
Translate this page into:
Isotonic hydroxyethyl starch is ineffective in restoring blood pressure during experimental septic shock: Implications for fluid resuscitation strategies
*Corresponding author: Alexandre Giusti-Paiva, Department of Physiology, Universidade Federal de Alfenas, Alfenas, State of Minas Gerais, Brazil. agiustipaiva@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Santiago MB, Vilela FC, Giusti-Paiva A. Isotonic hydroxyethyl starch is ineffective in restoring blood pressure during experimental septic shock: Implications for fluid resuscitation strategies. Indian J Physiol Pharmacol. 2024;68:1-8. doi: 10.25259/IJPP_286_2023
Abstract
Objectives:
The objectives of the study were to evaluate the effect of isotonic or hypertonic hydroxyethyl starch (HES) solutions on blood pressure and to assess the influence of the neurohypophyseal system on this response during experimental septic shock. Male Wistar rats were randomly allocated to undergo either cecal and ligation puncture (CLP) or a simulated surgical procedure (sham).
Materials and Methods:
Of 6 h post-surgery, either isotonic saline (0.9% sodium chloride, 4 mL/kg), isotonic (HES; at doses of 4, 8 or 16 mL/kg), or hypertonic saline-HES (HS-HES; 4 mL/kg) was administered through the endovenous route, followed by the recording of blood pressure and heart rate. In addition, the levels of sodium, vasopressin, and oxytocin were evaluated after the fluid infusion.
Results:
The administration of HES did not have a significant effect on blood pressure in our study. However, the HS-HES solution increased plasma osmolality, sodium, vasopressin, and oxytocin levels. Furthermore, the HS-HES induced a transient elevation in blood pressure immediately after infusion, which could be completely blunted by the pre-administration of a V1-vasopressin antagonist.
Conclusion:
Our results demonstrate that the infusion of an isotonic blood volume expander during experimental septic shock is ineffective in restoring blood pressure due to blood vessel compliance. In contrast, the infusion of a hypertonic solution stimulates vasopressin secretion and can transiently restore blood pressure.
Keywords
Cecal ligation and perforation
Hydroxyethyl starch
Neurohypophyseal hormones
Oxytocin
Vasopressin

INTRODUCTION
Per the Third International Consensus Definition for Sepsis and Septic Shock (Sepsis-3), sepsis is viewed as a potentially lethal medical situation originating from the body’s reaction to an infection leading to organ dysfunction.[1] Septic shock, a subcategory of sepsis, is distinguished by anomalies in circulation, cellular function, and metabolism, all contributing to a considerable elevation in mortality risk.[1,2]
Resuscitation with intravenous fluids to increase intravascular volume is a life-saving treatment and constitutes a cornerstone of care for patients with sepsis in the intensive care unit.[3-8] Intravenous (IV) fluid resuscitation is crucial for treating severe sepsis patients and the effects of different IV fluids have been extensively studied.[7,9] However, there is still controversy surrounding the optimal fluid replacement strategy, particularly with regard to kidney function.[10,11]
Solutions of colloids consist of substances with a high molecular mass that typically cannot traverse the capillary barrier. They are universally recognised for their role in amplifying intravascular volume, achieved through augmentation of the oncotic pressure inside the capillary compartment.[12,13] Compared to crystalloids, colloids are preferred for fluid resuscitation due to their longer intravascular retention time, lower required amount of fluid for resuscitation,[14] and faster circulatory stabilisation.[13,15] Conversely, the administration of hypertonic saline, classified as a crystalloid solution, enhances circulatory conditions by supplying fluid from an external resource while also recruiting water from the extravascular space.[6,16] This osmotic change may stimulate the secretion of vasopressin and oxytocin from the neurohypophysis through stimulation from osmoreceptors.[17] Hydroxyethyl starch (HES) is an amylopectin-based colloid, synthesised from either maize or sorghum-origin starch. Hypertonic saline-HES (HSHES) solutions exhibit complexity as they comprise two components: Sodium chloride, primarily accountable for the osmotic gradient, and HES, incorporated to extend the ephemeral volume effect of hypertonic saline. Thus, the hypertonicity of the HES solution increases the ability to retain water retention in the vascular space.[18]
Previous research has shown that hypertonic solutions can temporarily raise blood pressure and improve lung injury in rats with sepsis induced by cecal ligation and puncture (CLP) in rats.[19] HES has also been found to be effective in restoring and maintaining blood pressure, as well as improving blood flow to organs after resuscitation from haemorrhagic shock.[4,15] Studies conducted on cardiac surgical patients have demonstrated that administering HES during the perioperative period can lead to stable hemodynamics.[20,21] The use of HES during septic shock is often misunderstood and little attention has been given to the mechanisms responsible for the failure of fluid to correct hypotension.[10,22] This study aims to evaluate the effect of isotonic and hypertonic solutions of HES 130/0.4 on blood pressure during experimental septic shock. The objective is to understand why fluid resuscitation fails to correct hypotension in this condition.
