
Translate this page into:
Cardiac autonomic modulation during yoga postures and cycling: An “Acute State Effect”
*Corresponding author: Dr. Leena Phadke, Central Research Lab, Smt. Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India. leena_phadke@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Metkari A, Phadke L. Cardiac autonomic modulation during yoga postures and cycling: An “Acute State Effect”. Indian J Physiol Pharmacol 2020;64(3):229-35.
Abstract
Objectives:
Health benefits of aerobic exercises and Yogaasana (Yoga Postures) in lifestyle diseases are well known. There are pointers that these health benefits may be mediated through cardiac autonomic modulation. “Acute State effects” of autonomic modulation during aerobic exercise is fairly established; however there is relative dearth of information about it during Yogasana (Yoga Postures). The purpose of present study is to explore “Acute State Effect” of cardiac autonomic modulations during Yogasana (postures) and mild aerobic exercise (cycling) using heart rate variability (HRV) a cardiac autonomic marker in Yoga naïve volunteers.
Materials and Methods:
Thirty consenting volunteers between eighteen to twenty five years, of both genders performed test protocol comprised of four blocks of modified yoga postures, one block of cycling each of five minute duration and a block of supine rest that served as baseline. High sampled ECG (1 KHz) was recorded during protocol for HRV analysis. Friedman test for multiple blocks comparison and Wilcoxon signed rank test for pair wise comparison was employed. P < 0.05 considered as significant.
Results:
Multiple block comparison of HRV indices (P < 0.0001) and for breathing rate (P < 0.0004) were highly significant. Compared to resting baseline a pattern of vagal withdrawal (decrease in HF nu) with increment in average heart rate was observed during modified yogasanas and cycling. Shavasana showed pattern of parasympathetic reactivation with decrement in average heart rate.
Conclusion:
The pattern of autonomic modulation in Yoga naïve performing modified yogasanas was similar to mild intensity cycling. Shavasana showed pattern of post exercise recovery.
Keywords
Autonomic nervous system
Modified yogasana
Heart rate variability
Aerobic exercise

INTRODUCTION
Aerobic exercise and Yogasana (Yoga Postures) known to have health benefits in various diseases of public health importance, namely, diabetes mellitus, hypertension, cardiovascular diseases, anxiety, etc.[1-4] There are pointers that these health benefits may be mediated through modulation of autonomic nervous system.[5,6] While “Outcome Research” in both yoga and exercise has shown clinical benefits, the “process research” specifically related to yoga is still in its infancy.[7]
Heart rate variability (HRV), a non-invasive predictive and prognostic cardiac autonomic modulation marker, is extensively studied in exercise science for exploring the acute and training effects of exercise on cardiac autonomic modulation.[8] Initial parasympathetic withdrawal (indicated by decrease in HF component of HRV and tachycardia) and delayed sympathetic activation (indicated by increase in LF component (equivocal), blood pressure, cardiac output, heart rate, etc.) are fairly established observations of acute autonomic modulation during exercise,[9] while “Athletes bradycardia” due to increased vagal tone is a classic example of long-term exercise training effect on cardiac autonomic modulation.[10] Furthermore, cardiac autonomic modulation to orthostatic challenge (supine to standing) is also fairly known where the similar response of sympathetic augmentation (increased LF nu) and of vagal withdrawal (decrease in HF nu) was observed.[11,12] Stimuli-like changes in respiratory rate and tidal volume also have shown to affect the cardiac autonomic modulation indicated by changes in frequency components of HRV.[13]
Yoga, the traditional mind-body technique in its spectrum, includes various practices such as Yogasanas (set of multiple postures), Pranayama (set of different breathing techniques), and meditation (Dharana, Dhyana) and therefore in itself is a complex type of stimulus. Literature suggests that under the fold of yoga a typical yoga session includes either stand-alone (only Yogasana or Pranayam, or meditation) or combination of mentioned practices. Moreover, only yogasanas session in itself may consist of multiple sitting, supine, and standing postures. So is true for pranayama session where multiple breathing practices are employed in a single session. There are very few studies that explored autonomic modulation during yoga session and interestingly contradictory findings right from parasympathetic augmentation on the one hand to sympathetic augmentation on the other have been reported during a single yoga session.[14,15] To our understanding, these contradictory findings were may be due to the use of complex stimuli (multiple postures/multiple postures+pranayama/ multiple postures+meditation) during a single session that results in averaging of cardiac autonomic modulatory effects. This prompted us to use a protocol that involves holding different postures individually for 5 min each in a block design so that as far possible the constancy of stimulus can be maintained. Moreover, calorie expenditure wise yogasanas belong to mild aerobic activity,[16] it was thought useful to explore “Acute State Effect” of cardiac autonomic modulations during these postures and mild aerobic exercise (cycling). The insights in mechanisms of cardiac autonomic modulation may have therapeutic implication.
