
Translate this page into:
A systematic review of the association between lead levels in hair and urine in children with attention deficit hyperactivity disorder (ADHD)

*Corresponding author: Suchanda Sahu, Department of Biochemistry, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India. biochem_suchanda@aiimsbhubaneswar.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Sahu S, John J, Nayak S. A systematic review of the association between lead levels in hair and urine in children with attention deficit hyperactivity disorder (ADHD). Indian J Physiol Pharmacol. 2023;67:239-44. doi:10.25259/IJPP_18_2023
Abstract
Attention deficit hyperactivity disorder (ADHD), characterised by inattentiveness, hyperkinetic behaviour, and impulsivity in childhood, leads to decreased academic performance and learning in general. Among the environmental factors, lead (Pb) in the environment is considered a crucial public health issue associated with ADHD. This study assessed the existing literature for the association of hair and urine lead levels with ADHD. The studies included in this systematic review were case-control observational and prevalence studies of a place or population. For hair Pb levels, out of 478 participants, 89 were ADHD cases and 389 controls showed a pooled effect of a standardised mean difference of 0.30 (0.03–0.57). The overall effect Z was 2.16, which was statistically significant (P = 0.03). For urine Pb levels, there were 196 ADHD cases and 423 healthy controls. The pooled effect of the standardised mean difference was 0.34 (0.13–0.56). The overall effect Z was 3.12, which was statistically significant (P = 0.002). Pb estimations can reduce the disease burden of ADHD by non-invasive methods such as in hair and urine, which have better acceptance by parents.
Keywords
Attention deficit
Hyperactivity
Lead
Estimation
Hair
Urine

INTRODUCTION
Attention deficit hyperactivity disorder (ADHD) is a behavioural disorder that appears in childhood. It is characterised by inattentiveness, hyperkinetic behaviour, and impulsivity. Although this is not an illness and much progress has been made in the etiopathogenesis and management modes, it still draws attention to its prevention. There is poor compliance to treatment and resistance to long-term use of medications. For the same reasons, these children have decreased academic performance and learning in general. Usually, ADHD children have compromised social, behavioural, vocational, and occupational functioning.[1] Several genetic risks and environmental factors have been identified as causal effects of ADHD. Among the environmental factors, lead in the surrounding is considered a crucial public health issue, especially in children due to their hand using norms, and exposure to outdoor dust and paints in houses and toys. The same amount of lead exposure in adults is not as harmful as it is in children.[2]
Lead can enter the body through various sources such as air, food, water, dust, and soil. Its half-life in the blood is about 1–2 months.[3] Lead that is not absorbed by red blood cells is dispersed throughout the body’s soft tissues and eventually accumulates in bone. Lead deposited in bone has a long half-life of between 20 and 30 years. Lead is eliminated in the urine and bile and its clearance from the body is very slow. During pregnancy, there is an increased mobilisation of lead from bones and its passage to the foetus through the placenta causes grave neurotoxicity during the developmental stages.[4]
Although the centres for disease control and prevention currently use blood lead levels (BLLs) of 3.5 μg/dL as the normal reference range, it has been reported that there is a decline in intellect and an increase in behavioural and learning difficulties in children even at lower BLL. Hence, there is no safe level of lead exposure in children.[5,6] As BLL shows recent lead exposure and the same correlates well with the urine levels, we projected the long-term cumulative effect of lead in hair with ADHD. Thus, this study was planned to assess the association of hair and urine lead levels with ADHD from the existing literature.
METHODS
The medical literature was searched in the following databases: PubMed, Embase, Google Scholar, The Cochrane Library (Cochrane Database of Systematic Reviews), ScienceDirect, and Web of Science.
The search strategy was with MeSH terms related to the lead levels in hair and urine with the associated outcome that is ADHD. The keywords used for the literature search were: lead levels, hair, urine, hair lead, urine lead, and ADHD. The period of publication was from January 01, 1990, to December 31, 2021, that was 32 years. The project proposal was registered in PROSPERO was CRD42020222036 dated December 22, 2020. In our study population, the ADHD children were aged 3–18 years. After obtaining the list of journals from all the databases, they were manually identified whether to be included in the systematic review and meta-analysis.
