
Translate this page into:
Effect of alcohol-dependence on cognitive performance in middle-aged men: Preliminary results
*Corresponding author: Dr. Dipti Magan, Assistant Professor, Department of Physiology, All India Institute of Medical Sciences, Bathinda - 151001, Punjab, India. diptimagan@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ghai P, Magan D, Aneja J, Sharma H, Chaudhary A. Effect of alcohol dependence on cognitive performance in middle-aged men: Preliminary results. Indian J Physiol Pharmacol. 2023;67:303-9. doi: 10.25259/IJPP_96_2023
Abstract
Objectives:
The understanding of the relationship between alcohol-related neuropathology, cognitive impairment, and various factors such as alcohol consumption, thiamine levels, and age vulnerability is still poorly understood. Therefore, this study aims to examine the effect of alcohol dependence on cognitive performance in middle-aged men with psycho-biochemical evidence.
Materials and Methods:
A cross-sectional pilot study with a comparison group including 82 right-handed participants with and without alcohol dependence (n = 41 each). Alcohol dependence was diagnosed clinically by the International Classification of Disease Tenth Edition along with the use of alcohol use disorder identification test (AUDIT) and cognitive screening tests, that is, the Montreal Cognitive Assessment (MoCA) and the Mini-Mental State Examination (MMSE). The serum levels of thiamine (Vitamin B1) were determined using an enzyme-linked immunosorbent assay.
Results:
The MoCA scores, MMSE scores, and serum thiamine levels were significantly low for alcohol-dependent men (1509.43 ± 898.63 pmol/L) versus non-alcohol-dependent men (1862.81 ± 741.30 pmol/L; P = 0.021). The cognitive sub-domains including orientation, execution, calculation, visuoconstructional skills, and recall functions were also significantly (P < 0.05) affected for the alcohol-dependent patients when compared to non-alcohol-dependent men. Serum thiamine levels showed a positive (P < 0.05) correlation with MoCA scores whereas serum thiamine levels showed a significant (P < 0.05) negative correlation with AUDIT scores.
Conclusion:
Based on the significant positive association between serum thiamine levels with MoCA scores; therefore, both may be used as a screening tool for the early detection of cognitive impairment in patients with alcohol dependence.
Keywords
Thiamine
Alcohol dependence
Cognition
Mini-mental state examination
Montreal cognitive assessment
Neurotoxic

INTRODUCTION
Alcoholism is associated with brain damage and poor cognitive functioning.[1] The alcohol-related neuropathology and cognitive impairment for different etiological factors, such as alcohol, thiamine levels, and age vulnerability show inconsistent evidence.[1-3] This variation is due to methodological limitations[4] in terms of study design, that is, population selection, age criteria, and a variety of neuropsychological tests measured. Few studies have also shown the effects of alcohol consumption on poor cognitive performance, particularly executive functions,[5-11] episodic and working memory.[10] In the present scenario, all clinicians use subjective analysis to assess the cognitive status of alcohol-dependent patients. Further, the assessment of how rapidly cognition is progressing has important clinical implications. For this, a biological marker for rapid cognitive decline would be of importance because at-risk patients can be targeted early for non-pharmacological, medical, and psychosocial interventions to slow deterioration. Thiamine, also known as Vitamin B1, exerts neuroprotective[6,9,12] effects by maintaining blood–brain barrier integrity and is particularly, studied as a biological marker for cognitive decline.[13] To date, no published literature is available to show the association between thiamine blood levels and cognition in alcohol-dependent patients among the Indian middle-aged population. With this background, the present study was designed with the primary objective of evaluating the effect of alcohol dependence on neurocognitive functions using Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), and cognitive biomarkerthiamine (Vitamin B1) levels among Indian middle-aged (36–55 years)[4] men with alcohol dependence compared to non-alcohol dependent subjects. The secondary objective was to assess the correlation between the effect of alcohol dependence (alcohol use disorder identification test [AUDIT] scores) on the MoCA scores, MMSE scores, and serum thiamine levels and also provide a scientific association between the serum thiamine levels and MoCA scores.