Objective of the study
The Objective of the study was to explore “Acute State Effect” of cardiac autonomic modulations during yogasana (postures) and mild aerobic exercise (cycling).
MATERIALS AND METHODS
The present study was observational exploratory research and was approved by the Institutional ethics committee.
Inclusion criteria
The following criteria were included in the study:
Age between 18 and 25 years of age
Consenting volunteers of both genders
Functional capacity of more than 5 METS (assessed by modified Bruce protocol).
Exclusion criteria
The volunteers with disabilities that hinder physical activity and those with medical conditions affecting HRV (known cases of heart diseases, hypertension, diabetes, etc.) were excluded. The sample size was estimated considering α = 0.05, and statistical power at 80% and the medium effect size (0.51) as proposed by Quantana,[17] for HRV studies by modeling effect size distribution that requires minimum of 25 participants per group. As the protocol in the present study allows the comparison of HRV indices between yogasana and exercise blocks with individuals own respective baselines, thus the single group in the present study represents the case-control model. Accordingly, 30 volunteers were enrolled for the study. Demographic profile of volunteers is given in [Table 1].
| n | 28 |
|---|---|
| Female volunteers | 16 |
| Male volunteers | 12 |
| Mean age | 21.43±0.84 |
| Mean weight | 64.04±12.94 |
| Mean height | 164.78±8.1 |
| Average METs | 10.31±0.77 |
MET: Metabolic equivalent
Procedure
All participants performed block protocol that comprised four blocks of modified yoga postures in a sequence of (Tadasana, modified Adhomukhsvanasana, modified Sirsasana, Shavasana, respectively) followed by a block of cycling and an initial block of supine rest that serves as baseline. The volunteers were asked to hold the postures for 5 min in each block and to exercise for 5 min. The volunteers were asked to do free breathing. A high sampled ECG (1 KHz) was recorded during the protocol using Chronovisor Ambulab (make Promorphosis Pvt. Ltd., Pune). The Raw ECG data were pre-processed as per the guidelines of Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology.[18] Standard time and frequency domain HRV indices were analyzed using Chronovisor Software (version 1.1.499, make Promorphosis Pvt. Ltd., Pune). An ECG derived respiration was measured post hoc using Kubios HRV Premium software 3.0.1.
Statistical analysis
Out of 30 ECG records, two recordings were non-analyzable. Therefore, data from 20 eight participants were used for final analysis using SPSS for Windows, version 16. Chicago SPSS Inc. Mean and SD (95% of C.I.) of time and frequency domain indices were measured. Wilcoxon Signed-rank test was used for pair-wise comparison of HRV indices between test blocks with resting baseline. P < 0.05 was considered as statistically significant.
