
Translate this page into:
Weight gain during pregnancy and its impact on maternal autonomic modulations and birth outcomes
*Corresponding author: Sucharita Sambashivaiah, Department of Physiology, St Johns Medical College, Bengaluru, Karnataka, India. sucharita@stjohns.in
-
Received: ,
Accepted: ,
How to cite this article: Sharma S, Thomas T, Sambashivaiah S. Weight gain during pregnancy and its impact on maternal autonomic modulations and birth outcomes. Indian J Physiol Pharmacol. 2024;68:208-15. doi: 10.25259/IJPP_21_2023
Abstract
Objectives:
The study aimed to compare the heart rate variability (HRV) indices, a measure of cardiac autonomic modulation, and birth outcomes in mothers with below-adequate and adequate gestational weight gain.
Materials and Methods:
Eighty mothers (with low to normal body mass index [BMI]) were recruited in their first trimester. Fifty-one mothers were followed up throughout pregnancy. Maternal electrocardiogram (ECG) and anthropometry were collected at each trimester. Power spectral analysis was performed on ECG, and HRV indices were derived. Birth outcomes and anthropometric data were collected at birth. Participants were classified based on the Institute of Medicine (IOM) recommendations for weight gain into below adequate weight gain (BWG) group and adequate weight gain (AWG) group (cutoff of 12.5 kg for low BMI mothers and 11.5 kg for normal BMI mothers).
Results:
Mean weight gain during pregnancy was 9.6 ± 3.4 kg. Delta low frequency (LF), a marker of cardiac sympathetic activity (difference between the 1st and 3rd trimester), was lower (P < 0.05) among the BWG group (−377.5 ± 686 ms2) compared to the AWG group (−741.1 ± 581 ms2). Spearman’s correlation demonstrated a positive association between delta LF and birth weight (r = 0.34, P < 0.05) in the BWG.
Conclusion:
Irrespective of BMI status, mothers gained lower weight than the (revised) IOM recommendations. BWG had decreased sympathetic modulations during pregnancy. Birth weight was positively correlated with greater sympathetic modulations even among women in BWG, thus highlighting the need to monitor autonomic modulations, along with weight gain during pregnancy effectively.
Keywords
Pregnancy
Sympathetic modulation
Gestational weight gain
Birth outcomes

INTRODUCTION
India is home to one-fifth of the world’s birth rate. According to the UNICEF-World Health Organization (WHO) 2019 report,[1] even among the economically privileged groups, rates of low birth weight are among the highest in India. Maternal nutrition is an essential factor in determining birth outcomes.[2] Approximately 40% of rural women and 25% of urban women are undernourished.[3] Maternal nutrition status is mainly determined by pre-pregnancy body mass index (BMI) and weight gain during pregnancy.[4] Adequate nutrition is required not only for the healthy growth of the foetus but also for maternal health during pregnancy and beyond. The adverse consequences of underweight status during the beginning of pregnancy on birth outcomes and childhood developmental delay are well established.[5,6] However, there is little evidence to understand the changes in gestational weight gain on birth outcomes, especially among women with low to normal pre-pregnancy BMI. The Institute of Medicine, as per revised guidelines, recommends higher gestational weight gain for women with a pre-pregnancy BMI of <18.5 kg/m2 to deliver infants with the same birth weight as women with normal BMI.[7] Recent evidence from low- and middle-income countries, including India, suggests that irrespective of their nutritional status, women do not meet the recommended weight gain during pregnancy.[8,9] Thus, the results from these studies raise the question of the applicability of IOM recommendations for adequate weight gain suitable for high-income and low- and middle-income countries. Gestational weight gain results from adaptations that meet pregnancy requirements, such as increased blood volume, placenta and foetus growth, amniotic fluid growth and uterus and breast growth.[10-12] One of the critical regulators of adaptations (enlisted above) during pregnancy includes the modulation of the autonomic nervous system.[13] Heart rate variability (HRV) is a noninvasive technique to measure autonomic activity. Studies have shown decreased HRV during pregnancy compared to normal women in cross-sectional studies.[14,15] Insufficient adaptation of the autonomic nervous system as gestation advances has been linked with several complications not only during pregnancy but also in the foetus.[16,17] Obstetrical complications such as gestational diabetes and pre-eclampsia have been linked with maladaptation in autonomic nervous activity.[18,19] Increased sympathetic activity was seen in mothers with pre-eclampsia using HRV analysis.[20] Birth weight has been associated with dysfunctional maternal autonomic regulation.[21] Hence, complications during pregnancy can lead to increased perinatal morbidity and mortality. Early detection of autonomic maladaptation can help prevent the development and progression of such perinatal complications. Due to the association between pregnancy complications and autonomic dysfunction, tracking autonomic changes throughout pregnancy may allow for detecting maternal health deterioration. However, limited longitudinal studies exist to understand the autonomic modulations during normal pregnancy.[22,23] Furthermore, there is a lack of data to understand the impact of weight gain on maternal health, especially autonomic modulation and birth outcomes. Studies suggest that excessive weight gain during pregnancy is associated with obstetrical complications such as gestational hypertension, gestational diabetes and delivery by caesarean section.[24] Therefore, the study aimed to (i) understand the weight gain and HRV patterns in low to average BMI mothers during pregnancy and (ii) compare HRV indices and birth outcomes between below-adequate weight gain and adequate weight gain in Indian mothers.