MATERIALS AND METHODS
The present study was a cross-sectional pilot study with a comparison group including 82 right-handed, middle-aged (36–55 years) men with and without alcohol dependence (n = 41 each), carried out at a tertiary care hospital (All India Institute of Medical Sciences [AIIMS], Bathinda) in Western Punjab. This study was conducted by the Helsinki Declaration and was approved by the Institutional Ethics Committee (IEC) (Ref. No.: IEC/AIIMS/BTI/085; dated 17/03/2021). All participants provided written informed consent. The study was registered at the Clinical Trial Registry India (CTRI), CTRI/2021/12/039034. The study was conducted from September to November 2021 (the 2 months of the study period for the undergraduate Indian Council of Medical Research, New Delhi-STS-project 2020) in the Department of Psychiatry in association with the Department of Physiology and the Department of Biochemistry at AIIMS, Bathinda. The sample size for the study was calculated using n-master 2.0[14] software assuming the prevalence[15] of cognitive decline between 30% to 80% and 95% confidence interval with an absolute precision of 10% which came out to be 41 for each group.
Alcohol-dependent (Group A) participants were recruited on the basis of dependency on alcohol assessed by the International Classification of Disease Tenth Edition (ICD-10) criteria for diagnosis of alcohol dependence along with AUDIT.[16] These patients came under F10 (alcohol withdrawal) according to ICD-10 criteria. The inclusion criteria include those participants who were willing to participate in the study program after the detoxification phase of 7–10 days was over. The average years of alcohol consumption were found to be 11.36 ± 6.85 (mean ± standard deviation) years. The exclusion criteria include patients with serious medical conditions, seriously sick, non-ambulatory, non-cooperative patients, with significant liver disease (cirrhosis of the liver), history of drug dependence other than nicotine or caffeine, clinical evidence of Wernicke–Korsakoff syndrome (WKS), a significant history of head trauma or brain surgery, organic brain syndrome, psychotic disorder, major depressive disorder, and bipolar disorder. Only clinical history was utilised to exclude other major psychiatric disorders.
An age-matched comparison group, Group B, that is, non-alcohol-dependent subjects was recruited from among the caregivers of patients attending the psychiatry outpatient department. The non-alcohol dependence was analysed on the basis of AUDIT scores. The subjects in the control group were non-alcohol dependent and few were social drinkers who were considered in Zone 1 based on the AUDIT scores according to the World Health Organisation (WHO) criteria.[9,17,18] Exclusion criteria include those subjects having any serious medical problem or psychiatric illness on anamnestic recall, taking alcohol within 24 h of cognitive function assessment, a significant history of head trauma or brain surgery, history of drug dependence other than nicotine or caffeine. The aim of including the age-matched non-alcohol-dependent group was only to compare the natural variation in cognitive functions with the alcohol-dependent group.
We recorded sociodemographic data including age, height (stadiometer, Holtain Ltd., UK) body weight (digital weighing balance, Seca, Germany), body mass index (BMI), education level (<12 years, equal to 12 years and higher than 12 years)[19] and family history of alcohol/drug use disorders through a family tree.
Cognitive assessments
All participants underwent cognitive assessment using the English and Hindi versions of MMSE and the MoCA in the present study. Both instruments were valid and reliable among Indians by taking cultural and linguistic differences into account.[6] MMSE and MoCA were conducted within 5–10 min and 10–15 min, respectively, by the student under the supervision of expert clinicians.
MMSE
The MMSE[20,21] is a 30-point questionnaire used extensively in clinical and research settings to measure cognitive impairment, including simple tasks in several areas: The test of time and place, the repeating lists of words, arithmetic such as serial subtractions of seven, language use and comprehension, and basic motor skills. The scoring for MMSE includes (a) scores between 24 and 30 is no cognitive impairment; (b) scores between 18 and 23 is mild cognitive impairment and (c) scores between 0 and 17 is severe cognitive impairment.
MoCA
The MoCA[22] is a brief 30-question questionnaire that helps to assess people for dementia. The 8.1 version of the MoCA test was translated into English provided by the MoCA test organisation (http://www.MoCAtest.org/). The MoCA was designed as a rapid screening instrument for mild cognitive dysfunction. It assesses different cognitive domains: Attention and concentration, executive functions, memory, language, visuoconstructional skills, conceptual thinking, calculations, and orientation. The MoCA may be administered by anyone who understands and follows the instructions, however, only a health professional with expertise in the cognitive field may interpret the results. The total possible score is 30 points; a score of 26 or above is considered normal.
AUDIT questionnaire
The authors used the validated AUDIT[16] which was developed by the WHO as a method of screening for alcohol dependence that includes alcohol consumption, drinking behaviour, and alcohol-related problems. AUDIT scores are interpreted as (a) 0–7 scores indicate low risk; (b) 8–15 scores indicate increasing risk; (c) 16–19 scores indicate higher risk and (d) 20 scores or more indicate possible dependence.