RESULTS
The mean and standard deviation of HRV indices, average heart rate, and respiratory rate are shown in [Table 2].
| Blocks | RR (ms) | SDNN (ms) | TP (ms2) | LF (nu) | LF (ms2) | HF (nu) | HF (ms2) | LF/HF | AHR Beats/min | ABR Rate/min |
|---|---|---|---|---|---|---|---|---|---|---|
| Resting | 761.5±120.4 | 71.6±31.6 | 2839.8±2427.0 | 48.7±20.4 | 670±546 | 51.3±20.4 | 932±1038 | 1.6±2.2 | 80.7±12.8 | 12.4±3.7 |
| Tadasana | 631.3±86.2 | 52.8±22.3 | 1677.1±2035.8 | 73.3±13.7 | 669±805 | 26.7±13.7 | 311±486 | 3.9±2.8 | 96.6±12.2 | 12.77±3.5 |
| Mod. Adhomukhsvanasana | 649.2±92.3 | 53.2±25.3 | 1964.5±3063.4 | 64.8±15.2 | 553±473 | 35.2±15.2 | 462±876 | 2.4±1.5 | 94.3±13.6 | 13.05±3.8 |
| Mod. Shirshasana | 709.2±109.7 | 61.1±28.0 | 2205.4±2132.1 | 53.8±16.4 | 547±497 | 46.2±16.4 | 732±1044 | 1.5±1.1 | 86.6±13.4 | 13.65±4 |
| Mild exercise | 552.2±74.5 | 41.3±25.8 | 1240.6±2834.8 | 63.2±18.2 | 280±419 | 36.8±18.2 | 243±752 | 2.6±2.4 | 110.5±14.6 | 15.4±5.9 |
| Shavasana | 787.0±133.0 | 73.4±38.2 | 2816.2±2728.6 | 47.2±20.2 | 741±751 | 52.84±20.2 | 955±1114 | 1.3±1.4 | 78.4±13.5 | 13.9±4.3 |
RR: RR interval, SDNN: Standard deviation of normal to normal interval, TP: Total power, LF ms2: Low frequency, LF nu: Normalized units, HF ms2: High frequency, HF nu: Normalized units LF/ HF: Low-frequency/high-frequency ratio, AHR: Average heart rate, ABR: Average breathing rate. Mod.: Modified
Friedman’s test
Multiple block comparison for measured HRV indices (P < 0.0001) and for breathing rate (P < 0.0004) was highly significant. Moreover, there were significant differences in the means of HRV indices in all the blocks compared to each other. This significant difference between means was the basis for between block comparisons.
Wilcoxon signed-rank test
Yogasana and exercise block was compared with a resting baseline. As shown in [Table 3], compared to resting baseline, a significant decrement in RR interval, HF (ms2), total power, LF (ms2) power (Except Tadasana), and significant increment in LF (nu) and average heart rate was observed during Tadasana, modified Adhomukhsvanasa, modified Sirsasana, and Cycling. On the contrary, a significant increment in mean RR interval (P < 0.0001) and decrease in average heart rate was observed during Shavasana. Compared to the resting baseline, significant changes in breathing rate in all asanas and cycling were observed.
