
Translate this page into:
Symmetrical drug-related intertriginous and flexural exanthem with itraconazole: The unusual reaction with a frequently used drug
*Corresponding author: Sheenu Goyal, Department of Dermatology, GGS, Faridkot, Punjab, India. sheenugoyal1997@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Goyal S, Kumar S, Brar B, Mehta A. Symmetrical drug-related intertriginous and flexural exanthem with itraconazole: The unusual reaction with a frequently used drug. Indian J Physiol Pharmacol. doi: 10.25259/IJPP_19_2024
Abstract
Symmetrical drug-related intertriginous and flexural exanthem (SDRIFE) is a rare, benign and self-limiting cutaneous adverse drug reaction. It presents as an erythematous rash distributed symmetrically on the gluteal and intertriginous areas with no systemic affection. SDRIFE is most commonly reported after exposure to antibiotics, particularly those in the penicillin group. Here, we present a case of SDRIFE associated with itraconazole. A 15-year-old boy presented with a dermatophytic infection for which itraconazole was prescribed. After 10 days of drug intake, he presented with diffuse erythema and scaling over the buttocks. The rash continued to progress to other intertriginous areas and was associated with itching and a burning sensation. On examination, an erythematous scaly macular rash symmetrically involving groins, thighs, neck, axilla, flexural aspect of arms, popliteal fossa and upper part of chest was noted. There was complete resolution of the lesions after 2 weeks of stopping itraconazole. The patient was, thus, diagnosed with SDRIFE due to itraconazole, based on the drug history and clinical profile. Although SDRIFE caused by itraconazole is exceedingly rare, increasing awareness among dermatologists can facilitate early identification and prompt discontinuation of the medication.
Keywords
Symmetrical drug-related intertriginous and flexural exanthem
Itraconazole
Awareness

INTRODUCTION
Symmetrical drug-related intertriginous and flexural exanthem (SDRIFE) is a rare, benign and self-limiting cutaneous adverse drug reaction. It presents as an erythematous rash distributed symmetrically on the gluteal and intertriginous areas with no systemic affection. It has most commonly been reported after exposure to antibiotics, particularly those in the penicillin and cephalosporin groups.[1] Among antifungals, it has been reported commonly with terbinafine. Recently, in India, dermatophytic infection has become an epidemic, and to tackle it, the use of itraconazole is on surge. We hereby report a case of SDRIFE with itraconazole.
CASE REPORT
A 15-year-old boy presented to our outpatient department of dermatology with a dermatophytic infection in his groins and buttocks, for which he was prescribed itraconazole 100 mg twice daily. After 10 days of drug intake, he presented with diffuse erythema and scaling over the buttocks only. The patient was initially misdiagnosed with contact dermatitis to topical antifungals and was prescribed topical steroids for a short duration, and itraconazole was continued. The patient reported again after 10 days with progression of rash to other intertriginous areas associated with itching and burning sensation. There was no history of any systemic symptoms.
On examination, an erythematous scaly macular rash symmetrically involving groins, thighs, neck, axilla, flexural aspect of arms, popliteal fossa and upper part of chest was noted [Figures 1 and 2]. Mucosae, palms and soles were spared.

- Erythematous scaly rash distributed symmetrically over chest, neck and arms.
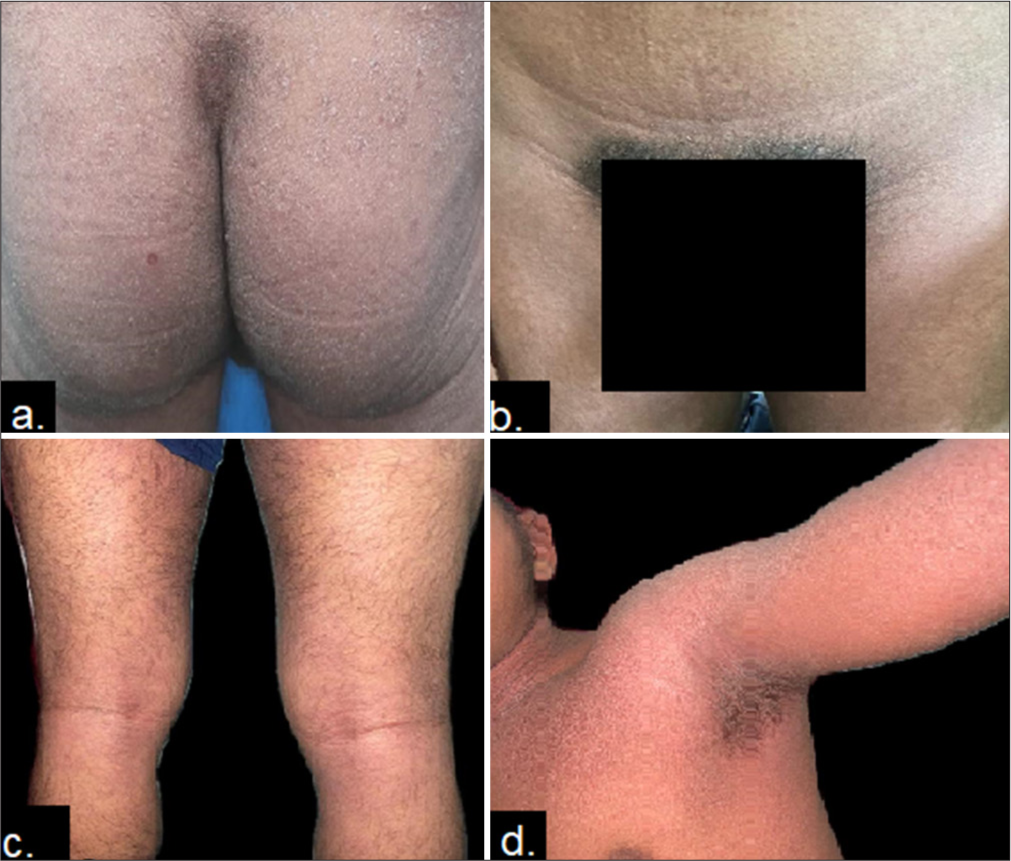
- Erythematous scaly rash involving (a) buttocks, (b) groins, (c) popliteal fossa and (d) axilla.