MATERIALS AND METHODS
Out of 125 mothers <14 weeks (first trimester) with low to normal BMI registered for the antenatal screening at the obstetrics and gynaecology outpatient department, 80 mothers were recruited after obtaining written informed consent. Women with BMI <25 kg/m2 with singleton pregnancy and willing to undergo follow-up for the duration of pregnancy were included in the study. Women were screened for chronic illnesses such as diabetes mellitus (both type 1 and 2), hypertension, heart disease, thyroid disease, hepatitis B and human immunodeficiency virus. Mothers were also screened for any symptoms of autonomic or peripheral neuropathy. Following a loss to follow-up, 51 mothers completed the study. Electrocardiograms (ECGs) for maternal HRV analysis and anthropometric parameters were collected during the first, second and third trimesters. Following delivery, details regarding the mode of delivery and anthropometric parameters such as birth weight, length and head circumference were collected. The Institutional Ethics Committee approved the research protocol, and all the study details were collected following the Helsinki Declaration.
Descriptive and anthropometric data
The gestational age was calculated as days from the 1st day of the last menstrual period reported. Anthropometric parameters, including weight and height, were recorded in each trimester. Weight was recorded using a calibrated digital scale. Using a vertically mobile scale, height was recorded to the nearest 0.1 cm; using a standard equation, the BMI was calculated as weight (kg)/height2 (m2). BMI of <18.5 kg/m2 was categorised as low BMI mothers. BMI between 18.5 and <25 kg/m2 was categorised as normal BMI.
HRV assessment
An abdominal maternal ECG (Monica DK ™, UK) was recorded for each subject. The procedure is described in detail previously. Subjects were asked to relax for 30 min, after which the ECG was recorded in a quiet room for 10 min. Five disposable electrodes (Ambu ™ blue sensor, Copenhagen, Denmark) were attached to the abdomen. Each electrode was placed in the four quadrants of the abdomen, and the reference electrode was placed in the upper part of the abdomen on the right side. RR intervals (distance between the peaks of 2 R waves in ECG) were extracted from the data acquisition system, and the tachogram was plotted. HRV analysis was performed on the recorded data (Lab Chart 7 Pro, AD Instruments™, Australia). The frequency-domain method was used to perform HRV analysis. Power spectral density (PSD) analysis was performed using the Fast Fourier transform algorithm. Different frequency bands were calculated based on power and peak frequencies derived from the PSD. In a given segment, up to 3 data points were edited. Power was calculated in three bands as per recommended guidelines. The low-frequency (LF) band, a reflection of sympathetic responses of the heart, was calculated using the 0.04–0.15 Hz band. The 0.15–0.4 Hz band is referred to as a high-frequency (HF) band. This band represents parasympathetic activity in the heart. The total variance of the power spectral density is defined by absolute total power (TP [0–0.4]).[25,26]
Statistical methods
The study variables were tested using Kolmogorov–Smirnov test for normality. HRV indices were not normally distributed during the three trimesters of pregnancy. The data were Log-transformed and used for further analysis. The mean (standard deviation) or percentage (%) was used to represent the data. Delta weight gain was computed by subtracting weight (kg) in the 1st trimester from weight (kg) in the 3rd trimester. Similarly, delta changes in HRV were calculated as the difference of each of the indices between the 1st and 3rd trimesters. Mothers were classified into two groups: Below below-adequate weight gain (BWG) group and the adequate weight gain (AWG) group based on the lower limit of normal IOM recommended weight gain guidelines (cut off of 12.5 kg for low BMI mothers and 11.5 kg for normal BMI mothers). Delta HRV indices and birth outcomes between the weight gain groups were analysed using the Mann–Whitney U-test. Comparison of the HRV indices among the BWG and AWG groups during three trimesters of pregnancy was done using repeated measures analysis of variance. Pearson’s correlation test was performed to study the association between variables. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) (v20, SPSS, Chicago, IL, USA). If P < 0.05, the results were considered significant.