| Resting/Tadasana | Resting/Mod. Adhomukhsvanasana | Resting/Mod. Sirsasana | Resting/Cycling | Resting/Shavasana | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| t-value | P-value | t-value | P-value | t-value | P-value | t-value | P-value | t-value | P-value | |
| Mean RR | 0.00 | 7.4E–09** | 1 | 1.49E–08** | 42 | 0.0002** | 0.0 | 7.4E–09** | 64 | 0.001** |
| Total power (ms2) | 1 | 2.9E–08** | 60 | 0.009** | 88 | 0.01* | 28 | 0.001** | 186 | 0.9 |
| LF (ms2) | 195 | 0.8 | 134 | 0.1 | 115 | 0.04* | 28 | 6.7E–05** | 156 | 0.2 |
| HF (ms2) | 25 | 5.05E–05** | 55 | 0.0007** | 108 | 0.03* | 25 | 5.05E–05** | 194 | 0.8 |
| LF (nu) | 13 | 7.4E–09** | 1 | 1.49E–08** | 42 | 0.0002** | 69 | 0.002** | 192 | 0.8 |
| HF(nu) | 13 | 1.5E–05** | 41 | 0.0002** | 153 | 0.2 | 69 | 0.002** | 192 | 0.8 |
| LF/HF | 25 | 5.05E–05** | 55 | 0.0007** | 191 | 0.7 | 69 | 0.002** | 162 | 0.3 |
| AHR | 0.0 | 7.4E–04** | 1 | 1.4E–08** | 38 | 0.0001** | 0.0 | 7.4E–09** | 59 | 0.001** |
| ABR | –100 | 0.03* | –94 | 0.04* | –116 | 0.005** | –225 | 0.0003** | –190 | 0.002** |
DISCUSSION
In the present study to explore autonomic modulation during yogasana, and considering the technical requirements for HRV analysis, the block protocol was employed. Each block was comprised of a single posture that was hold for 5 min. Similarly, cycling block consisted of 5 min. For comparison, HRV in supine position was measured that serves as a baseline. The protocol has allowed us to observe “Acute state effect” of one single posture at a time. This design avoided the problem of averaging of autonomic modulation due to postural or practice changes in one single session. One minute pause was given between blocks to prevent the spillover effects of ANS modulation. As the participants were yoga naïve, modified versions of yoga postures (preparatory poses) were given so that participants could hold them for 5 min duration. [Figures 1-6] shows the modified asanas and mild aerobic activity (Figure 1 resting supine as baseline, Figure 2 Tadasana hands on sides, Figure 3 Modified Dog Pose or adhomukhsvanasana, Figure 4 Modified Shirsasana, Figure 5 Shavasana with instructions, Figure 6 cycling) used in protocol. The protocol was based on the previously used protocol designed by Phadke et al.[19]

- Resting baseline.

- Tadasana with hands-on sides.
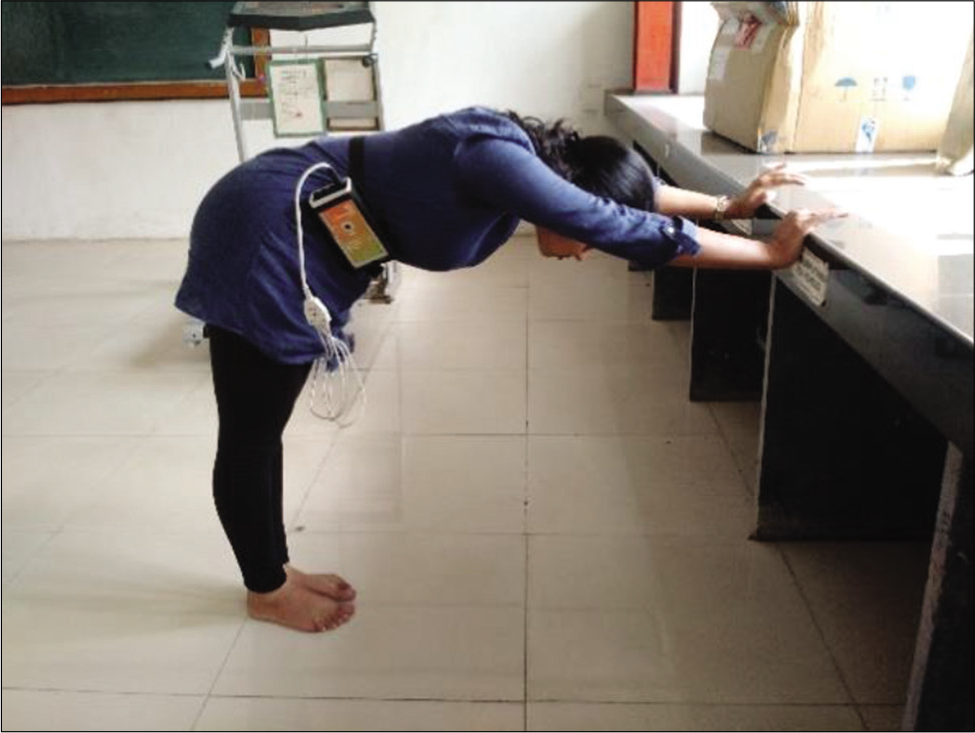
- Modified half dog pose.