A skin biopsy was done, showing focal parakeratosis, hyperkeratosis, subcorneal pustule, papillary oedema and non-specific perivascular inflammatory infiltrate [Figure 3]. Other routine laboratory investigations were within normal limits. The patient was, thus, diagnosed with SDRIFE due to itraconazole, based on the drug history and clinical profile.
![Histopathology showing hyperkeratosis, papillary oedema and non-specific perivascular inflammatory infiltrate [Hematoxylin and eosin (H & E) stain, ×10].](/content/114/2025/0/1/img/IJPP-19-2024-g003.png)
- Histopathology showing hyperkeratosis, papillary oedema and non-specific perivascular inflammatory infiltrate [Hematoxylin and eosin (H & E) stain, ×10].
Itraconazole was discontinued, and the patient was prescribed a short course of oral steroids in tapering doses, antihistaminics and topical steroids. The lesions completely resolved within 3 weeks.
DISCUSSION
SDRIFE is a benign, self-limiting condition characterised by a symmetrical erythematous rash on the gluteal and intertriginous areas seen after exposure to systemic drugs. It is most commonly reported with beta-lactam antibiotics such as penicillin and cephalosporins. Other drugs include clindamycin, erythromycin, non-steroidal anti-inflammatory drugs, antihypertensives, radiocontrast agents and cimetidine.
The pathogenesis is suspected to be a type IV hypersensitivity reaction. Another hypothesis suggested that the increased concentration of eccrine glands in the intertriginous area leads to excess excretion of drugs in these areas.[2]
Differential diagnosis includes contact dermatitis, inverse psoriasis, intertrigo, tinea cruris, acute-generalised exanthematous pustulosis and Hailey-Hailey disease.
Oral provocation tests are positive in 80% of patients with SDRIFE, while patch tests are positive in up to 50% of patients. The histopathology of SDRIFE is non-specific, showing superficial mononuclear perivascular infiltrate, subcorneal pustules, vacuolar changes and spongiosis.
The diagnosis of SDRIFE primarily relies on the history and clinical picture. Treatment is symptomatic, such as antihistamines, emollients, and offending drugs should be withdrawn. A short course of oral steroids hastens the recovery.
In our case, the patient was diagnosed with SDRIFE due to itraconazole, and the resolution of symptoms occurred after withdrawing the drug. Although SDRIFE caused by itraconazole is exceedingly rare, increasing awareness among dermatologists can facilitate early identification and prompt discontinuation of the medication. SDRIFE due to antifungal terbinafine has already been reported in the literature, but now rising trends are being seen with itraconazole also, especially in developing countries.[3] Recently, SDRIFE due to itraconazole has been added to the monthly drug safety alert (May 2022) in Indian Pharmacopoeia to wary physicians.
CONCLUSION
This case highlights the importance of recognizing SDRIFE as a rare but noteworthy adverse reaction to itraconazole. Although SDRIFE is benign, awareness among clinicians can facilitate timely diagnosis, avoiding mismanagement and unnecessary continuation of the causative drug. With itraconazole now being associated with SDRIFE and included in drug safety alerts, it is essential for healthcare professionals to remain vigilant and consider this diagnosis in patients presenting with symmetric intertriginous rashes after systemic drug exposure.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Symmetrical drug-related intertriginous and flexural exanthema In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK539750 [Last accessed on 2022 Oct 03]
- [Google Scholar]
- Symmetrical drug related intertriginous and flexural exanthema (SDRIFE) induced by fluconazole: An uncommon side effect of a commonly used drug. Dermatol Ther. 2019;32:e13130.
- [CrossRef] [Google Scholar]
- Rising trends of symmetrical drug related intertriginous and flexural exanthem due to Itraconazole in patients with superficial dermatophytosis: A case series of 12 patients from eastern part of India. Dermatol Ther. 2020;33:e13911.
- [CrossRef] [Google Scholar]