RESULTS
The mean age of the study participants was 24.3 ± 3.0 years. The gestational age at data collection at each trimester is as follows: I trimester (74.9 ± 24.3 days), II trimester (163.17 ± 17.5 days) and III trimester (249.13 ± 14.6 days). The mean BMI during 1st trimester was 20.2 ± 2.5 kg/m2, and the total mean weight gain during pregnancy was 9.6 ± 3.4 kg. About 62% of the study participants were primiparous. Below higher secondary school education level was reported by 28 women, and 19 mothers reported as being employed. Table 1 presents the descriptive characteristics of the study participants. About 29.5% of the participants belonged to the low BMI category during the trimester of the pregnancy.
| Maternal characteristics | AWG (n=16) | BWG (n=35) |
|---|---|---|
| Age at baseline (y) | 23.4±2.9 | 24.5±2.8 |
| Gestational age at baseline (days) | 77.7±21.3 | 78.8±25.9 |
| Heart rate (bpm) | 80.8±9.6 | 79.7±13.2 |
| Systolic blood pressure at baseline (mmHg) | 109.9±6.2 | 109.8±9.1 |
| Diastolic blood pressure at baseline (mmHg) | 69.1±5.5 | 72.7±7.7 |
| Weight at baseline (kg) | 49.2±7.0 | 47.5±4.4 |
| Height (m) | 1.58±7.8 | 1.54±4.6 |
| BMI at baseline (kg/m2) | 19.7±1.7 | 19.9±1.7 |
| BMI <18.5 kg/m2(%) | 20 | 74 |
| BMI ≥18.5 kg/m2(%) | 31 | 67 |
| Gestational weight gain (kg) | 14.0±2.4 | 8.0±1.8 |
| New born indicators (n=51) | ||
| Birth weight (kg) | 3.0±0.3 | 2.7±0.3 |
| Female (%) | 50 | 60 |
| Birth length (cm) | 52.4±0.2 | 49.8±0.6 |
| Head circumference (cm) | 34.0±0.4 | 34.2±0.2 |
| LBW (%) | 25 | 29 |
BMI: Body mass index, LBW: Low birth weight, BWG: Below adequate weight gain, AWG: Adequate weight gain
Mothers with low and normal BMI had comparable total weight gains of 9.4 ± 4.1 and 9.8 ± 3.2 kg, respectively. This was below the recommended weight gain for pregnancy in both groups. It was noted that 20% of the mothers with low BMI and 31% of mothers with normal BMI achieved the recommended weight gain during pregnancy [Figure 1]. Overall, when low and average-BMI mothers were combined, 67% gained weight less than the IOM recommendation during pregnancy.
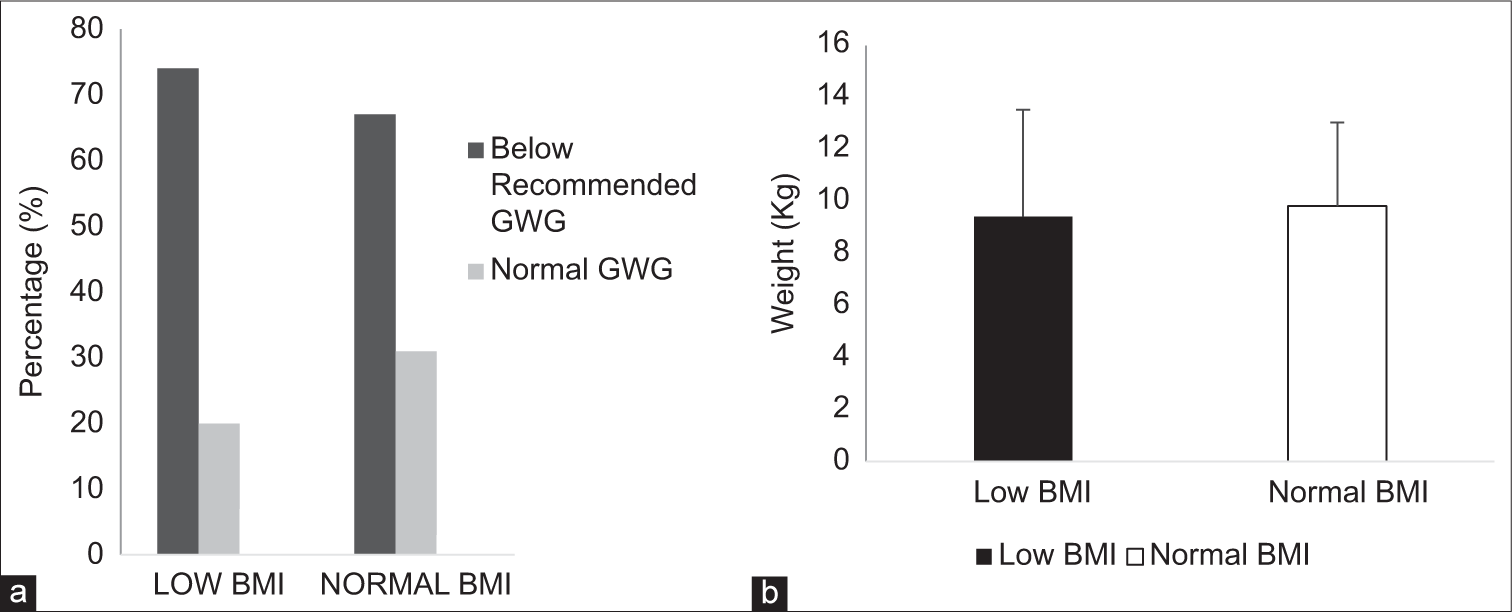
- Gestational weight gain (GWG) patterns in low and normal body mass index (BMI) mothers. (a) Percentage of study subjects under each category of GWG. (b) Comparison of delta weight gain in low BMI and normal BMI group. Category of GWG was based on Institute of Medicine (IOM) recommendations in low BMI and normal BMI.