- Modified Sirsasana.
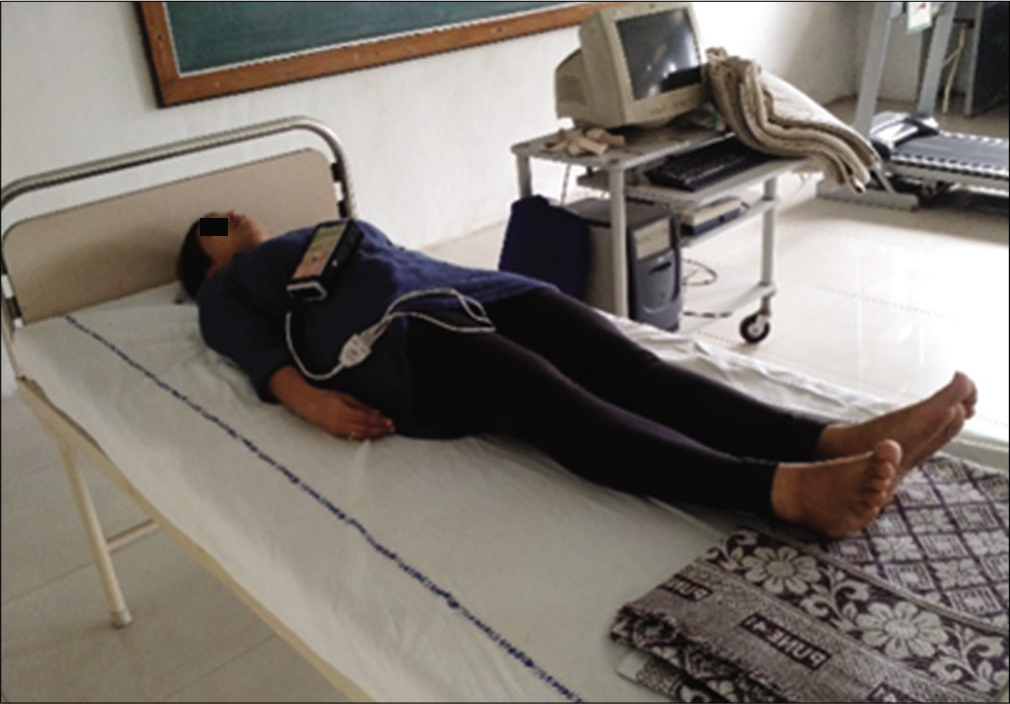
- Shavasana.

- Mild aerobic exercise (cycling).
All the participants were instructed to perform free breathing. Except Shavasana, a significant increase in breathing rate was observed during yogasana and cycling compared to resting baseline. However, it is worth to note that in none of the asanas and cycling, the mean respiratory rate was below resting and below the rate of eight beats per minute. As the HF frequency of HRV is a marker of respiratory sinus arrhythmia mediated through vagus, decrease in breathing frequency shifts the HF component of HRV into LF frequency band, thereby liable to erroneous interpretation about the vagal modulation.[20] However, in the present study, as breathing frequency in not less than eight per minute, the shifting of HF component to LF is duly ruled out.
In the present study in comparison to the resting baseline, two patterns of autonomic modulation were observed in yoga naïve individuals.