MATERIALS AND METHODS
Animals
Adult male Wistar rats weighing between 230 g and 260 g were housed in groups of four per cage (dimensions: 39 × 36 × 18 cm) under standard laboratory conditions. The animals were kept in a temperature-controlled room maintained at 24 ± 1°C with a 12 h light/dark cycle. They had unrestricted access to food and water and were housed in the Animal Care Unit of the Department of Physiology of the institution. All experimental procedures were conducted by the Animals in Research: Reporting In Vivo Experiments guidelines and approved by the Ethics Committee of the Federal University of Alfenas (3/14/2018). To prepare the rats for experimentation, they were first anaesthetised with tribromoethanol (250 mg/kg b.w.). Next, a Silastic catheter was inserted into the right external jugular vein to allow for the administration of drugs, saline, or HES solution. In addition, a polyethylene catheter was inserted into the abdominal aorta through the femoral artery. The catheter was then tunnelled under the skin and externalised on the animal’s dorsum, allowing it to be connected to the transducer system for recording mean arterial pressure (MAP) and heart rate (HR). The rats were given 24 h to recover from the surgery procedure. After this surgical procedure, the rats were administered a subcutaneous dose of ketoprofen (1%; 0.1 mL/rat) and placed in individual boxes with free access to water and food pellets.
The V1 receptor antagonist (β-mercapto-β, β-cyclopentamethylenepropionyl1, O-Et-Tyr2, Val4, and Arg8-vasopressin) and oxytocin receptor antagonist (atosiban) were purchased from Sigma Chemical Co. (São Paulo, Brazil). The HES 130/0.4 was purchased from Fresenius Kabi (Campinas, SP, Brazil). The doses for both antagonists were chosen based on the previous studies.[16,19,23]
Experimental protocols
Measurement of arterial blood pressure
A day post-animal preparation, the MAP and HR were recorded in unanaesthetised rats using an amplifier interfaced with a computerised acquisition system (Powerlab, ADInstruments, Australia). Subsequent to roughly 30 min of baseline MAP recording, the rats were anaesthetised with tribromoethanol (250 mg/kg body weight) and immediately subjected to either CLP a sham surgical procedure. Their MAP was then monitored during the following 24 h. Sepsis was induced by CLP following previously published protocols.[19,24] Briefly, the rats’ abdomen was incised, followed by the exposure and partial obstruction of the cecum at the level of the distal ileocecal valve. Subsequently, the cecum was punctured 10 times at various avascular spaces using a 16-gauge needle. After confirming stool extravasation, the cecum was repositioned into the abdominal cavity and sutured. The MAP of the rats was monitored over the next 24 h. Rats that underwent the sham operation experienced the same surgical protocol, with the exception that their caecum was not subjected to either ligation or puncture (n = 6). 6 h after CLP, the animals were randomly assigned to one other five groups (n = 6 per group). These groups differed in the composition or volume of the resuscitative fluid administered over 2 min: Isotonic saline solution (IS; 0.9% sodium chloride (NaCl); 4 mL/kg b.w.; placebo group); 0.9% NaCl in 6% HES 130/0.4 (HES; dosages of 4, 8, or 16 mL/kg b.w.); or 7.5% NaCl in 6% HES 130/0.4 (HS-HES; 4 mL/kg b.w.). The infusions were administered 6 h after the CLP, as this period is typically associated with hypotension and inappropriately low vasopressin secretion.[19]
To investigate the role of vasopressin and oxytocin in the cardiovascular response following fluid resuscitation after CLP we administered a V1 receptor antagonist (10 μg/kg b.w.), an oxytocin receptor antagonist (atosiban; 1 mg/kg b.w.), or 1 mL/kg of sterile saline (n = 6 per group) intravenously 5 min before the infusion of HS-HES or isotonic HES (16 mg/kg), 6 h after the CLP surgery.[16,19] At the conclusion of the experimental procedure, the rats were euthanised through an excessive inhalation dose of halothane.
Plasma hormones, sodium concentrations, haematocrit, and osmolality determination
To evaluate the impact of different resuscitative fluids on haematocrit, plasma sodium, plasma osmolality, and plasma levels of vasopressin and oxytocin, a novel cohort of animals was employed. After inducing sepsis, a distinct group of rats was randomly assigned to one of five treatment groups (n = 6 per group), each characterised by a specific resuscitative solution: IS solution (IS; 0.9% NaCl; 4 mL/kg body weight, placebo group); 0.9% NaCl in 6% HES 130/0.4 (HES; at doses of 4, 8 or 16 mL/kg b.w.) or 7.5% NaCl in 6% HES 130/0.4 (HS-HES; 4 mL/kg b.w.).
Just before the initiation of fluid infusion, a 200 μL blood sample was collected through a catheter in the jugular vein. The rats were euthanised 30 min after receiving intravenous administration of the respective fluid resuscitation, as the required blood volume for vasopressin and oxytocin measurements was approximately 2 mL. Blood specimens were collected in pre-cooled plastic tubes imbued with heparin. Subsequently, these samples underwent centrifugation for 20 min at a force of 2,500 g and a temperature of 4°C. The resulting plasma samples were preserved at a temperature of −80°C for posterior hormonal analysis utilising a radioimmunoassay method.[25] Haematocrit, plasma osmolality, and plasma sodium concentration were measured using an automatic electrolyte analyser (Cobas b121, Roche, Germany).[26] All samples were assayed in duplicate in the same assay to ensure accuracy.