Figure 2 summarises the changes in HRV indices during each trimester of pregnancy in the study groups. A significant change (P < 0.05) was seen in the HRV indices, namely, Log LF, Log HF, Log TP and LF/HF, in the 2nd and 3rd trimesters compared to the 1st trimester. There was no significant difference in HRV indices between the BWG and AGW groups. However, there was a significant interaction effect of groups over time (P = 0.04) for log LF.
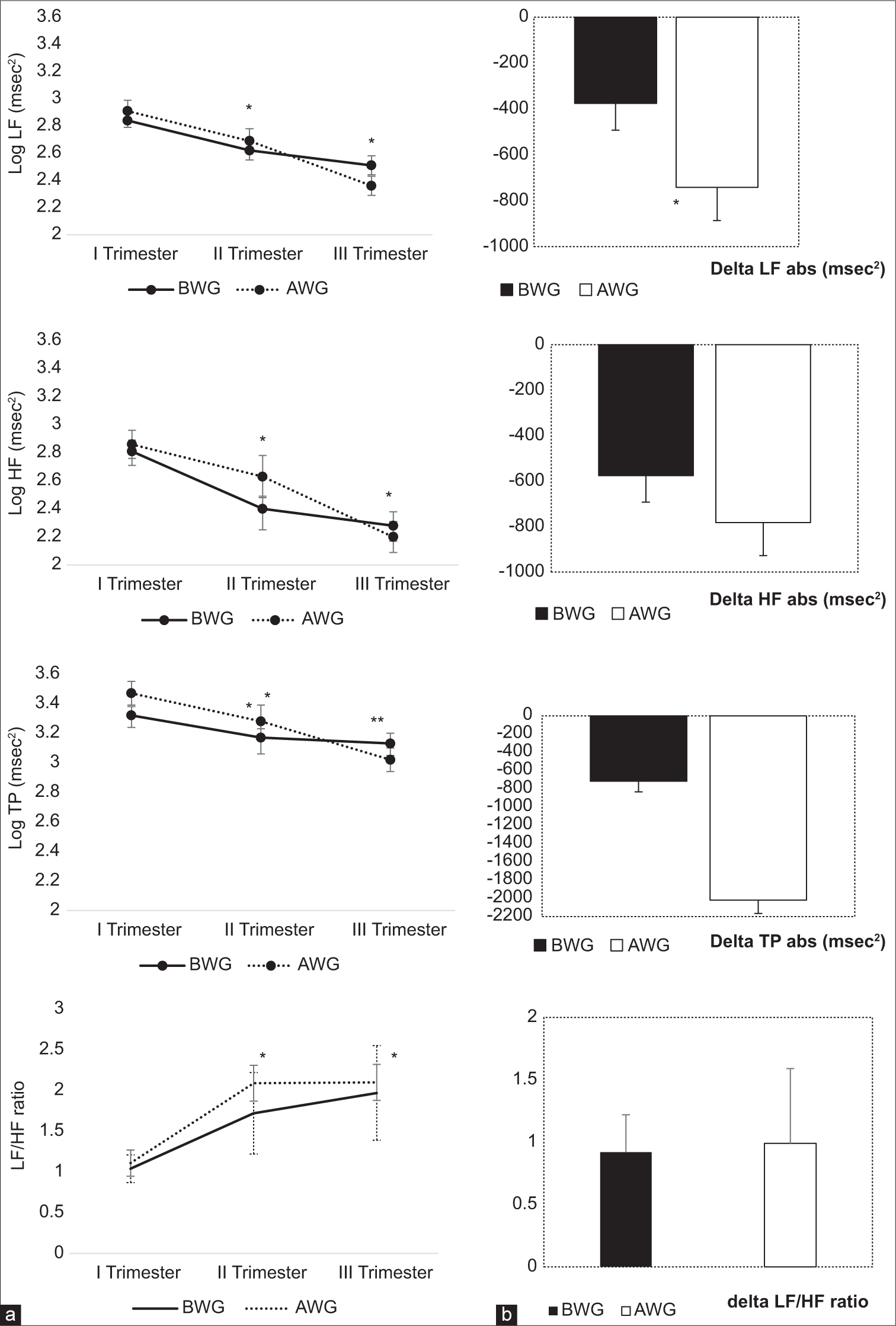
- Pattern of changes in HRV indices during three trimesters of pregnancy in BWG and AWG group. HRV: Heart rate variability, BWG: Below adequate weight gain, AWG: Adequate weight gain. (a) *P < 0.05 on comparison of 1st Trimester values with 2nd and 3rd trimester. HRV indices were log-transformed to achieve normality. (b) *P < 0.05 on comparison of delta HRV indices (absolute units) between AWG and BWG groups. LF: Low Frequency, HF: High Frequency, TP: Total Power, LF/HF: Low Frequency/High Frequency ratio. Data are represented as Mean±Standard error of the mean.