We included observational prospective cohort studies of all languages published in the last 32 years; from 1990 till date. The search and inclusion of studies were done by 2 authors (SS and SN) independently. The criteria that were used during the extraction process contained the following items: authors, publication year, the country where the study was conducted, study design, data collection, population, sampling technique, sample size, participant’s age range, participant’s age mean, other biomarker, risk factors associated (if any mentioned), hair and urine lead levels (quantity mentioned) and tool used for diagnosing ADHD. They were compiled as the quantity of lead levels in the hair and urine of ADHD-diagnosed children. The exclusion criteria were for children with intellectual disability or intellectual disorders due to any other cause. The exposure to lead was considered as long-term if the lead estimated in hair was more than normal limits or more than the controls.[7] Short-term lead exposure was defined as the presence of lead urine samples as a reflection of current blood levels[7], more than normal limits or more than the controls. As there was no literature stating the normal lead levels in hair and urine in children, we conducted the review with the levels compared in the two groups. Studies with measures of lead exposure in maternal samples only and animal studies were excluded. As the total number of studies, there were two for urine lead and three for hair lead levels, we could not conduct the meta-analysis which requires at least ten studies.[8] An older study (1983) had urine chelated lead reported[9], but could not be included as it was beyond the 32 years committed in our protocol.
The different tools used for the diagnosis of ADHD such as the Diagnostic and Statistical Manual of Mental Disorder-Fifth Edition (DSM-5) Criteria and National Initiative for Children’s Healthcare Quality (NICHQ) Vanderbilt Parent Rated ADHD Assessment Scale or others were noted. Subgroup analysis was proposed according to the tool used for ADHD, method of lead estimation, age of the child, and timing of sampling. Due to the small number of studies, subgrouping could not be performed.[8]
The pooled data were assessed for the risk association, quality, and bias for the association of lead quantity in hair and urine of ADHD children. The data analysis and interpretation were done using RevMan 5.4.1 software. The principal investigator graded the quality of research of the published studies as poor, fair, and good based on their inclusion/exclusion criteria, adequate reporting of outcome, variables, and methodology used in diagnosis and estimation of lead and was assessed by the co-author.
RESULTS