Statistical analysis
The data are expressed as means ± standard error of the mean. Statistical analyses between distinct groups were performed by implementing one-way analysis of variance (ANOVA), succeeded by post hoc assessments employing the Student–Newman–Keuls test for individual variances, or through repeated measures ANOVA complemented by a Bonferroni adjustment for multiple comparisons. P < 0.05 was considered indicative of statistical significance.
RESULTS
During the first 30 min before CLP or the sham surgery, there were no differences in baseline MAP and HR observed between the rats. However, rats subjected to CLP showed a significant reduction in MAP [Figure 1a] and an increase in HR [Figure 1b] compared with the sham group. This effect on MAP remained throughout the recording period (from 2 to 24 h), despite the infusion of different resuscitation fluids. At 6 h of CLP surgery, IS, HES, and HS-HES were infused (as indicated by the arrows in Figures 1a and b) and the effects on MAP and HR are shown in [Figures 1c and d], respectively. The infusion of IS did not change MAP and HR in CLP rats. Moreover, the administration of HES at doses of 4–16 mL/kg also did not induce a change in MAP in this experimental septic shock. In contrast, the administration of HS-HES resulted in an increase in blood pressure, with the most pronounced pressor response observed 2 min after the completion of the infusion. The pressor response remained high approximately 1 h after infusion, but after 6 h (12 h after CLP), no differences were observed compared to the CLP group. The HR, which increased after CLP surgery, declined immediately after infusions with 16 mL/kg HES and HS-HES and less intensely after infusions with HES 4 and 8 mL/kg [Figure 1d].

- Alterations in (a) arterial pressure and (b) heart rate over a period of 24 hours, as well as the immediate impact on (c) arterial pressure and (d) heart rate were quantified in animals subjected to septic shock induced by cecal ligation and puncture cecal ligation and puncture (CLP) or the sham operation following the endovenous administration of isotonic saline (IS; 0.9% sodium chloride (Nacl), 4 mL/kg), isotonic hydroxyethyl starch (HES in 0.9% NaCl; dosages of 4, 8 and 16 mL/kg) or hypertonic saline hydroxyethyl starch (HS-HES; HES in 7.5% NaCl; 4 mL/kg). The results represent the means ± standard error of the mean derived from six animals per group.
Furthermore, the administration of HES at doses of 4–16 mL/kg had no significant effect on plasma sodium levels [Figure 2a] or plasma osmolality [Figure 2b], but did result in a reduction of haematocrit levels [Figure 2c]. The reduction in haematocrit was more pronounced with higher doses of HES. IS injection did not affect haematocrit, plasma sodium, or plasma osmolality. However, HS-HES administration led to an increase in plasma sodium and osmolality. Moreover, HS-HES administration resulted in a significantly greater reduction in haematocrit compared to lower doses of HES (4 or 8 mL/kg), which was similar to the effect of HES at a dose of 16 mg/kg. In addition, the administration of either IS or HES (4–16 mL/kg) had no effects on plasma-level vasopressin [Figure 3a] or oxytocin [Figure 3b], with the exception of the infusion of 16 mL/kg HES, which resulted in increased oxytocin levels when compared to CLP group rats that did not receive fluid resuscitation. Moreover, HS-HES administration led to a significant increase in plasma levels of both vasopressin and oxytocin.
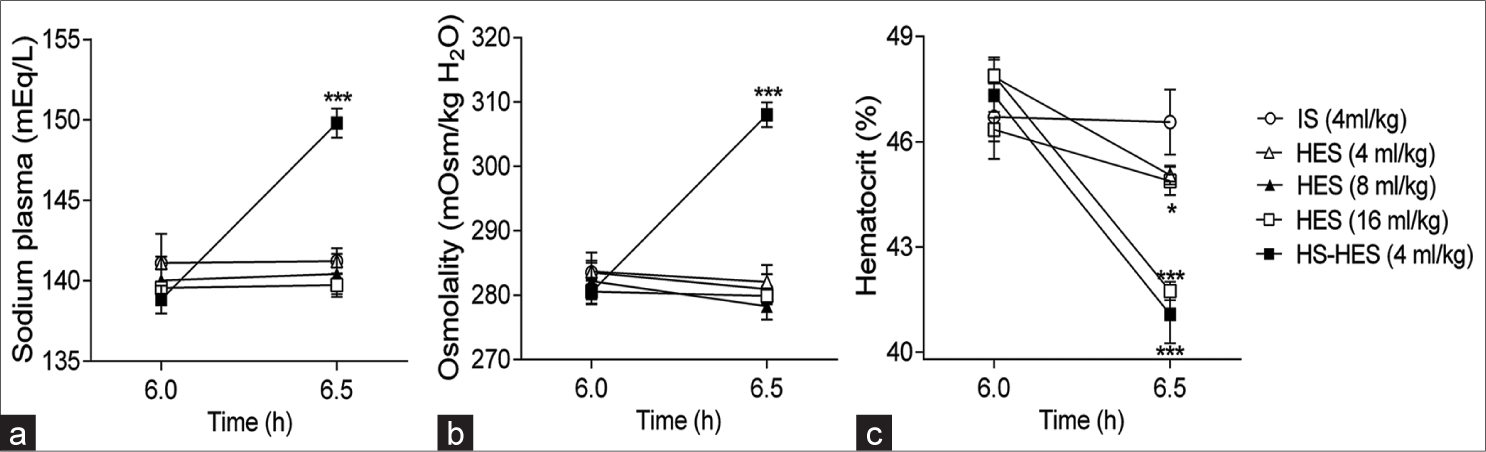
- The impact of endovenous administration of isotonic saline (IS) (0.9% sodium chloride (Nacl)), isotonic hydroxyethyl starch (HES in 0.9% NaCl at dosages of 4, 8 and 16 mL/kg), or hypertonic saline hydroxyethyl starch (HS-HES; HES in 7.5% NaCl at 4 mL/kg) on (a) plasma sodium levels, (b) plasma osmolality, and (c) hematocrit was examined 6 h post cecal ligation and puncture in rats. The presented data embody the means ± standard error of the mean derived from eight animals per group. The indicators *P < 0.05 and ***P < 0.001 demonstrate statistically significant differences when compared to the IS treatment group.