On comparing the delta HRV indices, it was seen that delta LF absolute units (ms2) were significantly lower (P < 0.05) among the BWG group (−377.5 ms2 ± 686) compared to the AWG group (−741.1 ms2 ± 581). The rest of the delta HRV indices were comparable between the two groups. There was no significant association between delta weight gain and any of the delta HRV indices.
Of the 51 newborns, 14 had low birth weight (21%). Three low-birth infants (<2.5 kg) were born to women in the low BMI group. There was no association between birth weight and maternal BMI. Out of the 14 low-birth-weight infants, 10 (71%) were born to mothers with BWG during pregnancy. The mean birth weight in the BWG group (2.67 kg ±0.3) was significantly lower (P < 0.05) compared to the AWG group (2.97 kg ±0.3). There was a significant and positive association between delta LF and birth weight (r = 0.33, P = 0.02) [Figure 3]. There was no association between birth weight and delta HF and delta total power in the overall sample. When the correlation between birth weight and delta LF was examined separately in the BWG and AWG, there was a significant and positive association between delta LF and birth weight (r = 0.34, P = 0.05) in the BWG group alone. There was no association between delta LF and birth weight in the average weight gain group (r = 012, P = 0.7).
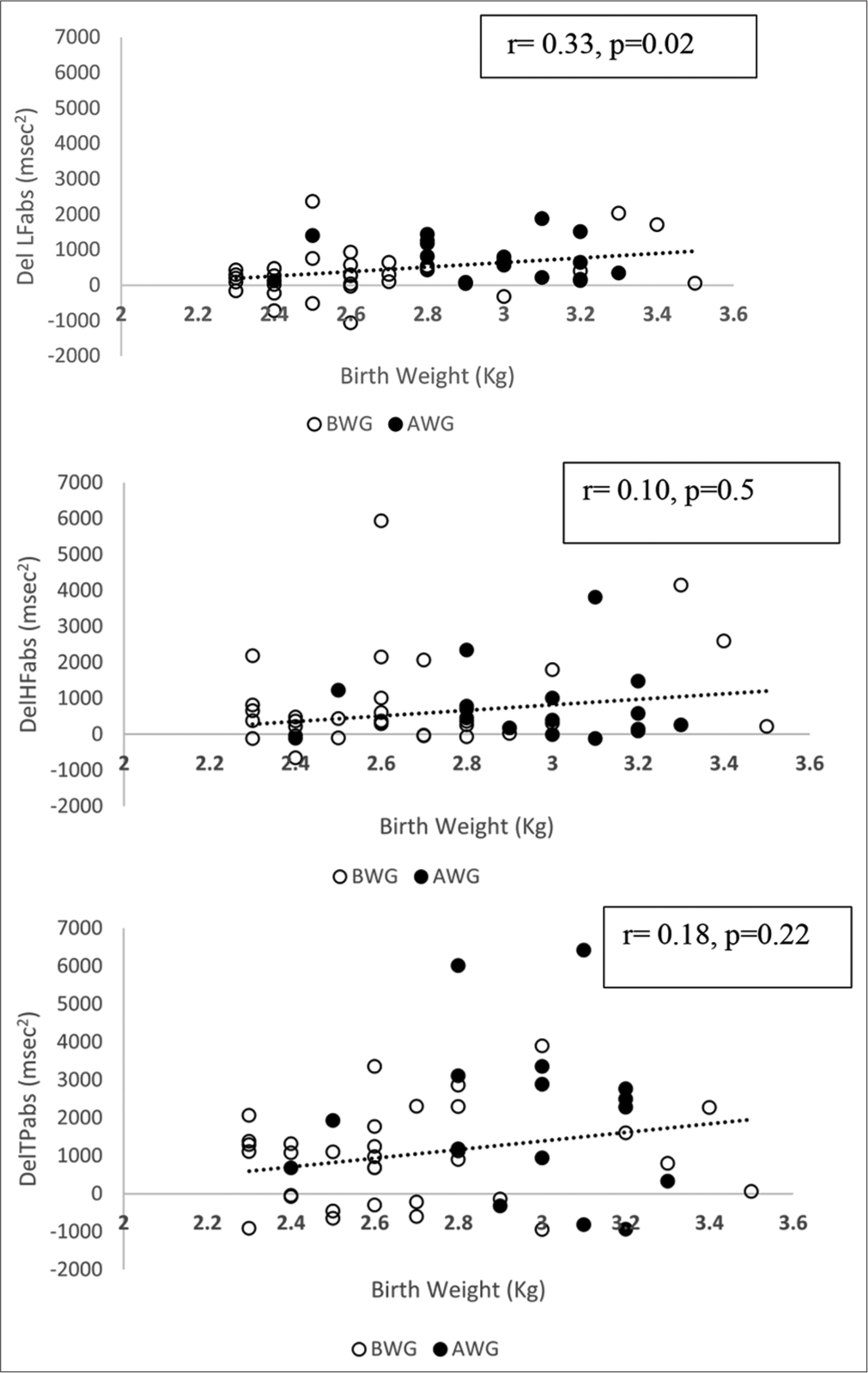
- Scatter plot representing the association between delta low heart rate variability indices with birth weight. The correlation coefficient, P values are for whole group. P < 0.05. BWG: Below adequate weight gain, AWG: Adequate weight gain.
DISCUSSION
The pattern of HRV indices during longitudinal follow-up of pregnancy
Findings from the present study showed that LF, which measures cardiac sympathetic activity, and HF, predominantly a measure of cardiac parasympathetic activity, were significantly lower during longitudinal follow-up of pregnancy. Further, when mothers were grouped based on total weight gain during pregnancy, the delta change in the LF HRV index, a measure of total sympathetic modulations during pregnancy, was significantly lower in mothers who did not gain the recommended weight.