Pattern I: Significant parasympathetic withdrawal, with increase in mean heart rate
Significant decrease in mean RR, total power, HF nu, HF (ms2), and increment in LF (nu) was observed in Tadasana, modified Adhomukhsvanasana, modified Sirsasana, and Cycling. Similar findings were observed by Sarang and Tellis,[21] where they assessed HRV with multiple postures within a single block in yoga practitioners, by Melville et al[22] during yoga session comprising of multiple postures in comparison to control group by Lucini et al[23] and Yamamoto et al.,[24] as an initial autonomic adjustment to moderate exercise in volunteers and during an orthostatic challenge by Pagani et al.[25] Although the observations in yoga studies were similar, it cannot be truly comparable as our blocks were consisted of a single yoga posture as against to multiple postures in their studies. On the contrary, an overall parasympathetic predominance (measured by time RMSSD and PNN50 indices) was observed during yoga session in a study conducted by Khattab et al[26] The differences may be due to the fact that in their study, the practitioners were trained yoga practitioners and the protocol that was used comprised of different yoga postures in one session that might have averaged overall autonomic modulation.
It is a well-established fact that the HF component of HRV predominantly represents the outflow of vagus on heart (a marker of respiratory sinus arrhythmia). Therefore, a significant decrement in HF powers with a concomitant rise in heart rate reflects vagal withdrawal as a principal modulatory mechanism responsible for changes in heart rate during asanas and cycling. Interestingly, however, a significant decrement in LF (ms2) power was observed in modified Adhomukhsvanasana, modified Sirsasana, and Cycling compared to resting, and no change was observed during Tadasana. Similar observations regarding the decrement in LF (ms2) power were also reported by Lipsitz et al.[27] during orthostatic challenge and Warren et al.[28] during exercise. Prima facie it appears to be a contradiction if LF power is assumed to be a marker of sympathetic tone. Many controversies regarding the physiological interpretation of LF frequency band exists, many researchers presume that LF power adjusted to total power and HF power or respiration reflects the cardiac sympathetic tone, or an index of both sympathetic and cardiovagal modulation together, and some attributed the LF frequency band to baroreflex modulation of autonomic outflows (Goldstein et al.).[29] In the present study during asana and cycling we have observed decrement in absolute LF power along with increment in heart rate. It is well known that arterial baroreflex plays an important role in the moment-to-moment regulation of blood pressure. It does this partly by eliciting changes in heart rate, but its ability to do this (i.e., sensitivity) during exercise is reduced from rest. This reduction in arterial baroreflex sensitivity is attributed to resetting of baroreflex during dynamic exercise. This resetting considered to be mediated by stimulation of metabolically sensitive nerves within the muscles during leg cycling exercise (muscle metaboreflex) and central command from higher centres. In the present study our observation of decrement in LF power supports the LF component of HRV much more in favour of marker of baroreflex mediated autonomic adjustment rather than marker of sympathetic tone. Decrease in LF power during asanas and exercise suggests a change in baroreflex sensitivity that needs further exploration. A significant increment in normalized LF (nu) in all asanas and cycling on backdrop of decrement in LF (ms2) power is seen. This observation primarily may be attributed to decrement in HF (nu) component of HRV rather than true increment in normalized LF (nu). As all postures were maintained for 5 min, the delayed interaction between central command and peripheral reflexes like muscle metaboreceptors that contributes in sustenance of vagal withdrawal (Rowell and Oleary, 1990)[30] and delayed sympathetic activation (White and Raven, 2014) cannot be ruled out.[31] In the present study as blood pressure or other markers of sympathetic modulations (norepinephrine spillover, etc.) were not assessed; therefore, contribution of delayed sympathetic activation on heart rate response cannot be ascertained. Therefore, our results show that stand-alone modified yoga postures in yoga naïve volunteers generate a similar pattern of autonomic modulation as seen with aerobic exercise and orthostatic challenge (Vagal withdrawal with an increase in heart rate) contrary to popular belief that Yogasana increases the parasympathetic influence and decrease the heart rate.