Estimation of cognitive biomarker
The concentration of serum levels of thiamine (Vitamin B1) was determined using a commercially available sandwich enzyme-linked immunosorbent assay kit (Immunotag, Geno Technology Inc., USA). Fasting venous blood samples (5 mL) were collected and allowed to clot for 10 min at room temperature and centrifuged at 2000–3000 rpm for 10 min. The serum was stored at −80°C until analysed. The limit of detection for Vitamin B1 levels ranged between 10 pmol/L and 4000 pmol/L. Quality control assays for biomarkers and validation were performed.
Statistical analysis
SPSS version 20.0 (IBM, Chicago, Illinois, United States of America, October 2020) was used for the statistical data analysis in this study. The normality of data was tested using the Kolmogorov–Smirnov test. The sociodemographic, MMSE scores, MoCA scores, serum Vitamin B1 levels, and cognitive sub-domains were analysed using the ‘Independent samples t-test.’ The association between the AUDIT scores, MoCA Scores, MMSE Scores, and serum Vitamin B1 levels was evaluated using ‘Pearson Correlation Coefficient.’ Significance was accepted at P < 0.05.
RESULTS
The present study included a total of 82 male participants with (n = 41) alcohol-dependent patients (age 41.72 ± 8.79 years) and (n = 41) non-alcohol-dependent subjects (age 43.34 ± 9.53 years) after meeting the inclusion and exclusion criteria [Table 1]. The alcohol-dependent patients had an average of 11.36 ± 6.85 years of alcohol consumption. No statistically significant differences were observed between alcohol-dependent and non-alcohol-dependent participants for age, education, BMI, systolic blood pressure, and diastolic blood pressure [Table 1].
 |
Neurocognitive assessments
For neurocognitive functions, both MMSE (26.46 ± 2.08; 29.09 ± 1.23; P = 0.001) and MoCA scores (23.14 ± 2.70; 28.18 ± 1.64; P = 0.008), respectively, were found to be significantly less for the alcohol- dependent patients when compared with the non-alcohol-dependent group. Further, the serum Vitamin B1 (thiamine) levels were found to be significantly (P = 0.021) low for alcohol-dependent patients (1509.43 ± 898.63 pmol/L) versus non-alcohol-dependent subjects (1862.81 ± 741.30 pmol/L) [Table 1].
Correlations between the different neurocognitive tests
Further, the correlations between the different neurocognitive tests, that is, MoCA scores, MMSE scores, and Vitamin B1 (thiamine) levels with AUDIT scores were evaluated using the Pearson correlation coefficient. The MoCA scores (r = −0.323; P = 0.039) and Vitamin B1 levels (r = −0.460; P = 0.002) had a significant negative correlation with AUDIT scores in middle-aged men with alcohol dependence [Figures 1a and b]. However, the MMSE scores were negatively correlated with AUDIT scores but no statistical significance (r = −0.215; P = 0.176) was observed between them. Importantly, the present study observed a significant (r = 0.550; P = 0.01) positive correlation between serum thiamine levels with MoCA scores [Figure 2].
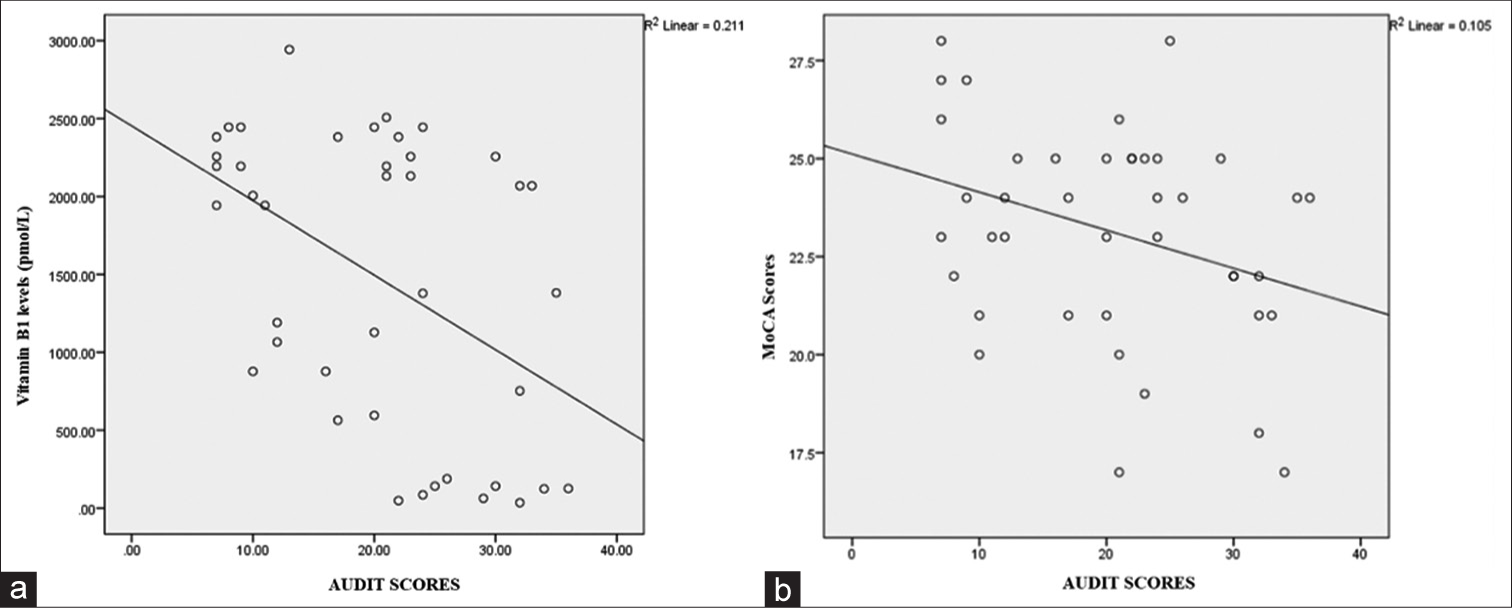
- (a) Correlation of alcohol dependence identification test (AUDIT) scores on thiamine (Vitamin B1) levels in alcohol-dependent patients, (b) correlation of alcohol use disorder identification test (AUDIT) scores on Montreal Cognitive Assessment (MoCA) scores.