Most evidence to understand changes in autonomic regulation during healthy pregnancy comes from cross-sectional studies where HRV indices were compared between groups of women in each trimester. Cross-sectional studies have shown that all the HRV indices decrease in the second and third trimesters compared to the first trimester.[27] Rapid hemodynamic changes have been associated with pregnancy, which begins with conception and reaches a peak at midgestation.[28] There is also an alteration in levels of various pressor hormones and vasoactive metabolites during pregnancy, which can result in a fall in systemic vascular tone and blood volume expansion.[29] Low resistance circulation is also seen in the gravid uterus.[30] These factors can decrease HRV indices in the second trimester compared to the first trimester, as seen in this study. During the second half of pregnancy, autonomic modulations can be brought about by aortocaval compression from the enlarging gravid uterus.[31] Any deviation in this autonomic adaptation can result in dysautonomia during pregnancy and suggest incomplete adaptation of the cardiovascular system to handle pregnancy-related changes resulting in complications. For example, sympathetic overactivity during later parts of pregnancy is known to result in gestational hypertension, gestational diabetes, perinatal complications and also adverse effects on the foetus.[32-34] Similarly, orthostatic dysregulation during pregnancy is also associated with spontaneous abortions, low-birth-weight infants and stillbirths.[35,36]
Gestational weight gain patterns among low and normal BMI women
On analysis of gestational weight gain patterns among study subjects, only 20% of low BMI women and 31% of normal-weight women achieved recommended weight gain as per IOM guidelines. Adequate maternal nutrition plays a crucial role in determining birth outcomes by ensuring the average growth and development of the foetus. Thus, to improve infant birth weight, IOM (Institute of Medicine, USA) has established guidelines for adequate weight gain during pregnancy. Based on WHO BMI cutoffs, these guidelines are currently being revised. Accordingly, gestational weight gain recommendations for underweight are 12.5–18 kg, normal-weight women are 11.5–16 kg, and overweight women are 7–11.5 kg, whereas obese women are recommended to achieve only 5–9 kg of weight throughout pregnancy.[7] However, it is unclear if the guidelines apply to developing countries as the BMI classification for Asians is different. Like a few studies from India and other parts of Asia.[8,37] Data from this study also showed that nearly 70% of women in both underweight and normal weight categories did not achieve the recommended weight gain.