The studies included in this systematic review are either case-control observational studies or prevalence studies of a place or population. The risk of bias assessment and the causal association of Pb levels in the hair and urine of children with ADHD have been informally represented. This is because the tools used for diagnosis of ADHD, the intelligence and emotional quotient (EQ), and the sampling of the study population were not similar in the limited number of studies included for review, though all methods used are standard protocols in their respective counties [Table 1].
| Citations | Place of study | No. of participants | Age of children (in years) | Tools used for diagnosis of ADHD | Sample(s) used for Pb estimation | Method used for Pb estimation | Results | |
|---|---|---|---|---|---|---|---|---|
| ADHD | Healthy controls | |||||||
| Amgalan et al. 2020[10] | Ulaanbaatar city, Mongolia | 30 | 30 | 7–12 | DSM IV, EQ score, WISC, FSIQ | Hair, 2.5 cm from the scalp | ICP-MS | ADHD had significantly higher hair lead levels by 1.6–2.9 times than the control group |
| Li et al. 2020[11] | Guangzhou, China | 178 | 106 | 6–11 | DSM-5 | Urine, 1 mL | ICP-MS, internal standard used | Pb in the case group was 2.99 times higher than in the control group. Pb levels are expressed as Median and IQR. IQR was used to calculate the SD |
| Shin et al. 2014[3] | Korea | 41 | 42 | 8–15 | DSM IV, K-SADS-PL-K, K-ARS and ADS for severity, WISC-III for IQ | 0.15 g of hair, 3 cm from the scalp. Pb levels were expressed in ppm | ICP-MS | Pb in hair d the ADS scores and this was more prominent in children with ADHD. Hair Pb expressed as mg/100g of hair. Hence I multiplied the result by 10 to make it µg/g. |
| Wang et al. 2009[13] | 4 villages in China | 18 | 299 | 6–12 | The Abbreviated Symptom Questionnaire of Conner’s was used to rate ADHD. Intelligence levels were classified into 5 grades | Urine- 50–100 mL Hair-0.1g |
AAS | Their result supports the hypothesis of intelligence reductions because of lead exposure. They proposed long-term cumulative lead in hair has more likelihood to associate with intelligence injury than the recent lead in blood. |
ADHD: Attention deficit hyperactivity disorder, ICP-MS: Inductively coupled plasma mass spectrometry, DSM: Diagnostic and statistical manual of mental disorder, WISC: Wechsler intelligence scale for children, FSIQ: Full-scale intelligence quotient, AAS: Atomic absorption spectroscopy, EQ: Emotional quotient, SD: Standard deviation, IQR: Interquartile range, Pb: Lead, K-ARS: Korean ADHD rating scale, ADS: Attention deficit syndrome, DSM IV: Diagnostic and statistical manual of mental disorders, 4thedition K-SADS-PL-K: The schedule for affective disorders and schizophrenia for school-age children-present and lifetime version for Korea