Pattern II: Parasympathetic augmentation with decrease in mean heart rate during shavasana
Compared to resting baseline, a pattern of parasympathetic reactivation (as indicated by slight increase in HF [ms2] as well as HF [nu]), along with significant cardio deaccelaration was observed during shavasana. Santaella et al[32] and Vempati and Tellis[33] in their study where they have seen the shavasana and yoga-based guided relaxation on autonomic modulation also observed similar results. A similar pattern was also observed during the recovery phase of exercise by Perini et al.[34] The initial cardio deaccelaration can be contributed to fast phase of parasympathetic reactivation due to abrupt removal of central command (Pecanha et al),[35] together with abolished feedback from muscle mechanoreceptors, and delayed withdrawal of sympathetic system (Pichon et al),[36] the increment in LF (ms2) may be indicative of resetting of baroreflex function in the supine posture.
In the present study, the participants were yoga naïve individuals and the cardiac autonomic modulation observed during modified yogasana was similar to modulation observed during exercise (cycling). However, it will be interesting to compare the pattern of cardiac autonomic modulation in experienced yoga practitioners during traditional yoga practice session performed within the framework of the designed study protocol. It may shed light on autonomic trainability.
CONCLUSION
The present study evaluated “Acute state effects” of cardiac autonomic modulation during modified yogasanas and exercise. ANS modulation during modified yogasanas and cycling were similar, and modulation during shavasana reflects the recovery phase similar to post-exercise recovery in yoga naive individuals. We propose that to gain similar benefits as that of exercise, the modified yogasanas can be used as a safe alternative to other modes of exercises in patients with limited mobility or disabilities, restricting them to do aerobic exercises.
Acknowledgment
Dr. Sanjeev Sarmukkadum, Dr. Snajay Phadke MD, DPM Maharashtra University of Health Sciences Nasik, Maharashtra (India).
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Risk indices associated with the insulin resistance syndrome, cardiovascular disease, and possible protection with yoga: A systematic review. J Am Board Fam Pract. 2005;18:491-519.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of yoga based lifestyle intervention on state and trait anxiety. Indian J Physiol Pharmacol. 2006;50:41-7.
- [Google Scholar]
- Physical activity/exercise and diabetes: A position statement of the American diabetes association. Diabetes Care. 2016;39:2065-79.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Med Hypotheses. 2012;78:571-9.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of the exercise on autonomic nervous system in diabetics: A literature review. J Cardiol Ther. 2017;6:594-8.
- [CrossRef] [Google Scholar]
- Psychological research questions about yoga. Ment Health Relig Cult. 2000;3:71-83.
- [CrossRef] [Google Scholar]
- The role of heart rate variability in sports physiology. Exp Ther Med. 2016;11:1531-6.
- [CrossRef] [PubMed] [Google Scholar]
- Modulation of cardiac autonomic activity during and immediately after exercise. Am J Physiol. 1989;256:H132-41.
- [CrossRef] [PubMed] [Google Scholar]
- Heart rate variability in athletes. Sports Med. 2003;33:889-19.
- [CrossRef] [PubMed] [Google Scholar]
- Reproducibility of heart rate variability parameters measured in healthy subjects at rest and after a postural change maneuver. Braz J Med Biol Res. 2010;43:982-8.
- [CrossRef] [PubMed] [Google Scholar]
- Heart rate variability and autonomic activity at rest and during exercise in various physiological conditions. Eur J Appl Physiol. 2003;90:317-25.
- [CrossRef] [PubMed] [Google Scholar]
- Toward understanding respiratory sinus arrhythmia: Relations to cardiac vagal tone, evolution and biobehavioral functions. Biol Psychol. 2007;74:263-85.
- [CrossRef] [PubMed] [Google Scholar]
- Heart rate variability during sleep following the practice of cyclic meditation and supine rest. Appl Psychophysiol Biofeedback. 2010;35:135-40.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of pranayama on stress and cardiovascular autonomic function. Indian J Physiol Pharmacol. 2011;55:370-7.