Autonomic modulations and gestational weight gain
The results from the present study demonstrated significantly lower birth weight and lower modulations in cardiac sympathetic activity in the low gestational weight gain group compared to normal gestational weight gain women. Adverse pregnancy outcomes such as spontaneous abortion, preterm birth, foetal growth restrictions and low birth weight have been linked to inadequate gestational weight gain.[38,39] Present results demonstrate that irrespective of pre-pregnancy BMI status, there was a significant positive correlation between gestational weight gain and birth weight of the newborns. Nearly 71% of low-birth-weight infants were born to women with low gestational weight gain. Lower autonomic modulations suggest dysregulation in autonomic adaptation in women with lower gestational weight gain. Any altered maternal cardiovascular autonomic control could result in abnormal uterine perfusion and placental development. A decrease in normal pregnancy-induced adaptations could result in foetal growth restriction or low birth weight. The study analysis showed a positive correlation between delta LF and birth weight in the low weight gain group, suggesting better birth outcomes with greater variability in HRV indices even among women with low gestational weight gain.
The findings from this study are essential as there is evidence linking lifestyle intervention programs in optimising gestation weight gain and improving pregnancy outcomes, even though mechanisms are unclear. Intervention techniques such as yoga, physical activity and relaxation methods are known to improve autonomic adaptations during pregnancy.[40,41] Further, practising these interventions has independently shown improvements in the outcomes of pregnancy and childbirth.[42] The findings from the study provide a link between autonomic adaptations and birth outcomes. This is useful as changes, if detected early, are known to be reversible. Thus, continuous monitoring using simple techniques can help us plan interventions effectively.
One of the limitations of the present study was that subjects did not undergo any interventions as part of the study. Understanding changes in autonomic modulations before and after interventions could have helped better understand the mechanisms. Furthermore, a larger sample size with a wide pre-pregnancy BMI range could have helped better understand the gestational weight gain patterns and birth outcomes. However, the study’s main strength was the longitudinal follow-up of each subject throughout pregnancy. Thus, the autonomic modulations and weight gain patterns were accurately recorded from I trimester to birth. Furthermore, the HRV technique for capturing autonomic modulations is a sensitive biomarker and a simple tool that primary care physicians or caregivers can use.
CONCLUSION
This study adds to evidence that Indian women, irrespective of their pre-pregnancy BMI status, gain lower weight than the revised IOM recommendations. Below-adequate weight gain is associated with adverse pregnancy outcomes. Even among women with below-adequate weight gain, there is a correlation between the modulations in HRV indices, specifically sympathetic activity and birth weight. This emphasises the need for continuous adequate primary care during pregnancy to acquire recommended gestational weight gain to reduce maternal and foetal complications.
Ethical approval
The research/study was approved by the Institutional Review Board at St. John’s Medical College, number IEC Ref No 136/2013, dated 12 September 2013.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
The study was partially funded by the St Johns Medical College Research Society, RS/1/1164/13.
References
- Low birthweight estimates: Levels and trends 2000-2015 Geneva: World Health Organization; 2019.
- [Google Scholar]
- Opportunities for improving maternal nutrition and birth outcomes: Synthesis of country experiences. Food Nutr Bull. 2012;33:S104-37.
- [CrossRef] [Google Scholar]
- Determinants of low birth weight in India: An investigation from the National Family Health Survey. Am J Hum Biol. 2020;32:e23355.
- [CrossRef] [Google Scholar]
- Poor maternal nutritional status before and during pregnancy is associated with suspected child developmental delay in 2-year old Brazilian children. Sci Rep. 2020;10:1851.
- [CrossRef] [Google Scholar]
- Maternal body mass index and risk of neonatal adverse outcomes in China: A systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019;19:105.
- [CrossRef] [Google Scholar]
- Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines In: Rasmussen KM, Yaktine AL, eds. Weight Gain During Pregnancy: Reexamining the Guidelines. Washington, DC: National Academies Press; 2009.
- [Google Scholar]
- Gestational weight gain and pregnancy outcomes in relation to body mass index in Asian Indian Women. Indian J Endocrinol Metab. 2017;21:588-93.
- [CrossRef] [Google Scholar]
- Gestational weight gain in low-income and middle-income countries: A modelling analysis using nationally representative data. BMJ Glob Health. 2020;5:e003423.
- [CrossRef] [Google Scholar]
- Nutritional support in obstetrics and gynecology. Clin Obstet Gynecol. 1976;19:489-513.
- [CrossRef] [Google Scholar]
- Nutrition and metabolism in pregnancy: Mother and fetus New York: Oxford University Press; 1990.
- [Google Scholar]
- Autonomic cardiovascular reflexes in pregnancy. A longitudinal study. Clin Auton Res. 1994;4:161-5.
- [CrossRef] [Google Scholar]
- Heart rate variability is reduced in normal pregnancy irrespective of trimester: A cross-sectional study from Gujarat, India. J Family Med Prim Care. 2020;9:626-31.