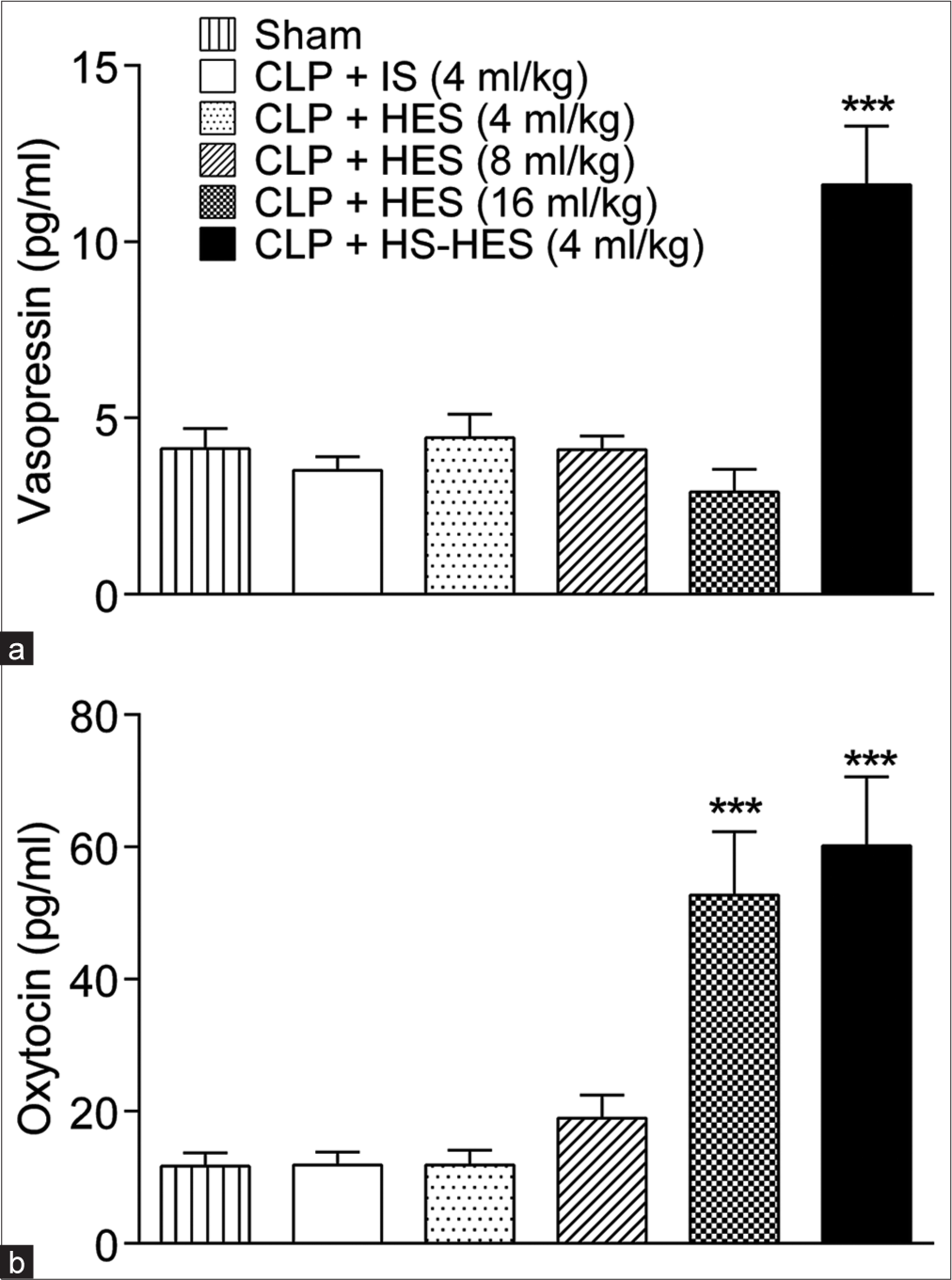
- The levels of plasma (a) vasopressin and (b) oxytocin were measured 30 min subsequent to the endovenous administration of isotonic saline (IS) (0.9% sodium chloride (Nacl)), isotonic hydroxyethyl starch (HES in 0.9% NaCl at doses of 4, 8 and 16 mL/kg), or hypertonic saline hydroxyethyl starch (HS-HES; HES in 7.5% NaCl at 4 mL/kg) in rats exposed to CLP. The reported data constitute the means ± standard error of the mean from eight animals per group. ***P < 0.001 denotes a statistically significant difference in comparison to the IS treatment group.