- [Google Scholar]
- Hatha yoga practices: Energy expenditure, respiratory changes and intensity of exercise. Evid Based Complement Alternat Med. 2011;2011:241294.
- [CrossRef] [PubMed] [Google Scholar]
- Statistical considerations for reporting and planning heart rate variability case-control studies. Psychophysiology. 2017;54:344-9.
- [CrossRef] [PubMed] [Google Scholar]
- physiological interpretation and clinical use, Task force of the European society of cardiology and the North American society of pacing and electrophysiology. Circulation. 1996;93:1043-65.
- [Google Scholar]
- Differential modulation of sympathetic and parasympathetic influences during different yoga asanas: Understanding the process. Int J Basic Appl Physiol. 2012;1:271.
- [Google Scholar]
- Effect of respiration rate on short-term heart rate variability. J Clin Basic Cardiol. 1999;2:92-4.
- [Google Scholar]
- Effects of two yoga based relaxation techniques on heart rate variability (HRV) Int J Stress Manag. 2006;13:460-75.
- [CrossRef] [Google Scholar]
- Fifteen minutes of chair-based yoga postures or guided meditation performed in the office can elicit a relaxation response. Evid Based Complement Alternat Med. 2012;2012:501986.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of initial autonomic adjustments to moderate exercise in humans. J Hypertens. 1995;13:1660-3.
- [CrossRef] [PubMed] [Google Scholar]
- Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J Appl Physiol (1985). 1991;71:1136-42.
- [CrossRef] [PubMed] [Google Scholar]
- Spectral analysis of heart rate variability in the assessment of autonomic diabetic neuropathy. J Auton Nerv Syst. 1988;23:143-53.
- [CrossRef] [Google Scholar]
- Iyengar yoga increases cardiac parasympathetic nervous modulation among healthy yoga practitioners. Evid Based Complement Alternat Med. 2007;4:511-7.
- [CrossRef] [PubMed] [Google Scholar]
- Spectral characteristics of heart rate variability before and during postural tilt, Relations to aging and risk of syncope. Circulation. 1990;81:1803-10.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of autonomic blockade on power spectrum of heart rate variability during exercise. Am J Physiol. 1997;273:R495-502.
- [CrossRef] [PubMed] [Google Scholar]
- Low-frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp Physiol. 2011;96912:1255-61.
- [CrossRef] [PubMed] [Google Scholar]
- Reflex control of the circulation during exercise: Chemoreflexes and mechanoreflexes. J Appl Physiol (1985). 1990;69:407-18.
- [CrossRef] [PubMed] [Google Scholar]
- Autonomic neural control of heart rate during dynamic exercise: Revisited. J Physiol. 2014;592:2491-500.
- [CrossRef] [PubMed] [Google Scholar]
- Yoga relaxation (savasana) decreases cardiac sympathovagal balance in hypertensive patients. Med Express. 2014;1:233-8.
- [CrossRef] [Google Scholar]
- Yoga-based guided relaxation reduces sympathetic activity judged from baseline levels. Psychol Rep. 2002;90:487-94.
- [CrossRef] [PubMed] [Google Scholar]
- Plasma norepinephrine and heart rate dynamics during recovery from submaximal exercise in man. Eur J Appl Physiol Occup Physiol. 1989;58:879-83.
- [CrossRef] [PubMed] [Google Scholar]
- Heart rate recovery: Autonomic determinants, methods of assessment and association with mortality and cardiovascular diseases. Clin Physiol Funct Imaging. 2014;34:327-39.
- [CrossRef] [PubMed] [Google Scholar]
- Spectral analysis of heart rate variability during exercise in trained subjects. Med Sci Sports Exerc. 2004;36:1702-8.
- [CrossRef] [PubMed] [Google Scholar]