- [CrossRef] [Google Scholar]
- A study on cardiac autonomic modulation during pregnancy by non-invasive heart rate variability measurement. Int J Med Public Health. 2014;4:441-5.
- [CrossRef] [Google Scholar]
- Heart rate variability in normal and complicated pregnancies. Fiziol Cheloveka. 2008;34:97-105.
- [CrossRef] [Google Scholar]
- Heart rate variability and pregnancy complications: Systematic review. Interact J Med Res. 2023;12:e44430.
- [CrossRef] [Google Scholar]
- Autonomic modulation in gestational diabetes mellitus. J Diabetes Complications. 2014;28:684-8.
- [CrossRef] [Google Scholar]
- Heart rate variability and autonomic modulations in preeclampsia. PLoS One. 2016;11:e0152704.
- [CrossRef] [Google Scholar]
- Preeclamptic pregnancy is associated with increased sympathetic and decreased parasympathetic control of HR. Am J Physiol Heart Circ Physiol. 2000;278:H1269-73.
- [CrossRef] [Google Scholar]
- Investigating the association of maternal heart rate variability with fetal birth weight. Annu Int Conf IEEE Eng Med Biol Soc. 2023;2023:1-4.
- [CrossRef] [Google Scholar]
- Trends in heart rate and heart rate variability during pregnancy and the 3-month postpartum period: Continuous monitoring in a free-living context. JMIR Mhealth Uhealth. 2022;10:e33458.
- [CrossRef] [Google Scholar]
- Longitudinally tracking maternal autonomic modulation during normal pregnancy with comprehensive heart rate variability analyses. Front Physiol. 2022;13:874684.
- [CrossRef] [Google Scholar]
- Association of gestational weight gain with adverse maternal and infant outcomes. JAMA. 2019;321:1702-15.
- [CrossRef] [Google Scholar]
- Role of editing of R-R intervals in the analysis of heart rate variability. Front Physiol. 2012;3:148.
- [CrossRef] [Google Scholar]
- Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation. 1996;93:1043-65.
- [Google Scholar]
- Baroreflex sensitivity, heart rate, and blood pressure variability in normal pregnancy. Am J Hypertens. 2000;13:1218-25.
- [CrossRef] [Google Scholar]
- Cardiac output and related haemodynamics during pregnancy: A series of meta-analyses. Heart. 2016;102:518-26.
- [CrossRef] [Google Scholar]
- Uteroplacental blood flow. The story of decidualization, menstruation and trophoblast invasion. Am J Pathol. 2000;157:1759-68.
- [CrossRef] [Google Scholar]
- Biphasic changes in autonomic nervous activity during pregnancy. Br J Anaesth. 2000;84:323-9.
- [CrossRef] [Google Scholar]
- Preeclampsia--a state of sympathetic overactivity. N Engl J Med. 1996;335:1480-5.
- [CrossRef] [Google Scholar]
- Sympathetic nervous system activity and reactivity in women with gestational diabetes mellitus. Physiol Rep. 2020;8:e14504.
- [CrossRef] [Google Scholar]
- Effects of psychological stress on adverse pregnancy outcomes and nonpharmacologic approaches for reduction: an expert review. Am J Obstet Gynecol MFM. 2020;2:100229.
- [CrossRef] [Google Scholar]
- Effects of low maternal heart rate on fetal growth and birthweight. Int J Gynaecol Obstet. 2019;146:250-6.
- [CrossRef] [Google Scholar]
- Autonomic cardiovascular control in pregnancies with abnormal uterine perfusion. Am J Hypertens. 2006;19:306-12.
- [CrossRef] [Google Scholar]
- Guidelines for obstetrical practice in Japan: Japan Society of Obstetrics and Gynecology (JSOG) and Japan Association of Obstetricians and Gynecologists (JAOG) J Obstet Gynaecol Res. 2014;40:1469-99.
- [CrossRef] [Google Scholar]
- Association between gestational weight gain and severe adverse birth outcomes in Washington State, US: A population-based retrospective cohort study, 2004-2013. PLoS Med. 2019;16:e1003009.
- [CrossRef] [Google Scholar]
- Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis. JAMA. 2017;317:2207-25.
- [CrossRef] [Google Scholar]
- Effect of integrated yoga on stress and heart rate variability in pregnant women. Int J Gynaecol Obstet. 2009;104:218-22.
- [CrossRef] [Google Scholar]
- The influence of physical activity during pregnancy on maternal, fetal or infant heart rate variability: A systematic review. BMC Pregnancy Childbirth. 2016;16:326.
- [CrossRef] [Google Scholar]
- The effect of yoga on the delivery and neonatal outcomes in nulliparous pregnant women in Iran: A clinical trial study. BMC Pregnancy Childbirth. 2021;21:351.
- [CrossRef] [Google Scholar]