Figure 4 illustrates how the pressor response during fluid replacement with HS-HES is affected by the V1 receptor antagonist or the oxytocin receptor antagonist. Before the infusion of HS-HES, no differences in MAP and HR were observed between the rats that received either the V1 receptor antagonist or the oxytocin receptor antagonist. However, the pre-administration of the vasopressin V1 receptor antagonist abolished the increase in MAP [Figure 4a] caused by HSHES infusion, while it had no effect on the decrease in HR [Figure 4b]. Conversely, pre-administration of oxytocin receptor antagonist (atosiban) did not affect MAP or HR following HS-HES infusion [Figure 4a]. In addition, atosiban did not promote any changes in MAP [Figure 4c] and HR [Figure 4d] after infusion with HES at a dose of 16 mL/kg.
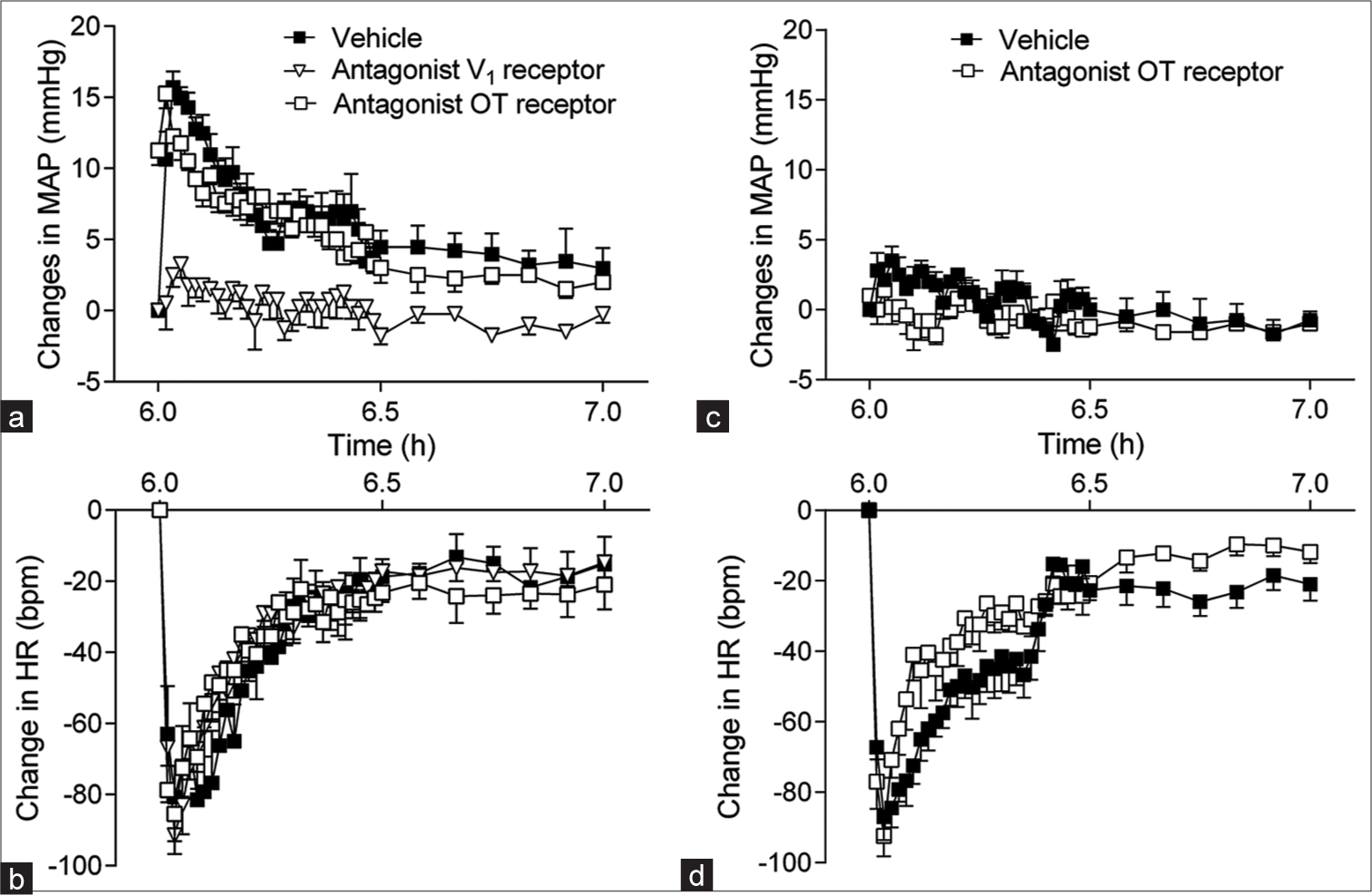
- Alterations in (a) arterial pressure and (b) heart rate over a period of 24 hours, as well as the immediate impact on (c) arterial pressure and (d) heart rate. Changes in the mean arterial pressure (MAP) and heart rate (HR) during the administration of hypertonic saline hydroxyethyl starch (HS-HES; HES in 7.5% sodium chloride (NaCl); 4 mL/kg; a and b, respectively) were examined following the injection of either a vehicle, the V1 receptor antagonist (10 μg/kg) or the oxytocin receptor antagonist (atosiban; 1 mg/kg). Similarly, the impact of vehicle injection or the oxytocin receptor antagonist (atosiban; 1 mg/kg) on changes in MAP and HR during the administration of isotonic hydroxyethyl starch (HES in 0.9% NaCl; 16 mL/kg; c and d, respectively) was studied. The data presented correspond to the means ± standard error of the mean for six animals per group.
