26] Both lesser rise in DBP, following SHG test[25] and raised RHR indicated (toward) an imbalance in sympathetic response in pre-hypertensive subjects.[27]
It has been postulated that the pressure response to the isometric exercise is reflex in origin, which serves to increase the perfusion pressure to the active muscles, in which the blood flow is impeded by the sustained muscular contraction.[28] This may be the reason for the increase in the peripheral resistance and, consequently, that in the diastolic pressure in our study. Significantly increased vascular resistance in pre-hypertensive young adults was also observed by Bond et al. in female African pre-hypertensive adults. Contrary to our finding, larger change in DBP of 40 mmHg versus 6 mmHg was observed in six pre-hypertensive females following SHG test P < 0.001 in comparison to normotensive.[24]
The present study, observed higher mean value of inflammatory marker hs-CRP though insignificant and a significantly higher immune marker IL-17 levels in prehypertensive as compared to normotensive, [P < 0.05 Table 2]. Corroborating to our finding study done by Wei Yao et al.[10] also observed a significant increase in the values of immune marker IL-17 in pre-hypertensive in the age group of >40–70 years comparison to normotensive subjects and also observed a significant higher levels of hsCRP in them. This suggests that immune dysfunction and vascular inflammation may already exist in pre-hypertensive individuals. The levels of IL-17 in our study were less than those reported in hypertensives. The insignificant difference in hsCRP levels between pre-hypertensive and normotensive observed in our study can be attributed to small sample size. Establishing the risk predictor for prehypertension, it was observed that only sympathetic reactivity (OR = 0.75) and IL-17 level (OR = 4.7) were able to increase the probability of odds of being pre-hypertensive. Significant direct relation of IL-17 with pre-hypertension independent of age, sex and BMI was also observed by Yao et al.[10] which also observed a linear relation of IL17 levels with SBP contrary to our finding. Contrary to several other studies,[29,30] no association of hsCRP could be observed with pre-hypertension.
Significant positive correlation of hs-CRP and % body fat in our study was also observed by several studies[31,32] indicating low-grade inflammation pathology in increasing body fat. A significant positive correlation between hs-CRP and SBP and RHR may reflect in increased basal sympathetic tone in subjects with low-grade inflammation[24] as sympathetic stimulation directly influencing bone marrow activity resulting in increase in pro-inflammatory cells (increase inflammation) and decrease in vascular repair.[11]
On the other hand, significant positive correlation of IL-17 to DBP strengths the involvement of immune system and sympathetic drive of the body strengthens the existing evidence of cardiovascular damage caused by excessive stimulation of the sympathetic and reticular activating system and their receptors (α- and β-adrenergic and angiotensin II AT1 receptors) are mediated through a pro-inflammatory activation of the immune system.[33]
CONCLUSION
Elevated IL-17 levels are significant predictor of prehypertension along with lower sympathetic reactivity. Inflammatory marker hsCRP is raised is associated % BF in pre-hypertensive. Study fortifies the inflammation and immune mechanism in the pathogenesis of increased blood pressure in pre-hypertensive in addition to dampen sympathetic reactivity. However, further research on a bigger sample is required to establish linking of immune mechanism to sympathetic over drive in high blood pressure pathology.
Limitation
The study was conducted using only one test to assess the sympathetic reactivity which could result in variability in the response. Studies on a bigger sample size and with battery of test for sympathetic system activity are required to obtain more conclusive results.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Authors are grateful to HIMS, SRH University, for providing finance and logistics for conducting the study.
Conflicts of interest
There are no conflicts of interest.
References
- Interleukin-17 and interferon-gamma are produced concomitantly by human coronary artery-infiltrating T cells and act synergistically on vascular smooth muscle cells. Circulation. 2009;119:1424-32.
- [CrossRef] [PubMed] [Google Scholar]
- Interleukin 17 promotes angiotensin II-induced hypertension and vascular dysfunction. Hypertension. 2010;55:500-7.
- [CrossRef] [PubMed] [Google Scholar]
- Reduction of renal immune cell infiltration results in blood pressure control in genetically hypertensive rats. Am J Physiol Renal Physiol. 2002;282:F191-201.
- [CrossRef] [PubMed] [Google Scholar]
- Role of the T cell in the genesis of angiotensin II induced hypertension and vascular dysfunction. J Exp Med. 2007;204:2449-60.
- [CrossRef] [PubMed] [Google Scholar]
- Metabolic characteristics of prehypertension: Role of classification criteria and gender. J Hypertens. 2009;27:2394-402.
- [CrossRef] [PubMed] [Google Scholar]
- Autonomic neural regulation of the immune system: Implications for hypertension and cardiovascular disease. Hypertension. 2012;59:755-62.