- Correlation of Vitamin B1 levels with Montreal Cognitive Assessment (MoCA) scores in alcohol-dependent patients.
Sub-scores of cognitive domains assessed by MMSE and MoCA
Based on the distribution of each cognitive domain sub-score in total samples assessed by different items of MMSE and MoCA [Table 2]. The performance of orientation, execution, naming, registration, visuoconstructional skills, writing, and repetition was found to be significantly (P < 0.05) decreased in alcohol-dependent patients versus non-alcohol-dependent group using MMSE maximum scores; whereas orientation, execution, calculation, visuoconstructional skills and recall functions were found to be significantly (P < 0.05) decreased in alcohol-dependent patients versus non-alcohol-dependent group using MoCA test. Importantly, calculation, recall, visuoconstructional skills, and writing are affected in alcohol-dependent patients more significantly (P < 0.05) than non-alcoholic-dependent subjects.
 |
DISCUSSION
To the best of our knowledge, this is the first report from the Indian population providing psycho-biochemical evidence that cognitive functions deteriorate in middle-aged men with alcohol dependence. Further, the present study also focussed on the sub-analysis of the cognitive domains of MMSE and MoCA. It has been observed that calculation, recall, visuoconstructional skills, and writing are significantly affected more in our study population when compared with other study research findings.[10,23,24] This impairment in cognitive performance of sub-domains may be due to the alcohol addiction process that affects the thiamine metabolism[6,9,12] and leads to neurotoxicity which further affects the brain areas, especially shrinkage of the hippocampal region.[25]
The previous research findings observed the uncertainty in the association between alcohol drinking and cognitive dysfunctions. Some studies have found no association between alcohol drinking and cognitive impairment[26,27] or Alzheimer’s disease,[28] whereas others have found an association between heavy drinking and increased risk of dementia.[26,27,29] Some have claimed there is a J or U-shaped relation between alcohol drinking and cognitive impairment[2,4,10,13] or dementia[7,8,13] Importantly, these studies showed inconsistency in their findings due to the methodological limitations in terms of study design about population selection, age criteria and a variety of neuropsychological tests used and did not validate it by any clinical or diagnostic criteria for defining the mild cognitive impairment.[4] For this, the present study has also provided the associations between alcohol dependency with different neuropsychological tests. We observed a non-linear relationship between alcohol dependency (AUDIT scores) with cognitive tests, that is, MoCA scores. Importantly, serum thiamine levels showed a linear relationship with MoCA cognitive scores. This linear relationship provides the scientific affirmation that cognitive domains are affected due to a decrease in serum thiamine levels. Reduced cellular thiamine concentrations, combined with the toxic effects of ethanol and acetaldehyde, are considered crucial factors contributing to cognitive impairment among individuals with alcohol dependence and also heighten the risk of developing WKS. This finding provides the scientific platform for the need for early detection of cognitive decline.