DISCUSSION
In our study, we observed that the administration of isotonic fluid with HES 130/0.4 (in an isotonic solution) was ineffective in increasing blood pressure during septic shock induced by CLP. However, we found that the infusion of a small volume of HS-HES solution resulted in increased vasopressin plasma levels and restored blood pressure. By comparing the pressor effects of isotonic HES and HS-HES during similar volume expansion, we can infer that the lack of a vasoconstrictor agent, combined with the increased vascular compliance observed in experimental septic shock, may contribute to the ineffectiveness of isotonic HES in this experimental scenario. In contrast, the use of HS-HES demonstrated that its pressor effect is accompanied and mediated by an increase in vasopressin secretion, which likely compensates for vascular compliance in septic shock.
HES is a synthetic colloid solution that has been used for fluid resuscitation in clinical practice for many years.[9,10] It is particularly useful in critically ill patients with hypovolemic shock, as it rapidly expands plasma volume and maintains blood pressure, and may improve microcirculatory blood flow while reducing the need for blood transfusions. Previous studies have shown negative effects of old-generation HES, such as HES 200/0.60–0.66 hexastarch or HES 200/0.5 pentastarch, on renal function in septic patients.[27,28] In addition, a meta-analysis by Tseng et al.[29] found that the use of HES in septic patients was associated with a higher risk of renal failure and mortality compared to crystalloids. Moreover, another relevant aspect that needs to be studied is the mechanism(s) responsible for the failure of fluid to correct hypotension in septic shock, compared to its effect on other causes of shock.[4,5] Thus, the present study evaluated the effect of isotonic and hypertonic HES 130/0.4 solution on blood pressure and the influence of vasopressin and oxytocin secretion in this response during experimental septic shock. Importantly, the infusions were performed 6 h after the CLP surgery, as hypotension at this time has been suggested to be associated with low vasopressin secretion.[30]
The expansion of blood volume through isotonic infusion leads to an increase in several hemodynamic parameters, including central venous pressure, right atrial pressure, central blood volume, cardiac output, and stroke volume.[31] However, this process can cause a reduction in HR and arterial blood pressure decrease due to the large volume expansion.[32,33] The current study revealed that the administration of isotonic HES did not lead to an increase in blood pressure through volume expansion. However, a dosage of 16 mL/kg of HES resulted in an increase in oxytocin secretion. Notably, the cardiovascular response was not affected by the administration of an oxytocin antagonist before the infusion of HES. It is possible that the inefficacy of isotonic expansion with HES in restoring blood pressure during experimental septic shock is due to excessive production of nitric oxide, which causes vasodilation and increases vessel compliance, allowing for greater volume to occupy the vascular bed without increasing blood pressure.[34]
The infusion of hypertonic fluids has been shown to restore hemodynamic parameters and tissue perfusion in patients with severe sepsis.[3] These solutions offer a potential advantage due to their high osmolality, which facilitates the movement of tissue fluid into the intravascular space, thereby reducing tissue oedema for a given increase in plasma volume.[3,35,36] However, it is important to note that repeated administration of hypertonic fluids can result in electrolyte imbalances, such as excessive sodium levels and increased plasma osmolality, leading to volume overload, heart failure, and pulmonary oedema.[35,36] The addition of HES may prolong the increase in blood pressure by keeping water in the vascular space. In this study, we found that the prior injection of the V1 receptor antagonist prevented the increase in blood pressure, indicating that the V1 receptor, but not the oxytocin receptor, is necessary for the pressor response to HS-HES infusion during septic shock. This result highlights the significant role of vasopressin in the pressor effect observed in the HS-HES during the CLP model. Prior research has also shown that vasopressin plays an important role in the pressor response to hypertonic saline during endotoxic shock.[16] and the CLP model.[19] These findings suggest that during septic shock, the vascular space’s water retention capacity is insufficient to promote increased blood pressure, requiring a vasoconstrictor substance, such as vasopressin.