Two of the authors individually went through the literature search and manual search of each article selected. The third author validated the findings and together the results were compiled. An initial search with the MeSH terms related to the lead levels in hair and urine with the associated outcome that is ADHD in our study population, that is children aged 3–18 years showed 12 articles. After full article retrieval and during analysis, a total of six articles were included which fulfilled our inclusion criteria, of which only one article had Pb levels estimated in both urine and hair [Figure 1]. There was no significant disagreement between the authors on the inclusion of studies and analyses done thereafter.
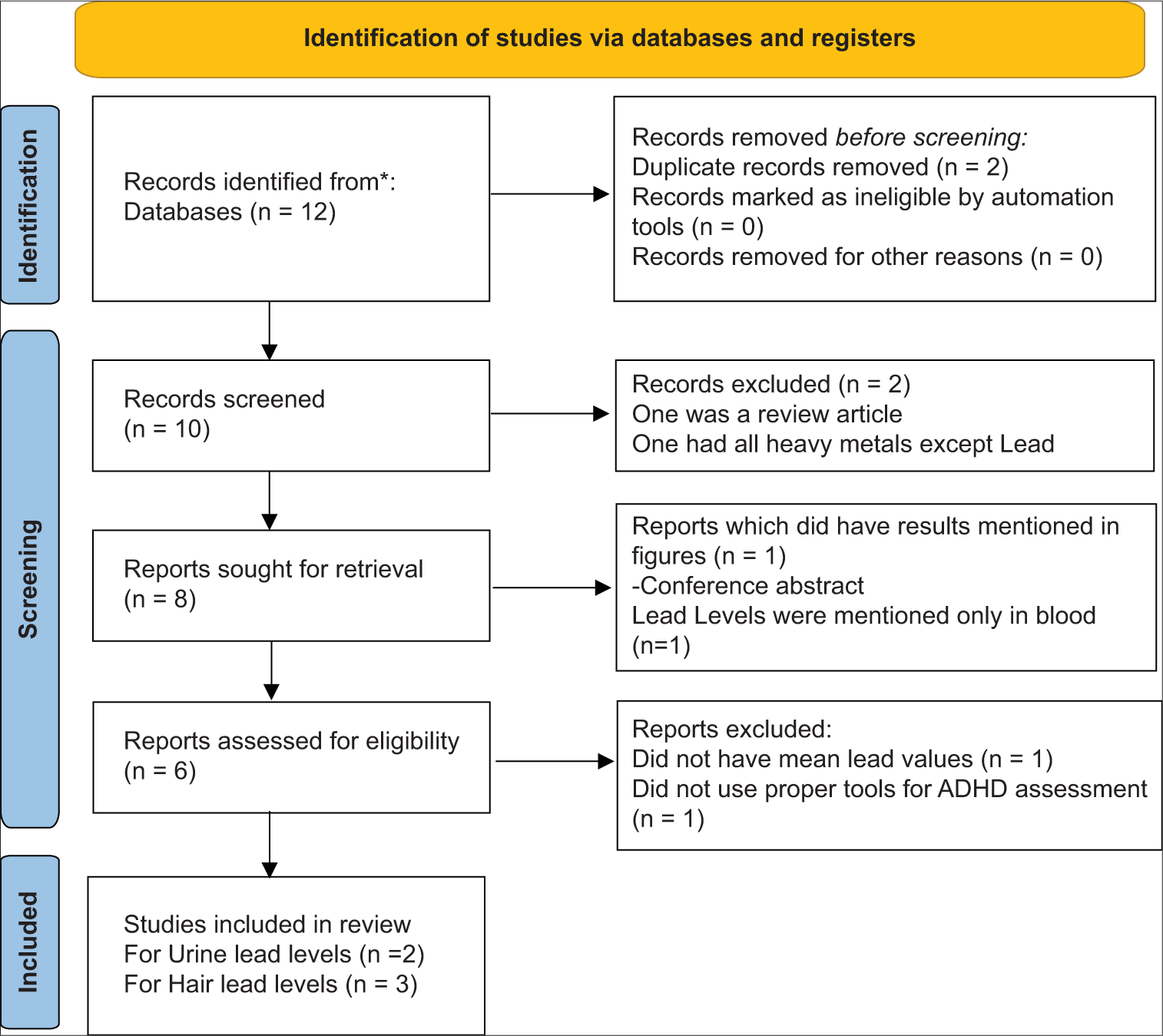
- A PRISMA flow diagram for urine and hair lead levels in attention deficit hyperactivity disorder (ADHD). n= number of articles, *is from PubMed, Embase, Google Scholar, The Cochrane Library (Cochrane Database of Systematic Reviews), Science Direct and Web of Science.
There were three studies which fitted the inclusion criteria for hair Pb levels. There were 478 participants, 89 cases, and 389 controls from three studies [Figure 2]. The pooled effect of standardised mean difference with a 95% confidence interval was 0.30 (0.03– 0.57). The overall effect Z was 2.16 which was statistically significant (P = 0.03). The Forest plot shown in [Figure 1] was arranged as per the weight of the study. The high heterogeneity, I2 = 91% depicted in [Figure 2] may be due to the different methods of diagnosis of ADHD used and the estimation of Pb levels in hair which are statistically significant (P < 0.0001).

- The mean hair lead levels in cases and controls. ADHD: Attention deficit hyperactivity disorder, SD: Standard deviation, CI: Confidence interval, IV: Inverse variance. The green squares designate the effect estimate of each individual study, their direction and the weight depend on the sample size. The black diamond designates the pooled effect of all studies.
The two studies included in the systematic review of urine Pb levels had 196 ADHD cases and 423 healthy controls [Figure 3]. The pooled effect of standardised mean difference with 95% confidence interval was 0.34 (0.13–0.56). The overall effect Z was 3.12 which was statistically significant (P = 0.002). The Forest plot shown in [Figure 3] was arranged as per the weight of the study.

- The mean urine lead levels in cases and controls. ADHD: Attention deficit hyperactivity disorder, SD: Standard deviation, CI: Confidence interval, IV: Inverse variance. The green squares designate the effect estimate of each individual study, their direction and the weight depend on the sample size. The black diamond designates the pooled effect of all studies.
Study design and subjects
All studies included were cross-sectional, case–control studies. Two were from China, and one each was from Korea and Mongolia. As per our protocol, we included studies done on children, their ages ranged from 6 to 15 years. The cases were diagnosed with ADHD either before sampling or were diagnosed during the study.