Strengths and limitations of the study
The present comparative cross-sectional study in India provided psycho-biochemical evidence to show the impact of alcohol dependence on different cognitive domains in middle-aged men. The study also strengthened its findings by establishing correlations between MoCA scores and serum thiamine levels with AUDIT scores. In addition, the linear association of serum thiamine levels with MoCA scores provides scientific validity to affirm the early detection of cognitive decline in alcohol-dependent patients. In the present scenario, all clinicians use subjective analysis to assess cognitive status. Therefore, this study also tries to bring the superiority in the use of cognitive biomarkers, that is, serum thiamine levels along with MoCA scores rather than solely relying on subjective neurocognitive test MoCA for cognitive decline. Sub-domain analysis of the MoCA also revealed interesting trends, indicating that alcohol-dependent patients exhibited a more significant decline in the calculation, visuoconstructional skills, and recall domain when compared to the non-alcohol-dependent group. This study group comprised middle-aged men who were specifically selected for cognitive assessment so that potential pharmacological and non-pharmacological interventions could be done to effectively prevent cognitive decline in their future as they age. Further, longitudinal studies are warranted to understand the association between different cognitive domains with serum thiamine levels in alcohol-dependent populations.
Although the study was conducted with a relatively sound methodology, this study nonetheless has a few limitations. First, due to the small sample size, the findings of this study need to be corroborated in larger sample studies because the study being time-bound short-term research for undergraduate students (2 months) could not afford a larger sample. Second, only male subjects were recruited for the study. There were no firm criteria to exclude female patients but no reported case of females with alcohol dependence was found in the small district. Third, the percentage decrease in serum thiamine levels for the number of years of alcohol intake could not be carried out to assess the rate of cognitive decline in alcohol-dependent patients. Further, the diet assessment could not be carried out for the alcohol-dependent patients to provide a better explanation of the cognitive decline. Furthermore, the effect of nicotine on thiamine levels could not be carried out for the data analysis. Despite these limitations, the present findings provide psycho-biochemical evidence to aware alcohol-dependent patients aware of their cognitive status.
CONCLUSION
Based on the significant positive association between serum thiamine levels with MoCA scores, both may be used as a screening tool for the early detection of cognitive impairment in patients with alcohol dependence.
Acknowledgment
The MBBS-Second Professional undergraduate student would like to thank the Indian Council of Medical Research (ICMR)-New Delhi, for approving and providing the financial support for STS-ICMR research project-2020 (ID:2020-09331).
Author Contributions
Pankhita Ghai was involved in the study conduct and acquiring the data; Dipti Magan was involved in study conceptualization, study design, data analysis, data interpretation, writing of the manuscript, and approving the final content of the manuscript; Jitender Aneja was involved in data analysis, data interpretation and manuscript review; Himanshu Sharma was involved in the biochemical estimation of cognitive biomarker and manuscript review; Aarthi Choudhary was involved in assisting the student for data collection.
Ethical approval
This study was conducted by the Helsinki Declaration and was approved by the Institutional Ethics Committee (IEC) (Ref. No.: IEC/AIIMS/BTI/085; dated 17/03/2021).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Further evidence of relationship between thiamine blood level and cognition in chronic alcohol-dependent adults: Prospective pilot study of an inpatient detoxification with oral supplementation protocol. Alcohol. 2023;110:23-31.
- [CrossRef] [PubMed] [Google Scholar]
- Aging with alcohol-related brain damage: Critical brain circuits associated with cognitive dysfunction. Int Rev Neurobiol. 2019;148:101-68.
- [CrossRef] [PubMed] [Google Scholar]
- Cognitive control deficits in alcohol dependence are a trait-and state-dependent biomarker: An ERP study. Front Psychiatry. 2020;11:606891.
- [CrossRef] [PubMed] [Google Scholar]
- Alcohol use and cognitive aging in middle-aged men: The Vietnam era twin study of aging. J Int Neuropsychol Soc. 2023;29:235-45.
- [CrossRef] [PubMed] [Google Scholar]
- Does thiamine protect the brain from iron overload and alcohol-related dementia? Alzheimers Dement. 2020;16:1591-5.
- [CrossRef] [PubMed] [Google Scholar]
- Alcohol consumption and risk of dementia: The Rotterdam study. Lancet. 2002;359:281-6.