The late phase of septic shock is characterised by an inadequate reduction in plasma vasopressin levels relative to the severity of hypotension.[37,38] This decline in vasopressin levels can be observed in humans as early as 6 h after the diagnosis of septic shock, leading to a relative deficiency of vasopressin within 36 h. Vasopressin plays a critical role in maintaining arterial blood pressure during hypotension by exerting potent vasoconstrictor effects. However, unlike in cardiogenic and hypovolemic shock, the increase in vasopressin levels during established septic shock is not substantial. Septic shock is characterised by a transient early rise in blood vasopressin concentration, followed by a subsequent decrease to significantly low levels, which has been attributed to vasopressin deficiency.[37] Several mechanisms have been proposed to explain the reduction in serum vasopressin during sepsis, including the depletion of pituitary stores due to baroreceptor-mediated release, autonomic dysfunction, and the inhibitory effect of elevated nitric oxide release in the hypothalamus.[38] Therefore, our findings indicate that the inhibition of vasopressin secretion due to the drop in blood pressure is likely the primary cause of hormone secretion deficit during the last phase of septic shock. However, this inhibition does not affect pathways involved in the response to hyperosmolarity, as shown by the observed vasopressin secretory response after the infusion of hypertonic solution.
CONCLUSION
Our results demonstrate that the infusion of an isotonic blood volume expander during experimental septic shock is ineffective in restoring blood pressure due to blood vessel compliance. In contrast, the infusion of a hypertonic solution stimulates vasopressin secretion and can transiently restore blood pressure. The use of HES in clinical practice is still a controversial topic that requires further investigation. Although pre-clinical studies suggest that HES may have limited benefits in septic shock, the optimal situations for its use remain unclear.
Acknowledgments
Our sincere gratitude goes to Marina F Venâncio and José dos Reis Pereira for their outstanding technical assistance. We also appreciate Dr. José Antunes-Rodrigues from Universidade de São Paulo for availing laboratory facilities.
Author contributions
MBS contributed to the formulation and design of the study, data collection, analysis and interpretation of data, initial drafting of the manuscript, and critical revision of the manuscript for significant intellectual content. FCV and AG-P participated in the development and design of the study, data acquisition, data analysis, and interpretation, manuscript drafting, critical revision of the manuscript for substantial intellectual content, administrative, technical, or material backing, and supervising the study.
Ethical approval
The author(s) declare that they have taken the ethical approval from IRB/IEC.
Declaration of patient consent
The authors certify that they have obtained all appropriate consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; #308762/2017-7).
References
- The third international consensus definitions for sepsis and septic shock (Sepsis-3) JAMA. 2016;315:801-10.
- [CrossRef] [PubMed] [Google Scholar]
- The surviving sepsis campaign: basic/translational science research priorities. Crit Care Med. 2020;48:1217-32.
- [CrossRef] [PubMed] [Google Scholar]
- Acute haemodynamic effects of a hypertonic saline/dextran solution in stable patients with severe sepsis. Intensive Care Med. 2002;28:1574-81.
- [CrossRef] [PubMed] [Google Scholar]
- Protective roles of hydroxyethyl starch 130/0.4 in intestinal inflammatory response and oxidative stress after hemorrhagic shock and resuscitation in rats. Inflammation. 2009;32:71-82.
- [CrossRef] [PubMed] [Google Scholar]
- Norepinephrine potentiates the efficacy of volume expansion on mean systemic pressure in septic shock. Crit Care. 2021;25:302.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of fluid resuscitation on acute lung injury in a rat model of sepsis. Bratisl Lek Listy. 2021;122:280-6.
- [CrossRef] [PubMed] [Google Scholar]
- Executive summary: Surviving sepsis campaign: International guidelines for the management of sepsis and septic shock 2021. Crit Care Med. 2021;49:1974-82.
- [CrossRef] [Google Scholar]
- Use of hydroxyethyl starch in sepsis research: A systematic review with meta-analysis. Acta Anaesthesiol Scand. 2021;65:1355-64.
- [CrossRef] [PubMed] [Google Scholar]
- Colloids versus crystalloids for fluid resuscitation in critically ill people. Cochrane Database Syst Rev. 2018;8:CD000567.
- [CrossRef] [Google Scholar]
- Intravenous fluid therapy in sepsis. Nutr Clin Pract. 2022;37:990-1003.
- [CrossRef] [PubMed] [Google Scholar]
- Protocolised reduction of non-resuscitation fluids versus usual care in patients with septic shock (REDUSE): A protocol for a multicentre feasibility trial. BMJ Open. 2023;13:e065392.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of hemodynamic efficacy and safety of 6% hydroxyethylstarch 130/0.4 vs 0.9% NaCl fluid replacement in patients with severe sepsis: The CRYSTMAS study. Crit Care. 2012;16:94.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy and safety of early target-controlled plasma volume replacement with a balanced gelatine solution versus a balanced electrolyte solution in patients with severe sepsis/septic shock: Study protocol, design, and rationale of a prospective, randomized, controlled, double-blind, multicentric, international clinical trial: GENIUS-Gelatine use in ICU and sepsis. Trials. 2021;22:376.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med. 2004;350:2247-56.