Methods used for diagnosis of ADHD
Two out of four studies used the DSM Fourth Edition (DSM-IV)[3,10] and one used the DSM-5.[11] The diagnostic criteria for ADHD are similar in DSM-IV and DSM-5. The same 18 symptoms noted in the DSM-IV are used and continue to be divided into two symptom domains (inattention and hyperactivity/impulsivity), of which at least six symptoms in one domain are required for diagnosis.[12] The fourth study used the Abbreviated Symptom Questionnaire of Conner’s to rate ADHD. Children with a summing score of ≥15 were regarded as having a behavioural deficits of ADHD. Revised Raven’s Standard Progressive Matrices were used for Intelligence scores. Intelligence levels were classified into 5 grades.[13] To evaluate cognitive functions or intelligence quotient (IQ), Wechsler Intelligence Scale for Children– Third Edition (WISC-III)[3] and Full Scale IQ and WISC.[10] were used. For the assessment of EQ, the Bar-On EQ Inventory-Youth version[14] was used by Amgalan et al.[10]
Methods used for estimation of lead levels
Three studies used inductively coupled plasma mass spectrometry for the assay of Lead levels in hair[3,10] and in urine.[11] One study used atomic absorption spectroscopy.[13] Both the methods are suitable for clinical use and on comparing the two methods, their results correlated well.[15]
DISCUSSION
ADHD is a chronic neurodevelopmental disorder according to DSM-5 that is characterised by a persistent and pervasive pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development.[12] The causes of ADHD are attributed to familial, biological, dietary, and environmental factors. Among the environmental factors, heavy metal exposure plays an important role in the pathogenesis of ADHD. Exposure to lead from household items, paints, exhaust fumes from vehicles and industries, batteries, and cosmetics contributes to lead levels in the body. Although the Centre for Disease Control has advised the initiation of public health measures if BLLs are >5 μg/dL, studies have shown that even lower blood levels of Pb are associated with ADHD.[16,17] At present, there are very few studies done on Pb levels in hair and urine. Those available for inclusion in our present systematic review mentioned that there was no safe level in children. There were no published levels of normal hair or urine Pb levels in children. Our findings depict that there is a significant overall effect of the association of lead in hair and urine with ADHD as compared to healthy children. However, the interpretation of these results needs caution due to the high heterogeneity among studies. Despite the heterogeneity, the definite association between Pb exposure and ADHD cannot be ignored. Goodlad et al. in their meta-analysis on the association of Pb and ADHD also reported a positive correlation between the two.[18] Therefore, it is unlikely that any future study that will be conducted will obtain a negative relation between Pb and ADHD. As the half-life of lead in our body is long; years to decades, blood Pb levels do not depict concurrent exposure. Exposure to Pb early in life, even low levels can affect neurological development and later lead to symptoms of hyperactivity and/or impulsivity.[19] Concurrent blood Pb levels are proportionate to the urine Pb levels and hair Pb levels depict earlier exposure but neither of them can reveal the actual age or the extent of lead absorption at that point in time.
Limitations of the study are that it is an observational study and may have suffered publication bias in the sense that, we would have missed studies not published in the databases we used for the literature search, or studies which were not published till date.
With the wide disparity in the number of studies conducted for blood Pb levels and those with hair and urine Pb levels in ADHD, it is imperative to screen for long and short-term exposure to lead in children using non-invasive methods.[2]
Scientific progress in understanding the association of Pb as the acausal factor of ADHD has hinted that the association is strong. At present, there are no cut-off levels for Pb in hair and urine in children. If it is known then adjuvant therapy can be given for Pb chelation and/or antioxidants to decrease the harmful effects of Pb in the body. Hence, it is crucial to conduct larger cross-sectional and cohort studies to derive decision-making outcomes from the research. ADHD being an impairing neurological disease in children can progress into adulthood and needs attention from researchers to enhance knowledge in prevention and treatment to lead these children into normal learning and make their adulthood more fruitful.
CONCLUSION
ADHD is a common disorder having multifactorial causes and varying degrees of severity. Most of the treatments available are limited by their efficacy and compliance. Leaving alone the non-modifiable factors like genetics and epigenetics due to intrauterine exposure and environmental exposure. We can attempt to decrease the disease burden of ADHD by Pb estimations by non-invasive methods such as in hair and urine which have better acceptance by parents. However, larger multicentric studies should be pursued to add to the knowledge that Pb accumulated can be removed and that the preventable causes of ADHD need early intervention to decrease disease severity and impairment.
Author contributions
The authors SS, JJ and SN conceived the idea, and prepared the protocol, and registered it in PROSPERO – CRD42020222036 dated 2212.2020. SS and SN did the literature search and that was counter-checked by JJ. SS prepared the 1st draft of the manuscript and JJ and SN critically edited the article. All of them agreed to the final manuscript.