- [CrossRef] [PubMed] [Google Scholar]
- Alcohol drinking in middle age and subsequent risk of mild cognitive impairment and dementia in old age: A prospective population based study. BMJ. 2004;329:539.
- [CrossRef] [PubMed] [Google Scholar]
- Thiamine and phosphate esters concentrations in whole blood and serum of patients with alcohol use disorder: A relation with cognitive deficits. Nutr Neurosci. 2021;24:530-41.
- [CrossRef] [PubMed] [Google Scholar]
- Episodic and working memory deficits in alcoholic korsakoff patients: The continuity theory revisited. Alcohol Clin Exp Res. 2008;32:1229-41.
- [CrossRef] [PubMed] [Google Scholar]
- Group and case study of the dysexecutive syndrome in alcoholism without amnesia. J Neurol Neurosurg Psychiatry. 2000;68:731-7.
- [CrossRef] [PubMed] [Google Scholar]
- Thiamine metabolism is critical for regulating correlated growth of dendrite arbors and neuronal somata. Sci Rep. 2017;7:5342.
- [CrossRef] [PubMed] [Google Scholar]
- Neuropsychological assessment of cognitive function in chronic alcohol-dependent patients and patients with Alzheimer's disease. In Vivo. 2007;21:1115-8.
- [Google Scholar]
- nMaster 2.0-sample size software. 2011. Available from: https://www.cmc-biostatistics.ac.in/nmaster/ [Last accessed on 2021 Apr 22]
- [Google Scholar]
- Prevalence of cognitive impairment in patients with substance use disorder. Drug Alcohol Rev. 2019;38:435-42.
- [CrossRef] [PubMed] [Google Scholar]
- Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption--II. Addiction. 1993;88:791-804.
- [CrossRef] [PubMed] [Google Scholar]
- Use of AUDIT-based measures to identify unhealthy alcohol use and alcohol dependence in primary care: A validation study. Alcohol Clin Exp Res. 2013;37(Suppl 1):E253-9.
- [CrossRef] [Google Scholar]
- Alcohol consumption in India-an epidemiological review. J Family Med Prim Care. 2020;9:49-55.
- [CrossRef] [PubMed] [Google Scholar]
- Investigation of cognitive improvement in alcohol-dependent inpatients using the montreal cognitive assessment (MoCA) Score. J Addict. 2016;2016:1539096.
- [CrossRef] [PubMed] [Google Scholar]
- "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-98.
- [CrossRef] [PubMed] [Google Scholar]
- Applicability of the mini-mental state examination (MMSE) and the Hindi mental state examination (HMSE) to the urban elderly in India: A pilot study. Int Psychogeriatr. 2009;21:123-8.
- [CrossRef] [PubMed] [Google Scholar]
- Validity of the Montreal cognitive assessment (MoCA) index scores: A comparison with the cognitive domain scores of the seoul neuropsychological screening battery (SNSB) Dement Neurocogn Disord. 2021;20:28-37.
- [CrossRef] [PubMed] [Google Scholar]
- Psychiatric comorbidities associated with a positive screening using the montreal cognitive assessment (MoCA) test in subjects with severe alcohol use disorder. Drug Alcohol Depend. 2018;191:266-9.
- [CrossRef] [PubMed] [Google Scholar]
- Measuring cognitive impairment in young adults with polysubstance use disorder with MoCA or BRIEF-A-the significance of psychiatric symptoms. J Subst Abuse Treat. 2019;97:21-7.
- [CrossRef] [PubMed] [Google Scholar]
- Reduced thiamine is a predictor for cognitive impairment of cerebral infarction. Brain Behav. 2020;10:e01709.
- [CrossRef] [PubMed] [Google Scholar]
- Smoking, drinking, and incident cognitive impairment: A cohort community based study included in the gospel oak project. J Neurol Neurosurg Psychiatry. 2000;68:622-6.
- [CrossRef] [PubMed] [Google Scholar]
- Alcohol abuse, cognitive impairment, and mortality among older people. J Am Geriatr Soc. 2001;49:415-20.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors for Alzheimer's disease: A prospective analysis from the Canadian study of health and aging. Am J Epidemiol. 2002;156:445-53.
- [CrossRef] [PubMed] [Google Scholar]
- Cognitive function after 11.5 years of alcohol use: Relation to alcohol use. Am J Epidemiol. 2002;156:747-52.
- [CrossRef] [PubMed] [Google Scholar]