- [CrossRef] [PubMed] [Google Scholar]
- Hypertonic/hyperoncotic fluid resuscitation after hemorrhagic shock in dogs. Anesth Analg. 1991;73:738-44.
- [CrossRef] [PubMed] [Google Scholar]
- Pressor response to fluid resuscitation in endotoxic shock: Involvement of vasopressin. Crit Care Med. 2009;37:2968-72.
- [CrossRef] [PubMed] [Google Scholar]
- Neuroendocrine control of body fluid metabolism. Physiol Rev. 2004;84:169-208.
- [CrossRef] [PubMed] [Google Scholar]
- Hypertonic-hyperoncotic solutions improve cardiac function in children after open-heart surgery. Pediatrics. 2006;118:e76-84.
- [CrossRef] [PubMed] [Google Scholar]
- Neurohypophyseal response to fluid resuscitation with hypertonic saline during septic shock in rats. Exp Physiol. 2013;98:556-63.
- [CrossRef] [PubMed] [Google Scholar]
- A novel hydroxyethyl starch (Voluven) for effective perioperative plasma volume substitution in cardiac surgery. Can J Anaesth. 2000;47:1207-15.
- [CrossRef] [PubMed] [Google Scholar]
- Hydroxyethyl starch 130/0.4 versus modified fluid gelatin for volume expansion in cardiac surgery patients: The effects on perioperative bleeding and transfusion needs. Anesth Analg. 2005;101:639-4.
- [CrossRef] [PubMed] [Google Scholar]
- Management of sepsis: Early resuscitation. Clin Chest Med. 2008;29:689-704, ix-x
- [CrossRef] [PubMed] [Google Scholar]
- Assessing the antidepressant-like effects of carbetocin, an oxytocin agonist, using a modification of the forced swimming test. Psychopharmacology (Berl). 2010;210:35-43.
- [CrossRef] [PubMed] [Google Scholar]
- Sepsis and septic shock--a review of laboratory models and a proposal. J Surg Res. 1980;29:189-201.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of plasma osmolality on pituitary-adrenal responses to corticotropin-releasing hormone and atrial natriuretic peptide changes in central diabetes insipidus. J Clin Endocrinol Metab. 1997;82:1243-7.
- [CrossRef] [Google Scholar]
- Hyponatremia in critically ill patients. Indian J Crit Care Med. 2014;18:83-7.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the novel hydroxyethylstarch 130/0.4 and hydroxyethylstarch 200/0.6 in brain-dead donor resuscitation on renal function after transplantation. Br J Anaesth. 2008;100:504-8.
- [CrossRef] [PubMed] [Google Scholar]
- Fluid resuscitation with hydroxyethyl starches in patients with sepsis is associated with an increased incidence of acute kidney injury and use of renal replacement therapy: A systematic review and meta-analysis of the literature. J Crit Care. 2014;29:7.e1-7.
- [CrossRef] [PubMed] [Google Scholar]
- Resuscitation fluid types in sepsis, surgical, and trauma patients: A systematic review and sequential network meta-analyses. Crit Care. 2020;24:693.
- [CrossRef] [PubMed] [Google Scholar]
- Neonatal endotoxin exposure changes neuroendrocine, cardiovascular function and mortality during polymicrobial sepsis in adult rats. Regul Pept. 2011;169:21-30.
- [CrossRef] [PubMed] [Google Scholar]
- Hemodynamics and plasma ANP (atrial natriuretic peptide) after acute blood volume expansion in normotensive and spontaneously hypertensive rats. Acta Physiol Scand. 1998;133:513-8.
- [CrossRef] [PubMed] [Google Scholar]
- Neurochemical brain groups activated after an isotonic blood volume expansion in rats. Neuroscience. 2005;133:493-505.
- [CrossRef] [PubMed] [Google Scholar]
- Oxytocin mediates atrial natriuretic peptide release and natriuresis after volume expansion in the rat. Proc Natl Acad Sci U S A. 1995;95:7902-6.
- [CrossRef] [PubMed] [Google Scholar]
- Nitric oxide and vascular reactivity in sepsis. Shock. 2008;30(Suppl 1):10-3.
- [CrossRef] [PubMed] [Google Scholar]
- Hypertonic resuscitation: Physiologic mechanisms and recommendations for trauma care. J Trauma. 2003;54:S89-99.
- [CrossRef] [PubMed] [Google Scholar]
- Medullary noradrenergic neurons mediate hemodynamic responses to osmotic and volume challenges. Front Physiol. 2021;12:649535.
- [CrossRef] [PubMed] [Google Scholar]
- Circulating vasopressin levels in septic shock. Crit Care Med. 2003;31:1752-8.
- [CrossRef] [PubMed] [Google Scholar]
- Neurohypophyseal dysfunction during septic shock. Endocr Metab Immune Disord Drug Targets. 2010;10:247-51.
- [CrossRef] [PubMed] [Google Scholar]