Acknowledgements
We acknowledge the contributions of our colleagues in the library for helping us with the literature. We will be obliged to our institutions for the efforts taken to promote and encourage research.
Data availability statement
The research articles used in this systematic review are available for use.
Ethical approval
Institutional review board approval is not required.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Attention-deficit hyperactivity disorder. Lancet Lond Engl. 2020;395:450-62.
- [CrossRef] [PubMed] [Google Scholar]
- Hair lead levels related to children's classroom attention-deficit behavior. Arch Environ Health Int J. 1996;51:214-20.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between hair zinc and lead levels and clinical features of attention-deficit hyperactivity disorder. J Korean Acad Child Adolesc Psychiatry. 2014;25:28-36.
- [CrossRef] [Google Scholar]
- Pb neurotoxicity: Neuropsychological effects of lead toxicity. BioMed Res Int. 2014;2014:840547.
- [CrossRef] [PubMed] [Google Scholar]
- Childhood blood lead levels and symptoms of attention deficit hyperactivity disorder (ADHD): A cross-sectional study of Mexican children. Environ Health Perspect. 2016;124:868-74.
- [CrossRef] [PubMed] [Google Scholar]
- National center for environmental health, division of environmental health science and practice. 2021. Available from: https://www.cdc.gov/nceh/lead/prevention/blood-lead-levels.htm [Last accessed on 2023 Aug 01]
- [Google Scholar]
- Exposure to lead and specific attentional problems in schoolchildren. J Learn Disabil. 1994;27:393-9.
- [CrossRef] [PubMed] [Google Scholar]
- Analysing data and undertaking meta-analyses In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, eds. Cochrane handbook for systematic reviews of interventions version 6.3. Ch. 10. United Kingdom: Cochrane; 2022. Available from: https://www.training.cochrane.org/handbook [Last accessed on 2023 Aug 01]
- [Google Scholar]
- Lead and hyperactivity revisited. An investigation of nondisadvantaged children. Arch Gen Psychiatry. 1983;40:827-33.
- [CrossRef] [PubMed] [Google Scholar]
- Lead hair level impact on Mongolian children with attention deficit hyperactivity disorder. Occup Dis Environ Med. 2020;8:188-202.
- [CrossRef] [Google Scholar]
- Association between 10 urinary heavy metal exposure and attention deficit hyperactivity disorder for children. Environ Sci Pollut Res Int. 2020;27:31233-42.
- [CrossRef] [PubMed] [Google Scholar]
- DSM-5 changes: Implications for child serious emotional disturbance In: Rockville (MD): substance abuse and mental health services administration (US). 2016. p. :16-20. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519712/table/ch3.t3 [Last accessed on 2023 Aug 01]
- [Google Scholar]
- Adverse health effects of lead exposure on children and exploration to internal lead indicator. Sci Total Environ. 2009;407:5986-92.
- [CrossRef] [PubMed] [Google Scholar]
- The Bar-On model of emotional-social intelligence (ESI) Psicothema. 2006;18(Suppl):13-25.
- [Google Scholar]
- Determination of lead, cadmium and mercury in blood for assessment of environmental exposure: A comparison between inductively coupled plasma-mass spectrometry and atomic absorption spectrometry. Spectrochim Acta B At Spectrosc. 2006;61:980-90.
- [CrossRef] [Google Scholar]
- The association between lead and attention-deficit/hyperactivity disorder: A systematic review. Int J Environ Res Public Health. 2019;16:382.
- [CrossRef] [PubMed] [Google Scholar]
- Low blood lead levels and attention-deficit hyperactivity disorder in children: A systematic review and meta-analysis. Environ Sci Pollut Res. 2019;26:17875-84.
- [CrossRef] [PubMed] [Google Scholar]
- Lead and attention-deficit/hyperactivity disorder (ADHD) symptoms: A meta-analysis. Clin Psychol Rev. 2013;33:417-25.
- [CrossRef] [PubMed] [Google Scholar]
- Low blood lead levels associated with clinically diagnosed attention-deficit/hyperactivity disorder and mediated by weak cognitive control. Biol Psychiatry. 2008;63:325-31.
- [CrossRef] [PubMed] [Google Scholar]