- [CrossRef] [PubMed] [Google Scholar]
- Stress hormones, proinflammatory and antiinflammatory cytokines, and autoimmunity. Ann N Y Acad Sci. 2002;966:290-303.
- [CrossRef] [PubMed] [Google Scholar]
- Interleukin-17 causes Rho-kinase-mediated endothelial dysfunction and hypertension. Cardiovasc Res. 2013;97:696-704.
- [CrossRef] [PubMed] [Google Scholar]
- Elevated serum level of interleukin 17 in a population with prehypertension. J Clin Hypertens (Greenwich). 2015;17:770-4.
- [CrossRef] [PubMed] [Google Scholar]
- Autonomic-immune-vascular interaction: An emerging concept for neurogenic hypertension. Hypertension. 2011;57:1026-33.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of sympathovagal imbalance by spectral analysis of heart rate variability in prehypertensive and hypertensive patients in Indian population. Clin Exp Hypertens. 2011;33:478-83.
- [CrossRef] [PubMed] [Google Scholar]
- Autonomic function tests in prehypertensive young adult males of Uttarakhand region. Indian J Physiol Pharmacol. 2016;60:45-51.
- [Google Scholar]
- The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA. 2003;289:2560-72.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of adrenergic receptor blockade on the responses to isometric handgrip: Studies in normal and hypertensive subjects. J Cardiovasc Pharmacol. 1979;1:253-63.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular response of human subjects to isometric contraction of large and small muscle groups. Proc Soc Exp Biol Med. 1977;154:171-4.
- [CrossRef] [PubMed] [Google Scholar]
- Importance of primary capture and L-selectin-dependent secondary capture in leukocyte accumulation in inflammation and atherosclerosis in vivo. J Exp Med. 2001;194:205-18.
- [CrossRef] [PubMed] [Google Scholar]
- Vascular inflammation: A role in vascular disease in hypertension? Curr Opin Nephrol Hypertens. 2003;12:181-7.
- [CrossRef] [PubMed] [Google Scholar]
- Vascular inflammation in hypertension and diabetes: Molecular mechanisms and therapeutic interventions. Clin Sci (Lond). 2007;112:375-84.
- [CrossRef] [PubMed] [Google Scholar]
- Prehypertension-associated elevation in circulating lysophosphatidlycholines, Lp-PLA2 activity, and oxidative stress. PLoS One. 2014;9:e96735.
- [CrossRef] [PubMed] [Google Scholar]
- Early inflammatory and metabolic changes in association with AGTR1polymorphisms in prehypertensive subjects. Am J Hypertens. 2011;24:225-33.
- [CrossRef] [PubMed] [Google Scholar]
- Single-unit sympathetic discharge: Quantitative assessment in human hypertensive disease. Circulation. 1999;100:1305-10.
- [CrossRef] [PubMed] [Google Scholar]
- The sympathetic control of blood pressure. Nat Rev Neurosci. 2006;7:335-46.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular responses to an isometric handgrip exercise in females with prehypertension. N Am J Med Sci. 2016;8:243-9.
- [CrossRef] [PubMed] [Google Scholar]
- The study of cardiovascular sympathetic reactivity in prehypertensives with normal and higher BMI. Int J Res Med Sci. 2017;5:1033-8.
- [CrossRef] [Google Scholar]
- Heart rate as a predictor of development of sustained hypertension in subjects screened for stage 1 hypertension: The HARVEST study. J Hypertens. 2006;24:1873-80.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of intravenous propranolol on the systemic circulatory response to sustained handgrip. Am J Cardiol. 1966;18:333-44.
- [CrossRef] [Google Scholar]
- hs-CRP: A potential marker for hypertension in Kashmiri population. Indian J Clin Biochem. 2010;25:208-12.
- [CrossRef] [PubMed] [Google Scholar]
- hsCRP in prehypertension and hypertension: A prospective study in Southern Asian region. Int J Res Med Sci. 2014;2:1402-7.
- [CrossRef] [Google Scholar]
- Obesity indices and metabolic markers are related to hs-CRP and adiponectin levels in overweight and obese females. Obes Res Clin Pract. 2013;7:e315-20.
- [CrossRef] [PubMed] [Google Scholar]
- Central obesity as a major determinant of increased high-sensitivity C-reactive protein in metabolic syndrome. Int J Obes (Lond). 2005;29:1452-6.
- [CrossRef] [PubMed] [Google Scholar]
- Central and peripheral mechanisms of T-lymphocyte activation and vascular inflammation produced by angiotensin II-induced hypertension. Circ Res. 2010;107:263-70.
- [CrossRef] [PubMed] [Google Scholar]




